Download as pdf or txt
You might also like
- Non-Invasive Evaluation of Human Brain Fluid Dynamics and Skull ...Document108 pagesNon-Invasive Evaluation of Human Brain Fluid Dynamics and Skull ...AlicjaNo ratings yet
- TBDY 2018 EnglishDocument608 pagesTBDY 2018 EnglishaygunbayramNo ratings yet
- Distribution Pattern of The Superior and Inferior Labial Arteries Impact For Safe Upper and Lower Lip Augmentation ProceduresDocument8 pagesDistribution Pattern of The Superior and Inferior Labial Arteries Impact For Safe Upper and Lower Lip Augmentation ProceduresLizeth Conde Orozco100% (1)
- The British Student's Guide To Obtaining Your Visa To Study at The Islamic University of Madinah v.2Document76 pagesThe British Student's Guide To Obtaining Your Visa To Study at The Islamic University of Madinah v.2Nouridine El KhalawiNo ratings yet
- Haematology - An Illustrated Colour Text, 4th Edition - 2Document132 pagesHaematology - An Illustrated Colour Text, 4th Edition - 2蔡季霖100% (1)
- XIAOMIDocument10 pagesXIAOMISrinath Saravanan75% (4)
- Normal Variant AortaDocument19 pagesNormal Variant AortaNyoman Ririn Chandrika SariNo ratings yet
- Nihms 1745044Document42 pagesNihms 1745044stevenburrow06No ratings yet
- Blood ThesisDocument8 pagesBlood Thesispamelasmithlittlerock100% (2)
- Synopsis Presentation 1Document11 pagesSynopsis Presentation 1Tejasvi ChavdaNo ratings yet
- Moffat 1996Document6 pagesMoffat 1996vernadskyiNo ratings yet
- The Hematopoietic System in The Context of Regenerative MedicineDocument19 pagesThe Hematopoietic System in The Context of Regenerative MedicineAlbert FBNo ratings yet
- 10 1016@j Ajog 2019 07 010 PDFDocument13 pages10 1016@j Ajog 2019 07 010 PDFDaniel GamarraNo ratings yet
- J Jpurol 2016 04 033Document17 pagesJ Jpurol 2016 04 033Audhrey BNo ratings yet
- Kaufmann-2004-Aspects of Human Fetoplacental V PDFDocument13 pagesKaufmann-2004-Aspects of Human Fetoplacental V PDFNguyễn Cao VânNo ratings yet
- Literature Review Stem Cell ResearchDocument4 pagesLiterature Review Stem Cell Researchea44a6t7100% (1)
- Building A Pulmonary Embolism Lysis Practice: Cover StoryDocument4 pagesBuilding A Pulmonary Embolism Lysis Practice: Cover Storydtech2No ratings yet
- Patogenesis Pleomorphic AdenomaDocument6 pagesPatogenesis Pleomorphic AdenomaYeni PuspitasariNo ratings yet
- Review: Shashikant L. SholapurkarDocument13 pagesReview: Shashikant L. SholapurkarFitria Ayu AnggrainiNo ratings yet
- Hipofisis 5Document33 pagesHipofisis 5RafaelPetitNo ratings yet
- Severe Preeclampsia Is Associated With Alterations in Cytotrophoblasts of The Smooth ChorionDocument64 pagesSevere Preeclampsia Is Associated With Alterations in Cytotrophoblasts of The Smooth ChorionRicvan Dana Nindrea,MKesNo ratings yet
- A Case of A Femoro Femoral Bypass FFB - An Instructi - 2021 - Translational ResDocument6 pagesA Case of A Femoro Femoral Bypass FFB - An Instructi - 2021 - Translational ResSơn VõNo ratings yet
- Research and Publication Ethics: What Have We Learned Thus Far?Document3 pagesResearch and Publication Ethics: What Have We Learned Thus Far?Jose ContrerasNo ratings yet
- A Pre Experimental Study To Assess The Effectiveness of STP On Knowledge Regarding Umbilical Cord Blood Banking Among Nursing Students at Selected Areas in JammuDocument6 pagesA Pre Experimental Study To Assess The Effectiveness of STP On Knowledge Regarding Umbilical Cord Blood Banking Among Nursing Students at Selected Areas in JammuEditor IJTSRDNo ratings yet
- Baker 6Document28 pagesBaker 6Ramadhan Maulana RizalNo ratings yet
- Ross2007 Abs AjogDocument2 pagesRoss2007 Abs AjogAbdillah FauziNo ratings yet
- Abbott2018 Article TheRoleOfBrainBarriersInFluidMDocument21 pagesAbbott2018 Article TheRoleOfBrainBarriersInFluidMAhmad Al-Husain100% (1)
- Loop Vs DividedDocument8 pagesLoop Vs DividedNatalindah Jokiem Woecandra T. D.No ratings yet
- Cerebellar Ataxia: Pathophysiology and RehabilitationDocument24 pagesCerebellar Ataxia: Pathophysiology and RehabilitationNistara Singh ChawlaNo ratings yet
- Failure of Physiological Transformation and SpiralDocument12 pagesFailure of Physiological Transformation and SpiralEcaterina Sorto de ArgeñalNo ratings yet
- Thesis On Congenital Heart DiseaseDocument4 pagesThesis On Congenital Heart Diseasegowlijxff100% (2)
- Histology: A Text and Atlas: January 1995Document3 pagesHistology: A Text and Atlas: January 1995Roxana RaduNo ratings yet
- Shuey, 2005Document2 pagesShuey, 2005Ruth WibowoNo ratings yet
- Management of Suprasellar Arachnoid Cysts in Children A Systematic Literature Review Highlighting Modern Endoscopic Approaches, 2020Document15 pagesManagement of Suprasellar Arachnoid Cysts in Children A Systematic Literature Review Highlighting Modern Endoscopic Approaches, 2020CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- Optimal Chest Drain Size - The Rise of The Small-Bore Pleural CatheterDocument9 pagesOptimal Chest Drain Size - The Rise of The Small-Bore Pleural CatheterRayCassidyNo ratings yet
- Califmed00115 0132cDocument1 pageCalifmed00115 0132csyntacs skNo ratings yet
- Dissertation Blood TransfusionDocument4 pagesDissertation Blood TransfusionAcademicPaperWritersTucson100% (1)
- Disproporsi Kepala PanggulDocument14 pagesDisproporsi Kepala PanggulIntan PermataNo ratings yet
- The Lyblpiilatlc Ip of Thsbody of THB Ijtybbvep A Study of 420 NecropsiesDocument19 pagesThe Lyblpiilatlc Ip of Thsbody of THB Ijtybbvep A Study of 420 NecropsiesWendy MarquezNo ratings yet
- HydrocephalusDocument9 pagesHydrocephalusDeby AnditaNo ratings yet
- Fresh Embryo Transfer vs. Frozen Embryo Transfer in in Vitro Fertilization Cycles: A Systematic Review and Meta-AnalysisDocument8 pagesFresh Embryo Transfer vs. Frozen Embryo Transfer in in Vitro Fertilization Cycles: A Systematic Review and Meta-AnalysisSri HariNo ratings yet
- Placenta in PreeclampsiaDocument20 pagesPlacenta in PreeclampsiaRania MousaNo ratings yet
- 1 s2.0 S141335552300014X MainDocument11 pages1 s2.0 S141335552300014X MainFirmansyah PurwantoNo ratings yet
- Seminar: Daniel J Penny, G Wesley Vick IIIDocument10 pagesSeminar: Daniel J Penny, G Wesley Vick IIIMuhammadAldoGiansyahNo ratings yet
- Umbilical Cord Accidents and Legal Implications Edit 14Document6 pagesUmbilical Cord Accidents and Legal Implications Edit 14DanNo ratings yet
- Clinical Anatomy - 2021 - Koziej - Termination Points of The Facial Artery A Meta AnalysisDocument8 pagesClinical Anatomy - 2021 - Koziej - Termination Points of The Facial Artery A Meta AnalysisOncología CdsNo ratings yet
- 18Document4 pages18Asrie Sukawatie PutrieNo ratings yet
- Evolution of The Human Pelvis and Obstructed Labor - 2019Document14 pagesEvolution of The Human Pelvis and Obstructed Labor - 2019residentesmihgz112023.2024No ratings yet
- The Anatomical Record - 2014 - Anderson - The Development of Septation in The Four Chambered HeartDocument16 pagesThe Anatomical Record - 2014 - Anderson - The Development of Septation in The Four Chambered HeartMarcelo BarberoNo ratings yet
- The New ICP Minimally Invasive Method Shows That The Monro-Kellie Doctrine Is Not ValidDocument4 pagesThe New ICP Minimally Invasive Method Shows That The Monro-Kellie Doctrine Is Not ValidEugenia AlmeidaNo ratings yet
- Paper Alumnos 6Document12 pagesPaper Alumnos 6Victor Martinez HagenNo ratings yet
- Withholding Feeds and Transfusion-Associated Necrotizing Enterocolitis in Preterm Infants: A Systematic ReviewDocument6 pagesWithholding Feeds and Transfusion-Associated Necrotizing Enterocolitis in Preterm Infants: A Systematic ReviewrezkyfikriNo ratings yet
- Pleural Disease NEJM 2018 PDFDocument12 pagesPleural Disease NEJM 2018 PDFPanayiotis StavroulakisNo ratings yet
- Stem Cell Research Literature ReviewDocument6 pagesStem Cell Research Literature Reviewafmzfgmwuzncdj100% (1)
- The Bone Marrow Niche For Haematopoietic Stem CellsDocument21 pagesThe Bone Marrow Niche For Haematopoietic Stem CellsHitomi-No ratings yet
- 1 s2.0 S0039610903001191 MainDocument15 pages1 s2.0 S0039610903001191 MainJuan Jos� Beltr�n Hern�ndezNo ratings yet
- Beyond Cord Clamping. Complexities of Umbilical Cord Management After BirthDocument5 pagesBeyond Cord Clamping. Complexities of Umbilical Cord Management After Birthnathalia_pastasNo ratings yet
- Embryology of The Hind GutDocument10 pagesEmbryology of The Hind Gutproject-247758No ratings yet
- Ricketts1960 ComunicationDocument28 pagesRicketts1960 ComunicationKaichou Wa Maid SamaNo ratings yet
- Splitting Hairs About Splitting Muscles - YmobDocument1 pageSplitting Hairs About Splitting Muscles - Ymobps.paulayanezNo ratings yet
- Histology BrachialDocument15 pagesHistology BrachialSolo UpdateNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Intraoperative Parathyroid Hormone Assays - Uptodate 2022Document18 pagesIntraoperative Parathyroid Hormone Assays - Uptodate 2022juanrangoneNo ratings yet
- Parathyroid Surgery For Inherited Syndromes - Uptodate 2022Document25 pagesParathyroid Surgery For Inherited Syndromes - Uptodate 2022juanrangoneNo ratings yet
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Document27 pagesParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDocument1 pageNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
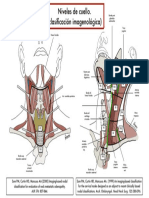
- Clasif Imagenológica Niveles de CuelloDocument1 pageClasif Imagenológica Niveles de CuellojuanrangoneNo ratings yet
- 23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomaDocument19 pages23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomajuanrangoneNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document5 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- SurvivalPhrases Arabic S1L03Document2 pagesSurvivalPhrases Arabic S1L03JohannCoxNo ratings yet
- Chapter04.pdf - How To Write A Project Report - ResearchDocument8 pagesChapter04.pdf - How To Write A Project Report - Researchbrownsugar26No ratings yet
- From Lovemaking To Superconsciousness-0shoDocument31 pagesFrom Lovemaking To Superconsciousness-0shoRAGUPATHYNo ratings yet
- FinAcc MCQ Sem2 PDFDocument11 pagesFinAcc MCQ Sem2 PDFBhavesh Rathod100% (2)
- Dark Souls 3 Lore - Father Ariandel & Sister Friede - VaatividyaDocument5 pagesDark Souls 3 Lore - Father Ariandel & Sister Friede - VaatividyashaunNo ratings yet
- Brakes MCQDocument8 pagesBrakes MCQSathistrnpcNo ratings yet
- VDSL POTS Splitter Whitepaper PDFDocument12 pagesVDSL POTS Splitter Whitepaper PDFEzZamNo ratings yet
- Feeling Good by Michael Bublé Song WorksheetDocument1 pageFeeling Good by Michael Bublé Song WorksheetMirna SolNo ratings yet
- In-Depth Interviews & EthnographyDocument29 pagesIn-Depth Interviews & EthnographyJin ZuanNo ratings yet
- Boat and StreamDocument4 pagesBoat and StreamAllin 1No ratings yet
- Car Sales Cover LetterDocument8 pagesCar Sales Cover Letterf5de9mre100% (2)
- Quarter 2:module 2: Understanding Unchanging Values in Vuca WorldDocument13 pagesQuarter 2:module 2: Understanding Unchanging Values in Vuca WorldDennis CamposNo ratings yet
- Digital Pivot Slide 37Document3 pagesDigital Pivot Slide 37ruciNo ratings yet
- Victor Manuel Chevere v. Jerry Johnson Stephen Kaiser Rick E. Peters Jim Keith Bob Affolter, 38 F.3d 1220, 10th Cir. (1994)Document4 pagesVictor Manuel Chevere v. Jerry Johnson Stephen Kaiser Rick E. Peters Jim Keith Bob Affolter, 38 F.3d 1220, 10th Cir. (1994)Scribd Government DocsNo ratings yet
- Vampires Werewolves and Witches Oh MyDocument51 pagesVampires Werewolves and Witches Oh Myangelg29850% (1)
- Driscoll WordsDocument55 pagesDriscoll WordsMatthew James DriscollNo ratings yet
- Noli Me Tangere CharactersDocument2 pagesNoli Me Tangere Characterseloisa quelitesNo ratings yet
- LTE ENB Feature Description SLR 2 4 V2 0 en PDF 1Document1,021 pagesLTE ENB Feature Description SLR 2 4 V2 0 en PDF 1Swati SiwachNo ratings yet
- ASurveyonthe Associated Factorsof Stressamong Operating Room PersonnelDocument6 pagesASurveyonthe Associated Factorsof Stressamong Operating Room PersonnelzharifderisNo ratings yet
- Emcee ScriptDocument6 pagesEmcee ScriptJasper MomoNo ratings yet
- Colgate-Palmolive Makes A Total EffortDocument2 pagesColgate-Palmolive Makes A Total EffortNandini NagabhushanNo ratings yet
- ToninaDocument6 pagesToninapancholopez2014No ratings yet
- K-Factor Rated Transformer For Deal With Harmonic Generating LoadsDocument4 pagesK-Factor Rated Transformer For Deal With Harmonic Generating Loadsp41005679No ratings yet
- Ob2 Sas 14Document5 pagesOb2 Sas 14Ralph Louie ManagoNo ratings yet
- The Champion Legal Ads: 06-30-22Document46 pagesThe Champion Legal Ads: 06-30-22Donna S. SeayNo ratings yet
- 78-2017ernakulam, KannurDocument13 pages78-2017ernakulam, KannurBingo MeNo ratings yet
- Instruction:: (There Is No SPI According To This SP in KSPK)Document3 pagesInstruction:: (There Is No SPI According To This SP in KSPK)maria oyongNo ratings yet