Download as docx, pdf, or txt
You might also like
- Counselling in Different Settings Maggie ReidDocument183 pagesCounselling in Different Settings Maggie ReidFaten Salah50% (4)
- Instructor's Manual For COUNSELING & PSYCHOTHERAPY THEORIES: IN CONTEXT AND PRACTICEDocument172 pagesInstructor's Manual For COUNSELING & PSYCHOTHERAPY THEORIES: IN CONTEXT AND PRACTICEherbalizer3392% (12)
- Pete Sanders Counselling For DepressionDocument17 pagesPete Sanders Counselling For DepressionFOCUS Psicología y PsicoterapiaNo ratings yet
- Beck's Cognitive TheoryDocument14 pagesBeck's Cognitive TheoryFatima Asim 922-FSS/BSPSY/F17No ratings yet
- Working at Relational Depth in Counselling and Psychotherapy - Dave MearnsDocument5 pagesWorking at Relational Depth in Counselling and Psychotherapy - Dave Mearnsjyjamewy33% (3)
- Dave Mearns - Person-Centred Therapy - A Leading EdgeDocument128 pagesDave Mearns - Person-Centred Therapy - A Leading EdgeBotezat-AntonescuRaduAndrei100% (2)
- Person CentredDocument13 pagesPerson CentredRenan Antunes100% (1)
- Conceptualization and Treatment Plan1Document11 pagesConceptualization and Treatment Plan1Leah WoodardNo ratings yet
- CBT EssayDocument16 pagesCBT EssayCristín Ní LiatháinNo ratings yet
- The Gloria FilmsDocument3 pagesThe Gloria Filmssalbina arabiNo ratings yet
- Counseling Treatment PlanDocument2 pagesCounseling Treatment PlanArhann Anthony Almachar Adriatico100% (1)
- Person Centred TheoryDocument7 pagesPerson Centred TheoryWendy Tate100% (2)
- Client Centered TherapyDocument8 pagesClient Centered TherapyIqbal BaryarNo ratings yet
- Introduction to Attachment Theory in Practice: Unveiling the Power of Emotionally Focused Therapy (EFT) for Individuals, Couples, and Families.From EverandIntroduction to Attachment Theory in Practice: Unveiling the Power of Emotionally Focused Therapy (EFT) for Individuals, Couples, and Families.No ratings yet
- Different Schools of PsychotherapyDocument10 pagesDifferent Schools of PsychotherapysanaNo ratings yet
- Pre TherapyDocument11 pagesPre TherapyВладимир ДудкинNo ratings yet
- Emotion-Focused Therapy: A Summary and Overview DR Leslie GreenbergDocument26 pagesEmotion-Focused Therapy: A Summary and Overview DR Leslie GreenbergRichiNo ratings yet
- The Case Formulation Approach To Psychotherapy Research RevisitedDocument22 pagesThe Case Formulation Approach To Psychotherapy Research Revisitedferreira.pipe3240No ratings yet
- Evaluating The Effectiveness of A Scholl-Based CounsellingDocument14 pagesEvaluating The Effectiveness of A Scholl-Based Counsellingjanettst2100% (1)
- The Role of Clinical SupervisionDocument7 pagesThe Role of Clinical Supervisionsethiee100% (1)
- What Is Counselling and Psychotherapy - (Counselling and Psychotherapy Practice) (PDFDrive)Document209 pagesWhat Is Counselling and Psychotherapy - (Counselling and Psychotherapy Practice) (PDFDrive)KarmenNo ratings yet
- Topic 9 Counselling in A Multicultural SocietyDocument35 pagesTopic 9 Counselling in A Multicultural SocietyQuen MieraNo ratings yet
- The Cork Person Centred Gestalt Project PDFDocument18 pagesThe Cork Person Centred Gestalt Project PDFevgeniiNo ratings yet
- Emotion Focused Therapy For Generalized Anxiety Intro SampleDocument14 pagesEmotion Focused Therapy For Generalized Anxiety Intro SamplemoizNo ratings yet
- Types of Brief Psychodynamic TherapyDocument2 pagesTypes of Brief Psychodynamic TherapyJasroop MahalNo ratings yet
- The Therapeutic Alliance, Ruptures, and Session-by-Session FeedbackDocument225 pagesThe Therapeutic Alliance, Ruptures, and Session-by-Session FeedbackJorge Rojas GNo ratings yet
- Introduction To Brief Therapy PDFDocument43 pagesIntroduction To Brief Therapy PDFrimpa29No ratings yet
- Counselling - Case Study Assignment 3Document11 pagesCounselling - Case Study Assignment 3Ryan ƁoŋŋęrNo ratings yet
- Comparing Different Approaches To CounsellingDocument7 pagesComparing Different Approaches To CounsellingTim RichardsonNo ratings yet
- Applications of Theory To Rehabilitation Counselling PracticDocument49 pagesApplications of Theory To Rehabilitation Counselling PracticShahinNo ratings yet
- Online Counselling AgreementDocument6 pagesOnline Counselling AgreementFairy AngelNo ratings yet
- Therapists Guide To Brief CBTManua2l PDFDocument111 pagesTherapists Guide To Brief CBTManua2l PDFbgvtNo ratings yet
- 2020 Handbook Master of Narrative Therapy and Community WorkDocument31 pages2020 Handbook Master of Narrative Therapy and Community Worknicolas mossoNo ratings yet
- Change Process Research in PsychotherapyDocument19 pagesChange Process Research in PsychotherapyJuanaNo ratings yet
- PSY1021 Foundation Counselling Skills Essay 1 Cover SheetDocument11 pagesPSY1021 Foundation Counselling Skills Essay 1 Cover SheetGRACE ON SPILL100% (1)
- Harlene Anderson: Postmodern Collaborative and Person-Centred Therapies: What Would Carl Rogers Say?Document22 pagesHarlene Anderson: Postmodern Collaborative and Person-Centred Therapies: What Would Carl Rogers Say?Alan MuñozNo ratings yet
- Personal Theory Reality TherapyDocument18 pagesPersonal Theory Reality Therapyapi-285903956100% (1)
- Gestalt FinalDocument25 pagesGestalt FinalDeeksha WaliaNo ratings yet
- What Is Humanistic CounsellingDocument9 pagesWhat Is Humanistic CounsellingSankalp JainNo ratings yet
- Counselling Skills - Reflective EssayDocument3 pagesCounselling Skills - Reflective EssayConnor Jefferies100% (1)
- Young People Hearing Voices FinalDocument28 pagesYoung People Hearing Voices Finalapi-247002951No ratings yet
- Acceptance and Commitment Therapy ModelDocument31 pagesAcceptance and Commitment Therapy ModelSusana FossaNo ratings yet
- The Therapeutic Alliance in Couples and Family TherapyDocument10 pagesThe Therapeutic Alliance in Couples and Family TherapySophiez0257No ratings yet
- Compare & Contrast The Behaviourist and Psychodynamic Approaches in Psychology. Paying Particular Attention To Conceptual & Methodological DifferencesDocument4 pagesCompare & Contrast The Behaviourist and Psychodynamic Approaches in Psychology. Paying Particular Attention To Conceptual & Methodological DifferencesKate Orange0% (1)
- SupervisionDocument445 pagesSupervisionCristina BadeaNo ratings yet
- Counselling TheoriesDocument15 pagesCounselling TheoriesPranavi KhandekarNo ratings yet
- Developing and Using A Case FormulationDocument9 pagesDeveloping and Using A Case FormulationSimona MoscuNo ratings yet
- Gestalt TherapyDocument19 pagesGestalt TherapyAngeline NaronNo ratings yet
- Narrative TherapyDocument9 pagesNarrative TherapyChristl GrtnNo ratings yet
- A Secure Base: Theoretical Context and OverviewDocument4 pagesA Secure Base: Theoretical Context and Overviewmadelaine_g1No ratings yet
- Cultivating Online Therapeutic Presence Strengthening Therapeutic Relationships in Teletherapy SessionsDocument18 pagesCultivating Online Therapeutic Presence Strengthening Therapeutic Relationships in Teletherapy SessionsMaRice Mar Rice100% (1)
- Men in TherapyDocument47 pagesMen in TherapyMarilena JuncuNo ratings yet
- Narrative TherapyDocument18 pagesNarrative TherapyLalaine Sarno100% (1)
- Family Systems TherapyDocument37 pagesFamily Systems TherapyMISTAcare67% (6)
- Ego StateDocument5 pagesEgo Stateptanoy8No ratings yet
- Solution Focused Counseling With Nvoluntary ClientsDocument13 pagesSolution Focused Counseling With Nvoluntary ClientsJuanaNo ratings yet
- The Basic Conditions, According To Carl Rogers, For The Development of A Good Counseling Relationship and Their Relationship With Counseling SkillsDocument7 pagesThe Basic Conditions, According To Carl Rogers, For The Development of A Good Counseling Relationship and Their Relationship With Counseling SkillsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cultural Adaptations of CBT A Summary and Discussion of The Special Issue On Cultural Adaptation of CBTDocument20 pagesCultural Adaptations of CBT A Summary and Discussion of The Special Issue On Cultural Adaptation of CBTKnud PedersenNo ratings yet
- Dokumen - Pub - Emotionally Focused Therapy For Couples 0898627303 0898621534Document250 pagesDokumen - Pub - Emotionally Focused Therapy For Couples 0898627303 0898621534Fernanda RuteNo ratings yet
- Theories of Counseling Object Relations TheoryDocument18 pagesTheories of Counseling Object Relations TheoryYoga UpasanaNo ratings yet
- Reflective Listening As A Counselling SkillDocument5 pagesReflective Listening As A Counselling Skillapi-240251499No ratings yet
- Transference and Counter TransferenceDocument10 pagesTransference and Counter TransferenceSajal SahooNo ratings yet
- Hypnosis BrochureDocument4 pagesHypnosis BrochuresrikanthvelagaNo ratings yet
- Attachment Theory and Child Abuse PDFDocument7 pagesAttachment Theory and Child Abuse PDFAlan ChallonerNo ratings yet
- CBT Course AnswersDocument34 pagesCBT Course AnswersAvinash ShenoyNo ratings yet
- Ijhbr January 2018 11-16Document6 pagesIjhbr January 2018 11-16Chinni ChinnaNo ratings yet
- Gestalt & Behavioral TherapyDocument4 pagesGestalt & Behavioral TherapyZaib RehmanNo ratings yet
- Psycocutaneous DiseaseDocument13 pagesPsycocutaneous DiseaseLaras KinasihNo ratings yet
- Asperger Jurnallll Dan AdhdDocument3 pagesAsperger Jurnallll Dan Adhdzakiah ulyaNo ratings yet
- 1987, Andrew Steptoe - Stage Fright in Orchestral Musicians A Study of Cognitive and BehaviouralDocument9 pages1987, Andrew Steptoe - Stage Fright in Orchestral Musicians A Study of Cognitive and BehaviouralEko A. SaputroNo ratings yet
- Clock Drawing TestDocument3 pagesClock Drawing TestNeny PatrowNo ratings yet
- Psychopathologies and Their TreatmentsDocument47 pagesPsychopathologies and Their TreatmentsLuther BlissettNo ratings yet
- Standards For Psychotherapy: 2010, College of Occupational Therapists of OntarioDocument36 pagesStandards For Psychotherapy: 2010, College of Occupational Therapists of OntariomkecikNo ratings yet
- Psychometric Properties of The Spanish Version of The Obsessive-Compulsive Inventory - Revised in A Non-Clinical SampleDocument11 pagesPsychometric Properties of The Spanish Version of The Obsessive-Compulsive Inventory - Revised in A Non-Clinical SampleJulia DGNo ratings yet
- Conversion Disorder (Dissociative Disorder) : Behavioral CharacteristicDocument5 pagesConversion Disorder (Dissociative Disorder) : Behavioral CharacteristicBhima DewanNo ratings yet
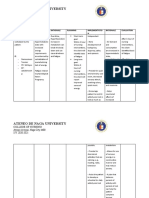
- Ateneo de Naga University: College of NursingDocument4 pagesAteneo de Naga University: College of NursingRenie SerranoNo ratings yet
- What Is An Eating DisorderDocument2 pagesWhat Is An Eating Disorderthurai_rajaNo ratings yet
- Mental Status Examination - Checklist1Document2 pagesMental Status Examination - Checklist1Reihann N. EdresNo ratings yet
- Perfect Day CollageDocument2 pagesPerfect Day Collageapi-541744798No ratings yet
- Evidence Graphic OrganizerDocument4 pagesEvidence Graphic Organizerapi-543670197No ratings yet
- Louis B. Schlesinger PDFDocument7 pagesLouis B. Schlesinger PDFMaksim PlebejacNo ratings yet
- Improving Self-Esteem Module 9 of 9Document10 pagesImproving Self-Esteem Module 9 of 9valeria_kendall6388100% (2)
- Psychiatric Nursing2 Questions)Document6 pagesPsychiatric Nursing2 Questions)Pamela MagsajoNo ratings yet
- Anxiety DisordersDocument37 pagesAnxiety DisordersDr Dushyant Kamal Dhari75% (4)
- A Comparison of Two Methods For Reducing Test-Anxiety and Improving Academic PerformanceDocument11 pagesA Comparison of Two Methods For Reducing Test-Anxiety and Improving Academic PerformanceGlobal Research and Development ServicesNo ratings yet
- ParanoiaDocument3 pagesParanoiatrinigalNo ratings yet
- Abnormal Psychology Midterm NotesDocument22 pagesAbnormal Psychology Midterm NotesAllana Ruth P. AbudaNo ratings yet
- Counseling TechniquesDocument2 pagesCounseling TechniquesCZar Ry NaNo ratings yet
- Bdi - IiDocument4 pagesBdi - IifosterbalaNo ratings yet
- List PDFDocument68 pagesList PDFParul SehgalNo ratings yet