Download as pdf or txt
You might also like
- Laboratory Request FormDocument1 pageLaboratory Request FormEric Nagum100% (2)
- Certified True Copy StampDocument1 pageCertified True Copy StampChris-Goldie Lorezo100% (1)
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayNo ratings yet
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- UST NSTP Medical Examination Report FormDocument1 pageUST NSTP Medical Examination Report FormFrancisQueNo ratings yet
- Case Investigation Form Coronavirus Disease (COVID-19) : (Check All That Apply, Refer To Appendix 2)Document4 pagesCase Investigation Form Coronavirus Disease (COVID-19) : (Check All That Apply, Refer To Appendix 2)john dave rougel ManzanoNo ratings yet
- Bulletproof Confidence - The Art of Not Caring What People Think and Living Fearlessly by Patrick KingDocument117 pagesBulletproof Confidence - The Art of Not Caring What People Think and Living Fearlessly by Patrick KingChris-Goldie Lorezo100% (1)
- Therapeutics HandbookDocument49 pagesTherapeutics Handbookaasdf100% (1)
- Gapuz Maternal Health NursingDocument80 pagesGapuz Maternal Health NursingHayes Clover100% (6)
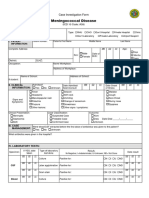
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- CIF-Meningococcal DiseaseDocument2 pagesCIF-Meningococcal DiseaseIvy marie BonNo ratings yet
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
- Cif AfpDocument2 pagesCif Afpninzah wanzahNo ratings yet
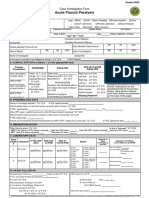
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormBarbie CincoNo ratings yet
- Case Investigation Form - Acute Flaccid ParalysisDocument2 pagesCase Investigation Form - Acute Flaccid Paralysisclaverialc10No ratings yet
- Afp 2013Document2 pagesAfp 2013rhu silagoNo ratings yet
- Zika IcifDocument2 pagesZika IcifMarav SymbNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- New Enhanced Zika CIFDocument3 pagesNew Enhanced Zika CIFMarav SymbNo ratings yet
- Sari FormsDocument3 pagesSari FormsJohnasse Sebastian NavalNo ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- RabiesDocument2 pagesRabiesninzah wanzahNo ratings yet
- CIF DiphDocument2 pagesCIF DiphIvy marie BonNo ratings yet
- CIF-MR 2022 Ver1Document2 pagesCIF-MR 2022 Ver1Ivy marie BonNo ratings yet
- Chikungunya FormDocument2 pagesChikungunya FormTin Causaren-Gertos100% (1)
- CIF MALARIA - Rev4 As July 4 2016 - LatestDocument3 pagesCIF MALARIA - Rev4 As July 4 2016 - LatestNicholai Cabaddu100% (2)
- Patient Document 2024Document5 pagesPatient Document 2024amunesu.kcNo ratings yet
- Yo G8 Nydqx CT1 MYWs U0 Ak 94 Pa VVTLG Ag LD8 JK ZXDN FXG Amva 7 T5 DVa CGwi Lxmy WP HT3 VFT6 OvuspoDocument4 pagesYo G8 Nydqx CT1 MYWs U0 Ak 94 Pa VVTLG Ag LD8 JK ZXDN FXG Amva 7 T5 DVa CGwi Lxmy WP HT3 VFT6 Ovusporehan302brandNo ratings yet
- Confidential Needlestick Sharps Injury or Exposure To Body Fluid Report Form v1 1Document2 pagesConfidential Needlestick Sharps Injury or Exposure To Body Fluid Report Form v1 1Kish BNo ratings yet
- NMC Case Notification Form NOTIFICATION PAGE v2 Final-Mar2018Document2 pagesNMC Case Notification Form NOTIFICATION PAGE v2 Final-Mar2018R TNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- Medical Admission Proforma: Hospital Name Patient DetailsDocument11 pagesMedical Admission Proforma: Hospital Name Patient DetailsAngelus129No ratings yet
- Labmgt Request FormDocument1 pageLabmgt Request Formferdinand carlosNo ratings yet
- V8 - ESR Verification Form - Revise - As of October 26Document3 pagesV8 - ESR Verification Form - Revise - As of October 26Faustine De GuzmanNo ratings yet
- ISEH Imaging Request Form 2019Document2 pagesISEH Imaging Request Form 2019Sarfraz LocusNo ratings yet
- SBI Life DEATH CLAIM FORMDocument4 pagesSBI Life DEATH CLAIM FORMCloudy ChefNo ratings yet
- DRI Elk Grove - BLANK Patient Information Form EnglishDocument2 pagesDRI Elk Grove - BLANK Patient Information Form EnglishKamal SahuNo ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Health Declaration FormDocument4 pagesHealth Declaration Formbrgyanos03No ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Travel Claim Form - Medical ExpensesDocument3 pagesTravel Claim Form - Medical Expensesshyamsundertripathi270No ratings yet
- Attending Physician's Statement For Proposed Insured/OwnerDocument2 pagesAttending Physician's Statement For Proposed Insured/OwnerSincerely ReynNo ratings yet
- History FormDocument5 pagesHistory FormYazeed AsrawiNo ratings yet
- Oral Health Form PregnantDocument1 pageOral Health Form PregnantAna TorresNo ratings yet
- Template HXDocument1 pageTemplate HXdawnNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- TRF For COVID-19 TEST (Coronavirus) : History Yes NoDocument1 pageTRF For COVID-19 TEST (Coronavirus) : History Yes NoRajendra ChavanNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Anexo 3 PEC-FormDocument2 pagesAnexo 3 PEC-FormdiogerNo ratings yet
- Department of OrthodonticsDocument2 pagesDepartment of OrthodonticsNauman ArshadNo ratings yet
- Print AdmissionDocument1 pagePrint Admissionthcimrd24No ratings yet
- CIF (For BMDL PhilHealth Purposes Only)Document1 pageCIF (For BMDL PhilHealth Purposes Only)BALIUAG DISTRICT LABORATORYNo ratings yet
- Clinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Document1 pageClinical Treatment Form: I DIAGNOSES (Must Be To The Highest Level of Specificity)Danielle YoderNo ratings yet
- Nigeria ART Program Evaluation Data Extraction TooDocument9 pagesNigeria ART Program Evaluation Data Extraction TooALEMAYEHU SHIFERAWNo ratings yet
- Medicalhistory 1Document2 pagesMedicalhistory 1nnma0127No ratings yet
- Pui FormDocument2 pagesPui FormBotez ElviraNo ratings yet
- TB Screening FormDocument2 pagesTB Screening Formkarlrcar.muntilguNo ratings yet
- Health Form A2Document2 pagesHealth Form A2Dane MagruderNo ratings yet
- Covid Bakuna Center RegistryDocument17 pagesCovid Bakuna Center RegistryChris-Goldie LorezoNo ratings yet
- AUTHENTIC SWEET AND SOUR by Sandy DazaDocument2 pagesAUTHENTIC SWEET AND SOUR by Sandy DazaChris-Goldie LorezoNo ratings yet
- Guidelines On Health Emergency Management Manual For PDFDocument173 pagesGuidelines On Health Emergency Management Manual For PDFChris-Goldie Lorezo100% (3)
- Teresita Jalandoni Provincial Hospital: Molecular LaboratoryDocument4 pagesTeresita Jalandoni Provincial Hospital: Molecular LaboratoryChris-Goldie LorezoNo ratings yet
- Philippine Red Cross Molecular Laboratory: Covid-19 RT-PCR Test Report & CertificationDocument1 pagePhilippine Red Cross Molecular Laboratory: Covid-19 RT-PCR Test Report & CertificationChris-Goldie LorezoNo ratings yet
- National EMS Week 2019 InvitationDocument2 pagesNational EMS Week 2019 InvitationChris-Goldie LorezoNo ratings yet
- Thunderbird Medication and Vaccination ProgramDocument1 pageThunderbird Medication and Vaccination ProgramChris-Goldie LorezoNo ratings yet
- IATF Advisory No. 1 Border Control FlowchartDocument4 pagesIATF Advisory No. 1 Border Control FlowchartChris-Goldie LorezoNo ratings yet
- 2020 Drug PricesDocument25 pages2020 Drug PricesChris-Goldie LorezoNo ratings yet
- Infection Control NurseDocument41 pagesInfection Control NurseChris-Goldie Lorezo100% (1)
- Oratio Imperata: Prayer Against COVID-19: Source: Catholic Bishops Conference of The PhilippinesDocument1 pageOratio Imperata: Prayer Against COVID-19: Source: Catholic Bishops Conference of The PhilippinesChris-Goldie LorezoNo ratings yet
- A Case Investigator's Guide For COVID-19: CDC - Gov/coronavirusDocument27 pagesA Case Investigator's Guide For COVID-19: CDC - Gov/coronavirusChris-Goldie LorezoNo ratings yet
- Workplace Incident Report TemplateDocument1 pageWorkplace Incident Report TemplateChris-Goldie LorezoNo ratings yet
- DAY 0 DAY 1 DAY 2 DAY 3 DAY 4 DAY 5: How To Use Your 14-Day LogDocument2 pagesDAY 0 DAY 1 DAY 2 DAY 3 DAY 4 DAY 5: How To Use Your 14-Day LogChris-Goldie LorezoNo ratings yet
- Timeline Urgent Conditions Following Disasters Other Conditions/Problems First 24 HrsDocument5 pagesTimeline Urgent Conditions Following Disasters Other Conditions/Problems First 24 HrsChris-Goldie LorezoNo ratings yet
- IYCF Counselling Cards ChildFundPCADocument34 pagesIYCF Counselling Cards ChildFundPCAChris-Goldie LorezoNo ratings yet
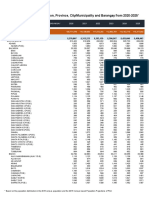
- 2015 Census-Based Population ProjectionsDocument685 pages2015 Census-Based Population ProjectionsChris-Goldie Lorezo100% (1)
- HEEADSSS Assessment Guide USUDocument11 pagesHEEADSSS Assessment Guide USUChris-Goldie LorezoNo ratings yet
- A Contact Tracer'S Guide For Covid-19: CDC - Gov/coronavirusDocument17 pagesA Contact Tracer'S Guide For Covid-19: CDC - Gov/coronavirusChris-Goldie LorezoNo ratings yet
- Isolation GuidelinesDocument203 pagesIsolation GuidelinesAlifia TrisnaningrumNo ratings yet
- Who HCV 2018Document108 pagesWho HCV 2018hendrawanNo ratings yet
- Zhan ZhuangDocument46 pagesZhan ZhuangAndrzej KaliszNo ratings yet
- Biology Matters 3rd EditionDocument272 pagesBiology Matters 3rd Editionotakukat763No ratings yet
- Term Paper On Air PollutionDocument5 pagesTerm Paper On Air PollutionaixgaoqifNo ratings yet
- SITXFSA001 Student Assessment TasksDocument24 pagesSITXFSA001 Student Assessment TasksMukta AktherNo ratings yet
- The Endocrine System:: Chemical Signals in AnimalsDocument13 pagesThe Endocrine System:: Chemical Signals in AnimalsbobNo ratings yet
- PHARCAL Abbreviations in RXDocument2 pagesPHARCAL Abbreviations in RXMiguel Santos0% (1)
- Short Notes and Short Cases in GynaecologyDocument163 pagesShort Notes and Short Cases in Gynaecologysalah subbahNo ratings yet
- Daftar Puastaka BaruuuDocument2 pagesDaftar Puastaka BaruuuEvan AninditoNo ratings yet
- NCP Risk For Infection TuberculosisDocument3 pagesNCP Risk For Infection TuberculosisWen SilverNo ratings yet
- Elder Abuse: by Julie A. Fusco, Pharm.D., BCPS, CGPDocument18 pagesElder Abuse: by Julie A. Fusco, Pharm.D., BCPS, CGPAnonymous hF5zAdvwCC100% (3)
- Krissa and Drentlaw Visual Acuity The Critical Measure!Document18 pagesKrissa and Drentlaw Visual Acuity The Critical Measure!Jolien WalravenNo ratings yet
- Eclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Document20 pagesEclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Grigore PopaNo ratings yet
- Veterinary MedicineDocument2 pagesVeterinary MedicineAmir 1No ratings yet
- ACOG Guidelines For Exercise During PregnancyDocument13 pagesACOG Guidelines For Exercise During Pregnancypptscribid100% (1)
- Preventive Care: Female Checklist - UnitedHealthcareDocument3 pagesPreventive Care: Female Checklist - UnitedHealthcareLiz MNo ratings yet
- Charcot-Marie-Tooth DiseaseDocument2 pagesCharcot-Marie-Tooth DiseaseitsmeayaeNo ratings yet
- Unit 3 AtherosclerosisDocument29 pagesUnit 3 AtherosclerosisJack TomarNo ratings yet
- History of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedDocument3 pagesHistory of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedVicente BaltazarNo ratings yet
- Cholelithiasis in Infants, Children, and Adolescents: George W. Holcomb, JR, MD, and George W. Holcomb, In, MDTDocument9 pagesCholelithiasis in Infants, Children, and Adolescents: George W. Holcomb, JR, MD, and George W. Holcomb, In, MDTangelaanapakuNo ratings yet
- Scopus Database Journal 02 NovDocument25 pagesScopus Database Journal 02 Novnaresh kotraNo ratings yet
- Blood DonationDocument15 pagesBlood DonationperllyNo ratings yet
- Chapter 36 Death Study GuideDocument25 pagesChapter 36 Death Study GuideDaniel McVayNo ratings yet
- Kidney Introduction PDF 508Document10 pagesKidney Introduction PDF 508Shailesh DixitNo ratings yet
- Telemedicine in Rural KenyaDocument6 pagesTelemedicine in Rural KenyaKamau GabrielNo ratings yet
- Tarun MeenaDocument59 pagesTarun Meenapiyushjakhar05No ratings yet
- MD LogbookDocument47 pagesMD LogbookAhmad fayazNo ratings yet