Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
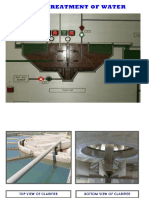
- Pre-Treatmentof WaterDocument18 pagesPre-Treatmentof WaterYoussef DaoudNo ratings yet
- Developing Professionals For The Lifting Equipment IndustryDocument199 pagesDeveloping Professionals For The Lifting Equipment IndustryYoussef DaoudNo ratings yet
- Ap 01-21: Pilot Water Disposal System For Main Station at Tibisti Field Request of ClarificationDocument3 pagesAp 01-21: Pilot Water Disposal System For Main Station at Tibisti Field Request of ClarificationYoussef DaoudNo ratings yet
- Ap01 21Document9 pagesAp01 21Youssef DaoudNo ratings yet
- Pathophysiology of Primary Cataract: Saint Paul University Dumaguete College of Nursing S.Y. 2021-2022Document3 pagesPathophysiology of Primary Cataract: Saint Paul University Dumaguete College of Nursing S.Y. 2021-2022zoie ziazzetteNo ratings yet
- School Form 8 (SF 8)Document2 pagesSchool Form 8 (SF 8)Mike DelivaNo ratings yet
- A Case Study Submitted in Partial Fulfilment of The Requirements in Capstone ProjectDocument5 pagesA Case Study Submitted in Partial Fulfilment of The Requirements in Capstone Projectedison savellanoNo ratings yet
- Fit To Work Certificate DocxDocument3 pagesFit To Work Certificate DocxBlood ViernesNo ratings yet
- World Wide: PhilippinesDocument2 pagesWorld Wide: PhilippinesGuile RilleraNo ratings yet
- NGCM 112 Course OutlineDocument7 pagesNGCM 112 Course OutlineAYTONA, JAMAICA F.No ratings yet
- 3descriptive EpidemiologyDocument49 pages3descriptive EpidemiologyAnusha VergheseNo ratings yet
- Down Syndrome: PDFDocument70 pagesDown Syndrome: PDFSharafuddin SalimiNo ratings yet
- IJCRT23A5059Document9 pagesIJCRT23A5059Agus SunardiNo ratings yet
- PHE Complete Immunisation Schedule Jan2020 PDFDocument2 pagesPHE Complete Immunisation Schedule Jan2020 PDFJyotirmaya RajaNo ratings yet
- Dapus AbrorDocument2 pagesDapus AbrorZulfitrawatiNo ratings yet
- Phlegmon: Signs and SymptomDocument4 pagesPhlegmon: Signs and SymptomFadly RizkyNo ratings yet
- Haq - Myastenia GravisDocument1 pageHaq - Myastenia GravisArinal HaqNo ratings yet
- Prevalence of Cardiovascular Risk Factors Among Workers at A Private Tertiary Center in AngolaDocument7 pagesPrevalence of Cardiovascular Risk Factors Among Workers at A Private Tertiary Center in AngolaMilton J. Samuel MateusNo ratings yet
- Pancreatic Adenocarcinoma: Albumin-Bound Paclitaxel/GemcitabineDocument1 pagePancreatic Adenocarcinoma: Albumin-Bound Paclitaxel/GemcitabineJaneNo ratings yet
- Case No. 3Document3 pagesCase No. 3Rialyn PontillasNo ratings yet
- Crohn DiseaseDocument2 pagesCrohn DiseaseFiraFurqaniNo ratings yet
- PertussisDocument1 pagePertussisapi-350983586No ratings yet
- 1 Drug Study - DexamethasoneDocument6 pages1 Drug Study - DexamethasoneJohn100% (1)
- Peripheral NeuropathyDocument16 pagesPeripheral NeuropathyKhaled OssamaNo ratings yet
- Primer On Allergic and Immunologic Deseases Part 2Document3 pagesPrimer On Allergic and Immunologic Deseases Part 2ponbohacopNo ratings yet
- Preeclampsia With HELLP SyndromeDocument8 pagesPreeclampsia With HELLP SyndromeWely Tiffani YpNo ratings yet
- Drug Addiction: By: Ralph Berganio Abeygail Jimenez Maria Jasmine Maala Arleen Rose Roxas Margareth CortezDocument9 pagesDrug Addiction: By: Ralph Berganio Abeygail Jimenez Maria Jasmine Maala Arleen Rose Roxas Margareth CortezRikka TakanashiNo ratings yet
- Interview - Test - Educazione ServiziDocument4 pagesInterview - Test - Educazione ServiziRounak BasuNo ratings yet
- The Role of Social Media inDocument16 pagesThe Role of Social Media inSaba TahseenNo ratings yet
- Croft On ScoreDocument1 pageCroft On ScoreGalaleldin AliNo ratings yet
- Patient Medication Management: DRUG STUDY University of Cebu Medical CenterDocument1 pagePatient Medication Management: DRUG STUDY University of Cebu Medical CenterMemcom SolutionNo ratings yet
- March 2019 Issue of Clinics in Dermatology PDFDocument71 pagesMarch 2019 Issue of Clinics in Dermatology PDFcuteNo ratings yet
- Tibbi Terimler Ve KisaltmalarDocument2 pagesTibbi Terimler Ve KisaltmalarDilara IrakNo ratings yet
- Vol 26 1 2018 15Document10 pagesVol 26 1 2018 15sind badNo ratings yet