
CHN Notes Summary
CHN Notes Summary
You might also like
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- CHN NotesDocument7 pagesCHN NotesAnvi Turingan PedronanNo ratings yet
- Gordons TypologyDocument3 pagesGordons TypologyMaxinne Allyssa Cancino RoseñoNo ratings yet
- FNCPDocument14 pagesFNCPhelloaNo ratings yet
- Concept of NUrsingDocument4 pagesConcept of NUrsingcriselda desistoNo ratings yet
- CHN RVW 2Document51 pagesCHN RVW 2Michael UrrutiaNo ratings yet
- 1 Apgar and MMDST 1Document34 pages1 Apgar and MMDST 1Abigail BrillantesNo ratings yet
- Health Teaching and Discharge PlanDocument4 pagesHealth Teaching and Discharge Plankamalab04No ratings yet
- Community Health NursingDocument105 pagesCommunity Health NursingKBDNo ratings yet
- NLE Reviewers: Leadership Management Research and Ethics (LMRE)Document7 pagesNLE Reviewers: Leadership Management Research and Ethics (LMRE)Lot RositNo ratings yet
- COPAR or Community Organizing Participatory Action Research Is A Vital Part ofDocument5 pagesCOPAR or Community Organizing Participatory Action Research Is A Vital Part ofPrei BaltazarNo ratings yet
- Name: Korina A. Rabadon BSN 3-A1 Sas 10Document1 pageName: Korina A. Rabadon BSN 3-A1 Sas 10Sunny Mae Tura PuigNo ratings yet
- Community Health NursingDocument7 pagesCommunity Health NursingRosafe E. PeraltaNo ratings yet
- BioethicsDocument11 pagesBioethicsgabbybibobuNo ratings yet
- Chapter 2 Lesson 3 Learning Input 1 2Document26 pagesChapter 2 Lesson 3 Learning Input 1 2Myla Claire AlipioNo ratings yet
- Involving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialDocument10 pagesInvolving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialAngel MayNo ratings yet
- Kusain - NCP in NCM 112 RleDocument2 pagesKusain - NCP in NCM 112 Rlejay kusainNo ratings yet
- Medicine Ward NCPDocument11 pagesMedicine Ward NCPKimsha ConcepcionNo ratings yet
- Chapter 51. Nursing Care of The Child With A Musculoskeletal Disorder TermsDocument3 pagesChapter 51. Nursing Care of The Child With A Musculoskeletal Disorder TermsJœnríčk AzueloNo ratings yet
- Cultural CompetenceDocument70 pagesCultural Competencekatejewel de rosasNo ratings yet
- Transcultural Perspective in The Nursing Care of Adults Physiologic Development During AdulthoodDocument5 pagesTranscultural Perspective in The Nursing Care of Adults Physiologic Development During AdulthoodeuLa-mayzellNo ratings yet
- Age Related ChangesDocument8 pagesAge Related ChangesEricson CandelariaNo ratings yet
- History of Past IllnessDocument4 pagesHistory of Past IllnessKrisianne Mae Lorenzo FranciscoNo ratings yet
- Clinical PaperDocument18 pagesClinical PaperlhhjklllNo ratings yet
- 2010 TFN Module Unit 06 Nursing Paradigm - NursingDocument43 pages2010 TFN Module Unit 06 Nursing Paradigm - NursingCamille Denise Nucum100% (1)
- Assisting A Patient With Ambulation Using A Walker: Page 1/2Document2 pagesAssisting A Patient With Ambulation Using A Walker: Page 1/2Mac Cristian A. CaraganNo ratings yet
- NCM 114 Gerontology - WeeK 1Document38 pagesNCM 114 Gerontology - WeeK 1Jmarie Brillantes Popioco0% (1)
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- Assessing Pediatric ClientsDocument30 pagesAssessing Pediatric ClientsJae TyNo ratings yet
- Health Assessment and Physical ExaminationDocument5 pagesHealth Assessment and Physical Examinationmrsfelic08No ratings yet
- Nursing Care Plan - MergedDocument13 pagesNursing Care Plan - MergedJuls Flares SycaycoNo ratings yet
- NP1Document14 pagesNP1rexinne noahNo ratings yet
- Gordons TypologyDocument37 pagesGordons TypologyJo PigarNo ratings yet
- Chapter 11Document4 pagesChapter 11Ramsel Kong Tan100% (1)
- Gapuz Fundamentals of NursingDocument61 pagesGapuz Fundamentals of NursingAlphonse ElricNo ratings yet
- Npi Format For Rle 1Document9 pagesNpi Format For Rle 1Patricia VasquezNo ratings yet
- Teaching Plan: Living With Congestive Heart FailureDocument7 pagesTeaching Plan: Living With Congestive Heart FailureAbegail LazoNo ratings yet
- GitDocument302 pagesGitjgcriste100% (7)
- 11 Key Areas of ResponsibilitiesDocument1 page11 Key Areas of Responsibilitiesjo_annamae4413No ratings yet
- Nursing EthicsDocument4 pagesNursing Ethicskai5090No ratings yet
- 2 Community Healtyh Nursing - Field in NursingDocument12 pages2 Community Healtyh Nursing - Field in NursingsannsannNo ratings yet
- Newborn CareDocument3 pagesNewborn CareBudoy WashupapiNo ratings yet
- Unit 1: Concepts, Principles, and Theories in The Care of Older AdultsDocument10 pagesUnit 1: Concepts, Principles, and Theories in The Care of Older AdultsEricson CandelariaNo ratings yet
- Communication With Older AdultsDocument22 pagesCommunication With Older AdultsNathaniel Karl Enin PulidoNo ratings yet
- Community Health NursingDocument140 pagesCommunity Health NursingPrince Jhessie L. Abella67% (3)
- OncoDocument3 pagesOncoTni JolieNo ratings yet
- DINAWANAO3BM2PNDocument2 pagesDINAWANAO3BM2PNCherry Mae DinawanaoNo ratings yet
- Competency Appraisal 1Document30 pagesCompetency Appraisal 1mirai desuNo ratings yet
- Module 2 Phases of The Nursing Research Process Fact Sheet 1Document7 pagesModule 2 Phases of The Nursing Research Process Fact Sheet 1ALAS MichelleNo ratings yet
- VitaminsDocument3 pagesVitaminsJamil Samira E. BuizonNo ratings yet
- The Nursing Process in The Care of The CommunityDocument96 pagesThe Nursing Process in The Care of The CommunityCzarina Aeri RollorataNo ratings yet
- Models of Health and WellnessDocument5 pagesModels of Health and WellnessGlory GloryNo ratings yet
- Oxygen TherapyDocument3 pagesOxygen Therapymarie100% (3)
- NCM 112 E LEARNING AutosavedDocument7 pagesNCM 112 E LEARNING AutosavedMikko McDonie VeloriaNo ratings yet
- Fundamentals of Nursing Practice ReviewerDocument3 pagesFundamentals of Nursing Practice Reviewerchie9268No ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- CHN Notes SummaryDocument6 pagesCHN Notes SummaryLeeyanBhadzzVagayNo ratings yet
- CHN Notes SummaryDocument6 pagesCHN Notes SummaryjeromeNo ratings yet
- Responsibilities of The Nurse in Nutritional CareDocument1 pageResponsibilities of The Nurse in Nutritional CareVIKTORIA SARAH DIZONNo ratings yet
- Role of Nutrients in The Health Illness ContinuumDocument2 pagesRole of Nutrients in The Health Illness ContinuumVIKTORIA SARAH DIZONNo ratings yet
- Nutrients For Nourishment and Pharmacologic FunctionsDocument2 pagesNutrients For Nourishment and Pharmacologic FunctionsVIKTORIA SARAH DIZONNo ratings yet
- NCM 104 - Activity #1Document1 pageNCM 104 - Activity #1VIKTORIA SARAH DIZONNo ratings yet
- Community Health Nursing Reviewer: - 1 Twitter: @nursehoomanDocument12 pagesCommunity Health Nursing Reviewer: - 1 Twitter: @nursehoomanVIKTORIA SARAH DIZONNo ratings yet
- Lp-Grade 10 HealthDocument17 pagesLp-Grade 10 HealthJovelyn TakilidNo ratings yet
- Substance AbuseDocument54 pagesSubstance AbuseCharles CastilloNo ratings yet
- Activity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreDocument4 pagesActivity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreJovie FabrosNo ratings yet
- GDI 12 States FederalismDocument172 pagesGDI 12 States FederalismSupre ScrblNo ratings yet
- Child Rights and You - Wikipedia PDFDocument14 pagesChild Rights and You - Wikipedia PDFpatel mariyamNo ratings yet
- For DissertationDocument13 pagesFor DissertationRegi viniciyaNo ratings yet
- MCQ in OphthalmologyDocument108 pagesMCQ in OphthalmologySushi HtetNo ratings yet
- 5 1 Why Your Body Needs NutrientsDocument3 pages5 1 Why Your Body Needs Nutrientsapi-261782961No ratings yet
- Manual CabinaDocument20 pagesManual CabinaCintexNo ratings yet
- Adolescence and Preg Position PaperDocument2 pagesAdolescence and Preg Position PaperNichole Trisha MontalbaNo ratings yet
- Declaration Form - Work From Home Attachment 2Document1 pageDeclaration Form - Work From Home Attachment 2BAGUIO CATSNo ratings yet
- Kit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9Document2 pagesKit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9micky mouseNo ratings yet
- Section A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Document13 pagesSection A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Sheldon FerronNo ratings yet
- Factor Affecting The Development of FetusDocument8 pagesFactor Affecting The Development of FetusWhye Jun CheongNo ratings yet
- Molly McDowell - Course Project Part 1Document5 pagesMolly McDowell - Course Project Part 1Adelaide DariaNo ratings yet
- Monitoring The Fermentation of GlucoseDocument4 pagesMonitoring The Fermentation of GlucoseSonia IsaacsNo ratings yet
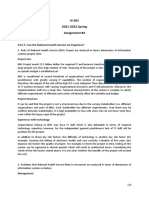
- IS 501 2021-2022 Spring Assignment #4: Part-1: Can The National Health Service Go Paperless?Document3 pagesIS 501 2021-2022 Spring Assignment #4: Part-1: Can The National Health Service Go Paperless?adsfNo ratings yet
- Betz Rebecca ResumeDocument2 pagesBetz Rebecca Resumeapi-316054946No ratings yet
- Knowledge ManagementDocument63 pagesKnowledge Managementrahul-singh-6592No ratings yet
- L. Gifford The Mature Organism ModelDocument12 pagesL. Gifford The Mature Organism ModelRoar SyltebøNo ratings yet
- Orphan Drugs Doctoral SeminarDocument21 pagesOrphan Drugs Doctoral SeminarDr RC Mishra100% (1)
- Abstract Dedication Scope and DelimitationDocument2 pagesAbstract Dedication Scope and DelimitationLufin Buadilla BiolenaNo ratings yet
- Name: Rank: Date: Quiz On IMO Conventions 1. Write True or FalseDocument3 pagesName: Rank: Date: Quiz On IMO Conventions 1. Write True or FalseBisratNo ratings yet
- Prosthodontic Perspective To All On - 4 ConceptDocument33 pagesProsthodontic Perspective To All On - 4 ConceptKrupali JainNo ratings yet
- PacemakersDocument69 pagesPacemakersdocjeevan89100% (1)
- Celebrating Worthing College 2012 SpeadsDocument9 pagesCelebrating Worthing College 2012 SpeadsWorthing College-SportNo ratings yet
- HackerRank - India Benefits and PerksDocument5 pagesHackerRank - India Benefits and PerksNacturNo ratings yet
- Section 8 The CTA Written Examination PDFDocument10 pagesSection 8 The CTA Written Examination PDFBojana VulasNo ratings yet
- Brit J Clinical Pharma - 2001 - Sathyan - Effect of OROS Controlled Release Delivery On The Pharmacokinetics andDocument10 pagesBrit J Clinical Pharma - 2001 - Sathyan - Effect of OROS Controlled Release Delivery On The Pharmacokinetics andGeorgiana CorneagaNo ratings yet
- Clinical AssignmentDocument9 pagesClinical AssignmentkomalNo ratings yet





























































































Download as pdf or txt
You might also like
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- CHN NotesDocument7 pagesCHN NotesAnvi Turingan PedronanNo ratings yet
- Gordons TypologyDocument3 pagesGordons TypologyMaxinne Allyssa Cancino RoseñoNo ratings yet
- FNCPDocument14 pagesFNCPhelloaNo ratings yet
- Concept of NUrsingDocument4 pagesConcept of NUrsingcriselda desistoNo ratings yet
- CHN RVW 2Document51 pagesCHN RVW 2Michael UrrutiaNo ratings yet
- 1 Apgar and MMDST 1Document34 pages1 Apgar and MMDST 1Abigail BrillantesNo ratings yet
- Health Teaching and Discharge PlanDocument4 pagesHealth Teaching and Discharge Plankamalab04No ratings yet
- Community Health NursingDocument105 pagesCommunity Health NursingKBDNo ratings yet
- NLE Reviewers: Leadership Management Research and Ethics (LMRE)Document7 pagesNLE Reviewers: Leadership Management Research and Ethics (LMRE)Lot RositNo ratings yet
- COPAR or Community Organizing Participatory Action Research Is A Vital Part ofDocument5 pagesCOPAR or Community Organizing Participatory Action Research Is A Vital Part ofPrei BaltazarNo ratings yet
- Name: Korina A. Rabadon BSN 3-A1 Sas 10Document1 pageName: Korina A. Rabadon BSN 3-A1 Sas 10Sunny Mae Tura PuigNo ratings yet
- Community Health NursingDocument7 pagesCommunity Health NursingRosafe E. PeraltaNo ratings yet
- BioethicsDocument11 pagesBioethicsgabbybibobuNo ratings yet
- Chapter 2 Lesson 3 Learning Input 1 2Document26 pagesChapter 2 Lesson 3 Learning Input 1 2Myla Claire AlipioNo ratings yet
- Involving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialDocument10 pagesInvolving Family, Domestic Relations, Women and Children. (2015) - Philippine JudicialAngel MayNo ratings yet
- Kusain - NCP in NCM 112 RleDocument2 pagesKusain - NCP in NCM 112 Rlejay kusainNo ratings yet
- Medicine Ward NCPDocument11 pagesMedicine Ward NCPKimsha ConcepcionNo ratings yet
- Chapter 51. Nursing Care of The Child With A Musculoskeletal Disorder TermsDocument3 pagesChapter 51. Nursing Care of The Child With A Musculoskeletal Disorder TermsJœnríčk AzueloNo ratings yet
- Cultural CompetenceDocument70 pagesCultural Competencekatejewel de rosasNo ratings yet
- Transcultural Perspective in The Nursing Care of Adults Physiologic Development During AdulthoodDocument5 pagesTranscultural Perspective in The Nursing Care of Adults Physiologic Development During AdulthoodeuLa-mayzellNo ratings yet
- Age Related ChangesDocument8 pagesAge Related ChangesEricson CandelariaNo ratings yet
- History of Past IllnessDocument4 pagesHistory of Past IllnessKrisianne Mae Lorenzo FranciscoNo ratings yet
- Clinical PaperDocument18 pagesClinical PaperlhhjklllNo ratings yet
- 2010 TFN Module Unit 06 Nursing Paradigm - NursingDocument43 pages2010 TFN Module Unit 06 Nursing Paradigm - NursingCamille Denise Nucum100% (1)
- Assisting A Patient With Ambulation Using A Walker: Page 1/2Document2 pagesAssisting A Patient With Ambulation Using A Walker: Page 1/2Mac Cristian A. CaraganNo ratings yet
- NCM 114 Gerontology - WeeK 1Document38 pagesNCM 114 Gerontology - WeeK 1Jmarie Brillantes Popioco0% (1)
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- Assessing Pediatric ClientsDocument30 pagesAssessing Pediatric ClientsJae TyNo ratings yet
- Health Assessment and Physical ExaminationDocument5 pagesHealth Assessment and Physical Examinationmrsfelic08No ratings yet
- Nursing Care Plan - MergedDocument13 pagesNursing Care Plan - MergedJuls Flares SycaycoNo ratings yet
- NP1Document14 pagesNP1rexinne noahNo ratings yet
- Gordons TypologyDocument37 pagesGordons TypologyJo PigarNo ratings yet
- Chapter 11Document4 pagesChapter 11Ramsel Kong Tan100% (1)
- Gapuz Fundamentals of NursingDocument61 pagesGapuz Fundamentals of NursingAlphonse ElricNo ratings yet
- Npi Format For Rle 1Document9 pagesNpi Format For Rle 1Patricia VasquezNo ratings yet
- Teaching Plan: Living With Congestive Heart FailureDocument7 pagesTeaching Plan: Living With Congestive Heart FailureAbegail LazoNo ratings yet
- GitDocument302 pagesGitjgcriste100% (7)
- 11 Key Areas of ResponsibilitiesDocument1 page11 Key Areas of Responsibilitiesjo_annamae4413No ratings yet
- Nursing EthicsDocument4 pagesNursing Ethicskai5090No ratings yet
- 2 Community Healtyh Nursing - Field in NursingDocument12 pages2 Community Healtyh Nursing - Field in NursingsannsannNo ratings yet
- Newborn CareDocument3 pagesNewborn CareBudoy WashupapiNo ratings yet
- Unit 1: Concepts, Principles, and Theories in The Care of Older AdultsDocument10 pagesUnit 1: Concepts, Principles, and Theories in The Care of Older AdultsEricson CandelariaNo ratings yet
- Communication With Older AdultsDocument22 pagesCommunication With Older AdultsNathaniel Karl Enin PulidoNo ratings yet
- Community Health NursingDocument140 pagesCommunity Health NursingPrince Jhessie L. Abella67% (3)
- OncoDocument3 pagesOncoTni JolieNo ratings yet
- DINAWANAO3BM2PNDocument2 pagesDINAWANAO3BM2PNCherry Mae DinawanaoNo ratings yet
- Competency Appraisal 1Document30 pagesCompetency Appraisal 1mirai desuNo ratings yet
- Module 2 Phases of The Nursing Research Process Fact Sheet 1Document7 pagesModule 2 Phases of The Nursing Research Process Fact Sheet 1ALAS MichelleNo ratings yet
- VitaminsDocument3 pagesVitaminsJamil Samira E. BuizonNo ratings yet
- The Nursing Process in The Care of The CommunityDocument96 pagesThe Nursing Process in The Care of The CommunityCzarina Aeri RollorataNo ratings yet
- Models of Health and WellnessDocument5 pagesModels of Health and WellnessGlory GloryNo ratings yet
- Oxygen TherapyDocument3 pagesOxygen Therapymarie100% (3)
- NCM 112 E LEARNING AutosavedDocument7 pagesNCM 112 E LEARNING AutosavedMikko McDonie VeloriaNo ratings yet
- Fundamentals of Nursing Practice ReviewerDocument3 pagesFundamentals of Nursing Practice Reviewerchie9268No ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- CHN Notes SummaryDocument6 pagesCHN Notes SummaryLeeyanBhadzzVagayNo ratings yet
- CHN Notes SummaryDocument6 pagesCHN Notes SummaryjeromeNo ratings yet
- Responsibilities of The Nurse in Nutritional CareDocument1 pageResponsibilities of The Nurse in Nutritional CareVIKTORIA SARAH DIZONNo ratings yet
- Role of Nutrients in The Health Illness ContinuumDocument2 pagesRole of Nutrients in The Health Illness ContinuumVIKTORIA SARAH DIZONNo ratings yet
- Nutrients For Nourishment and Pharmacologic FunctionsDocument2 pagesNutrients For Nourishment and Pharmacologic FunctionsVIKTORIA SARAH DIZONNo ratings yet
- NCM 104 - Activity #1Document1 pageNCM 104 - Activity #1VIKTORIA SARAH DIZONNo ratings yet
- Community Health Nursing Reviewer: - 1 Twitter: @nursehoomanDocument12 pagesCommunity Health Nursing Reviewer: - 1 Twitter: @nursehoomanVIKTORIA SARAH DIZONNo ratings yet
- Lp-Grade 10 HealthDocument17 pagesLp-Grade 10 HealthJovelyn TakilidNo ratings yet
- Substance AbuseDocument54 pagesSubstance AbuseCharles CastilloNo ratings yet
- Activity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreDocument4 pagesActivity #1: ETHICAL CASE Name: Date: Year/Section: Grade/scoreJovie FabrosNo ratings yet
- GDI 12 States FederalismDocument172 pagesGDI 12 States FederalismSupre ScrblNo ratings yet
- Child Rights and You - Wikipedia PDFDocument14 pagesChild Rights and You - Wikipedia PDFpatel mariyamNo ratings yet
- For DissertationDocument13 pagesFor DissertationRegi viniciyaNo ratings yet
- MCQ in OphthalmologyDocument108 pagesMCQ in OphthalmologySushi HtetNo ratings yet
- 5 1 Why Your Body Needs NutrientsDocument3 pages5 1 Why Your Body Needs Nutrientsapi-261782961No ratings yet
- Manual CabinaDocument20 pagesManual CabinaCintexNo ratings yet
- Adolescence and Preg Position PaperDocument2 pagesAdolescence and Preg Position PaperNichole Trisha MontalbaNo ratings yet
- Declaration Form - Work From Home Attachment 2Document1 pageDeclaration Form - Work From Home Attachment 2BAGUIO CATSNo ratings yet
- Kit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9Document2 pagesKit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9micky mouseNo ratings yet
- Section A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Document13 pagesSection A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Sheldon FerronNo ratings yet
- Factor Affecting The Development of FetusDocument8 pagesFactor Affecting The Development of FetusWhye Jun CheongNo ratings yet
- Molly McDowell - Course Project Part 1Document5 pagesMolly McDowell - Course Project Part 1Adelaide DariaNo ratings yet
- Monitoring The Fermentation of GlucoseDocument4 pagesMonitoring The Fermentation of GlucoseSonia IsaacsNo ratings yet
- IS 501 2021-2022 Spring Assignment #4: Part-1: Can The National Health Service Go Paperless?Document3 pagesIS 501 2021-2022 Spring Assignment #4: Part-1: Can The National Health Service Go Paperless?adsfNo ratings yet
- Betz Rebecca ResumeDocument2 pagesBetz Rebecca Resumeapi-316054946No ratings yet
- Knowledge ManagementDocument63 pagesKnowledge Managementrahul-singh-6592No ratings yet
- L. Gifford The Mature Organism ModelDocument12 pagesL. Gifford The Mature Organism ModelRoar SyltebøNo ratings yet
- Orphan Drugs Doctoral SeminarDocument21 pagesOrphan Drugs Doctoral SeminarDr RC Mishra100% (1)
- Abstract Dedication Scope and DelimitationDocument2 pagesAbstract Dedication Scope and DelimitationLufin Buadilla BiolenaNo ratings yet
- Name: Rank: Date: Quiz On IMO Conventions 1. Write True or FalseDocument3 pagesName: Rank: Date: Quiz On IMO Conventions 1. Write True or FalseBisratNo ratings yet
- Prosthodontic Perspective To All On - 4 ConceptDocument33 pagesProsthodontic Perspective To All On - 4 ConceptKrupali JainNo ratings yet
- PacemakersDocument69 pagesPacemakersdocjeevan89100% (1)
- Celebrating Worthing College 2012 SpeadsDocument9 pagesCelebrating Worthing College 2012 SpeadsWorthing College-SportNo ratings yet
- HackerRank - India Benefits and PerksDocument5 pagesHackerRank - India Benefits and PerksNacturNo ratings yet
- Section 8 The CTA Written Examination PDFDocument10 pagesSection 8 The CTA Written Examination PDFBojana VulasNo ratings yet
- Brit J Clinical Pharma - 2001 - Sathyan - Effect of OROS Controlled Release Delivery On The Pharmacokinetics andDocument10 pagesBrit J Clinical Pharma - 2001 - Sathyan - Effect of OROS Controlled Release Delivery On The Pharmacokinetics andGeorgiana CorneagaNo ratings yet
- Clinical AssignmentDocument9 pagesClinical AssignmentkomalNo ratings yet