
Ms-001 (2) Clinical Priv Form Ortho 2019
Ms-001 (2) Clinical Priv Form Ortho 2019
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Full Download Ebook Ebook PDF Lippincott Nursing Procedures 8th Edition PDFDocument41 pagesFull Download Ebook Ebook PDF Lippincott Nursing Procedures 8th Edition PDFdennis.reddout18698% (46)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ipi Nursing Part 1,2,3Document53 pagesIpi Nursing Part 1,2,3Noleen MckayNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ISMP198 Periop Guidelns FINALDocument29 pagesISMP198 Periop Guidelns FINALHIRANGERNo ratings yet
- Ms-001 (2) Clinical Priv Form Emergency 2019Document3 pagesMs-001 (2) Clinical Priv Form Emergency 2019Athira Rajan100% (2)
- Intermediate Math For Nurses NAME - WorkbookDocument7 pagesIntermediate Math For Nurses NAME - WorkbookRaniela MaeNo ratings yet
- Ms-001 (2) Clinical Priv Form Dental 2019Document4 pagesMs-001 (2) Clinical Priv Form Dental 2019Athira RajanNo ratings yet
- MS-001 (2) Clinical Priv Form Pediatrician 2019Document4 pagesMS-001 (2) Clinical Priv Form Pediatrician 2019Athira RajanNo ratings yet
- Ms-001 (2) Clinical Priv Form Ent2019Document5 pagesMs-001 (2) Clinical Priv Form Ent2019Athira RajanNo ratings yet
- MS-7 POLMS00 CP Revised 2019 - MOHDocument7 pagesMS-7 POLMS00 CP Revised 2019 - MOHAthira RajanNo ratings yet
- MS-001 (2) Clinical Priv Form Nephro 2019Document4 pagesMS-001 (2) Clinical Priv Form Nephro 2019Athira RajanNo ratings yet
- MS-001 (2) Clinical Priv Form Urology 2019Document4 pagesMS-001 (2) Clinical Priv Form Urology 2019Athira Rajan100% (1)
- Ms-001 (2) Clinical Privi Form Anesthesia 2019Document4 pagesMs-001 (2) Clinical Privi Form Anesthesia 2019Athira Rajan100% (1)
- Management of Maternal Anemia With Intravenous Iron SucroseDocument6 pagesManagement of Maternal Anemia With Intravenous Iron Sucroseprakhar dwivediNo ratings yet
- Pediatric Infusion StandardsDocument20 pagesPediatric Infusion StandardsJessica TorreglosaNo ratings yet
- Lactated RingersDocument3 pagesLactated RingersE100% (5)
- MIL Vol 4Document6 pagesMIL Vol 4garywall.ukNo ratings yet
- Intravenous Fluids: Balancing Solutions: Ewout J. HoornDocument8 pagesIntravenous Fluids: Balancing Solutions: Ewout J. HoornbagusNo ratings yet
- Неотложка 2022 НГИDocument61 pagesНеотложка 2022 НГИȜLaa AsHrafNo ratings yet
- Take One FC Preboards Np4Document19 pagesTake One FC Preboards Np4Yaehl SuarezNo ratings yet
- IV Meds in Volumetric Set C RationaleDocument2 pagesIV Meds in Volumetric Set C RationalePascal Marie IzhaqNo ratings yet
- Managing Immunoglobulin TherapyDocument1 pageManaging Immunoglobulin TherapySITTIE JOBAISAH TOMINAMAN ALINo ratings yet
- Lactated RingersDocument22 pagesLactated Ringerskiky_frakNo ratings yet
- Fao Report 2009Document833 pagesFao Report 2009Siti MariyamNo ratings yet
- AV Shunt-Brescia Cimino - EditDocument53 pagesAV Shunt-Brescia Cimino - EditYufriadi100% (1)
- Case 1 ICCU CHARTDocument107 pagesCase 1 ICCU CHARTMaria Charis Anne IndananNo ratings yet
- Chapter 38Document22 pagesChapter 38Tito, Stephen Gabriel, A.No ratings yet
- Assessment-Tool-For-Ambulance 2018 PDFDocument12 pagesAssessment-Tool-For-Ambulance 2018 PDFDerrick ChavezNo ratings yet
- PPT1 - Vice and Drug Education ControlDocument17 pagesPPT1 - Vice and Drug Education ControlMarianne GabrielNo ratings yet
- 41 (1) In-Process Revision - 1790 - Visual Inspection of InjectionsDocument10 pages41 (1) In-Process Revision - 1790 - Visual Inspection of InjectionsBudy WijiyantoNo ratings yet
- Drug Name Indication: Action: Mechanism of Action Classificatio N Adverse Effects Contraindications: Nursing ConsiderationsDocument2 pagesDrug Name Indication: Action: Mechanism of Action Classificatio N Adverse Effects Contraindications: Nursing ConsiderationsEsmareldah Henry SirueNo ratings yet
- AR07449 FloTrac Vig SetupGuide 1212aLRiPDocument2 pagesAR07449 FloTrac Vig SetupGuide 1212aLRiPandany0117No ratings yet
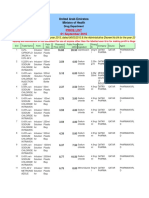
- MOH Medicines Price List For Official Use As On 1st of Sep 2016Document579 pagesMOH Medicines Price List For Official Use As On 1st of Sep 2016Sajitha SujeeshNo ratings yet
- Rigel Multi Flo Manual v2.7Document70 pagesRigel Multi Flo Manual v2.7RandhiMahardhika100% (1)
- Cerezyme of GenzymeDocument2 pagesCerezyme of GenzymeLakis Takis PapasNo ratings yet
- Intestinal Failure and Short Bowel SyndromeDocument5 pagesIntestinal Failure and Short Bowel SyndromesivaNo ratings yet
- NCM 109 B Skills Lab Manual IV InsertionDocument7 pagesNCM 109 B Skills Lab Manual IV InsertionRosevick BadocoNo ratings yet
- Hazards of IV TherapyDocument21 pagesHazards of IV TherapyFaraz Qurban RajperNo ratings yet
- Iv TherapyDocument11 pagesIv TherapyMarinill SolimanNo ratings yet













































































Download as doc, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Full Download Ebook Ebook PDF Lippincott Nursing Procedures 8th Edition PDFDocument41 pagesFull Download Ebook Ebook PDF Lippincott Nursing Procedures 8th Edition PDFdennis.reddout18698% (46)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ipi Nursing Part 1,2,3Document53 pagesIpi Nursing Part 1,2,3Noleen MckayNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ISMP198 Periop Guidelns FINALDocument29 pagesISMP198 Periop Guidelns FINALHIRANGERNo ratings yet
- Ms-001 (2) Clinical Priv Form Emergency 2019Document3 pagesMs-001 (2) Clinical Priv Form Emergency 2019Athira Rajan100% (2)
- Intermediate Math For Nurses NAME - WorkbookDocument7 pagesIntermediate Math For Nurses NAME - WorkbookRaniela MaeNo ratings yet
- Ms-001 (2) Clinical Priv Form Dental 2019Document4 pagesMs-001 (2) Clinical Priv Form Dental 2019Athira RajanNo ratings yet
- MS-001 (2) Clinical Priv Form Pediatrician 2019Document4 pagesMS-001 (2) Clinical Priv Form Pediatrician 2019Athira RajanNo ratings yet
- Ms-001 (2) Clinical Priv Form Ent2019Document5 pagesMs-001 (2) Clinical Priv Form Ent2019Athira RajanNo ratings yet
- MS-7 POLMS00 CP Revised 2019 - MOHDocument7 pagesMS-7 POLMS00 CP Revised 2019 - MOHAthira RajanNo ratings yet
- MS-001 (2) Clinical Priv Form Nephro 2019Document4 pagesMS-001 (2) Clinical Priv Form Nephro 2019Athira RajanNo ratings yet
- MS-001 (2) Clinical Priv Form Urology 2019Document4 pagesMS-001 (2) Clinical Priv Form Urology 2019Athira Rajan100% (1)
- Ms-001 (2) Clinical Privi Form Anesthesia 2019Document4 pagesMs-001 (2) Clinical Privi Form Anesthesia 2019Athira Rajan100% (1)
- Management of Maternal Anemia With Intravenous Iron SucroseDocument6 pagesManagement of Maternal Anemia With Intravenous Iron Sucroseprakhar dwivediNo ratings yet
- Pediatric Infusion StandardsDocument20 pagesPediatric Infusion StandardsJessica TorreglosaNo ratings yet
- Lactated RingersDocument3 pagesLactated RingersE100% (5)
- MIL Vol 4Document6 pagesMIL Vol 4garywall.ukNo ratings yet
- Intravenous Fluids: Balancing Solutions: Ewout J. HoornDocument8 pagesIntravenous Fluids: Balancing Solutions: Ewout J. HoornbagusNo ratings yet
- Неотложка 2022 НГИDocument61 pagesНеотложка 2022 НГИȜLaa AsHrafNo ratings yet
- Take One FC Preboards Np4Document19 pagesTake One FC Preboards Np4Yaehl SuarezNo ratings yet
- IV Meds in Volumetric Set C RationaleDocument2 pagesIV Meds in Volumetric Set C RationalePascal Marie IzhaqNo ratings yet
- Managing Immunoglobulin TherapyDocument1 pageManaging Immunoglobulin TherapySITTIE JOBAISAH TOMINAMAN ALINo ratings yet
- Lactated RingersDocument22 pagesLactated Ringerskiky_frakNo ratings yet
- Fao Report 2009Document833 pagesFao Report 2009Siti MariyamNo ratings yet
- AV Shunt-Brescia Cimino - EditDocument53 pagesAV Shunt-Brescia Cimino - EditYufriadi100% (1)
- Case 1 ICCU CHARTDocument107 pagesCase 1 ICCU CHARTMaria Charis Anne IndananNo ratings yet
- Chapter 38Document22 pagesChapter 38Tito, Stephen Gabriel, A.No ratings yet
- Assessment-Tool-For-Ambulance 2018 PDFDocument12 pagesAssessment-Tool-For-Ambulance 2018 PDFDerrick ChavezNo ratings yet
- PPT1 - Vice and Drug Education ControlDocument17 pagesPPT1 - Vice and Drug Education ControlMarianne GabrielNo ratings yet
- 41 (1) In-Process Revision - 1790 - Visual Inspection of InjectionsDocument10 pages41 (1) In-Process Revision - 1790 - Visual Inspection of InjectionsBudy WijiyantoNo ratings yet
- Drug Name Indication: Action: Mechanism of Action Classificatio N Adverse Effects Contraindications: Nursing ConsiderationsDocument2 pagesDrug Name Indication: Action: Mechanism of Action Classificatio N Adverse Effects Contraindications: Nursing ConsiderationsEsmareldah Henry SirueNo ratings yet
- AR07449 FloTrac Vig SetupGuide 1212aLRiPDocument2 pagesAR07449 FloTrac Vig SetupGuide 1212aLRiPandany0117No ratings yet
- MOH Medicines Price List For Official Use As On 1st of Sep 2016Document579 pagesMOH Medicines Price List For Official Use As On 1st of Sep 2016Sajitha SujeeshNo ratings yet
- Rigel Multi Flo Manual v2.7Document70 pagesRigel Multi Flo Manual v2.7RandhiMahardhika100% (1)
- Cerezyme of GenzymeDocument2 pagesCerezyme of GenzymeLakis Takis PapasNo ratings yet
- Intestinal Failure and Short Bowel SyndromeDocument5 pagesIntestinal Failure and Short Bowel SyndromesivaNo ratings yet
- NCM 109 B Skills Lab Manual IV InsertionDocument7 pagesNCM 109 B Skills Lab Manual IV InsertionRosevick BadocoNo ratings yet
- Hazards of IV TherapyDocument21 pagesHazards of IV TherapyFaraz Qurban RajperNo ratings yet
- Iv TherapyDocument11 pagesIv TherapyMarinill SolimanNo ratings yet