Download as pdf or txt
You might also like
- Introductory Medical Surgical Nursing 10 Timby and SmithDocument153 pagesIntroductory Medical Surgical Nursing 10 Timby and SmithStarrx7140% (2)
- Breast MCQDocument55 pagesBreast MCQAhmad Adel Qaqour94% (16)
- Grammar Guidelines in TranscriptionDocument37 pagesGrammar Guidelines in TranscriptionSteph TanaNo ratings yet
- Clinical Case StudyDocument18 pagesClinical Case StudyAubrey StuecklerNo ratings yet
- ManuscriptDocument5 pagesManuscriptAnisa Mulida SafitriNo ratings yet
- Intl J Gynecology Obste - 2018 - Adams - Cancer of The VaginaDocument8 pagesIntl J Gynecology Obste - 2018 - Adams - Cancer of The VaginaBattleAppleNo ratings yet
- Full Paper Giant PT RSHD Kota Bengkulu Maju Pabi Jakarta Revisi NewDocument11 pagesFull Paper Giant PT RSHD Kota Bengkulu Maju Pabi Jakarta Revisi NewPoppy WulandariNo ratings yet
- Ovarian CancerDocument7 pagesOvarian CancerAndi AliNo ratings yet
- FigoDocument11 pagesFigoPraja Putra AdnyanaNo ratings yet
- Cryosurgery of Breast Cancer: Lizhi Niu, Liang Zhou, Kecheng XuDocument8 pagesCryosurgery of Breast Cancer: Lizhi Niu, Liang Zhou, Kecheng XuKaton Adi NugrohoNo ratings yet
- Therapeutic Interventions For Breast Cancer TreatmentDocument12 pagesTherapeutic Interventions For Breast Cancer TreatmentDineshNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case Reportsfitouri asmaNo ratings yet
- Primary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportDocument4 pagesPrimary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportBastiaanNo ratings yet
- Journal On CancerDocument5 pagesJournal On CancerChriz LechNo ratings yet
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDocument6 pagesLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraNo ratings yet
- Breast Sarcoma: About Two Cases and Review of The LiteratureDocument4 pagesBreast Sarcoma: About Two Cases and Review of The LiteratureIJAR JOURNALNo ratings yet
- Breast Cancer Mrker NatureDocument12 pagesBreast Cancer Mrker Naturerajasekaran_mNo ratings yet
- Rare Case of Radiotherapy Induced Angiosarcoma RIAS A - 2024 - International JDocument4 pagesRare Case of Radiotherapy Induced Angiosarcoma RIAS A - 2024 - International JRonald QuezadaNo ratings yet
- Art1 Para+publicarDocument4 pagesArt1 Para+publicardra.camilaalvesbioNo ratings yet
- Adnexal Masses in Pregnancy: An Updated Review: Key Words: Adnexa, Management, Mass, Pregnancy, SurgeryDocument7 pagesAdnexal Masses in Pregnancy: An Updated Review: Key Words: Adnexa, Management, Mass, Pregnancy, SurgeryPamela laquindanumNo ratings yet
- BreastDocument14 pagesBreastapi-3840195No ratings yet
- Breast CancerDocument17 pagesBreast CancerLaura CampañaNo ratings yet
- Research Paper Topics About Breast CancerDocument8 pagesResearch Paper Topics About Breast Cancerafnkjarbwbozrr100% (1)
- Practice Essentials: View Media GalleryDocument8 pagesPractice Essentials: View Media GallerywzlNo ratings yet
- A Case Study On Penile CancerDocument4 pagesA Case Study On Penile CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intl J Gynecology Obste - 2021 - Adams - Cancer of The Vagina 2021 Update 2Document9 pagesIntl J Gynecology Obste - 2021 - Adams - Cancer of The Vagina 2021 Update 2mintunlananobgynNo ratings yet
- Riker ABSITE ReviewDocument36 pagesRiker ABSITE Reviewsgod34No ratings yet
- Running Head: Brachytherapy: Isotopes 1Document20 pagesRunning Head: Brachytherapy: Isotopes 1api-384666214No ratings yet
- Rhabdomyosarcoma of The Vagina in An Adolescent GirDocument11 pagesRhabdomyosarcoma of The Vagina in An Adolescent GirPhn StanleyNo ratings yet
- Sarcoma of The Breast - An Update On A Rare EntityDocument10 pagesSarcoma of The Breast - An Update On A Rare EntityZaniru Raúl Marín MartínezNo ratings yet
- Staging and Treatment of Breast CancerDocument20 pagesStaging and Treatment of Breast CancerSalim Mwiti NabeaNo ratings yet
- 4 5875114609198762278Document13 pages4 5875114609198762278Ashraf JupiterNo ratings yet
- Breast SurgeryDocument14 pagesBreast SurgeryUday Prabhu100% (1)
- Axillary Node Metastases With Occult Primary Breast CancerDocument19 pagesAxillary Node Metastases With Occult Primary Breast CanceraizatamlikhaNo ratings yet
- Phyllodes TumorsDocument4 pagesPhyllodes TumorsNexi anessaNo ratings yet
- Rosendahl 2017Document7 pagesRosendahl 2017Prince VallejosNo ratings yet
- Oral Malignant MelanomaDocument3 pagesOral Malignant MelanomaKrisna AugustianNo ratings yet
- Jmri 26654Document14 pagesJmri 26654marizal saputraNo ratings yet
- Breast SarcomaDocument4 pagesBreast SarcomaMinh Thư DươngNo ratings yet
- Review Adnexal Masses Pregnancy Rcog PDFDocument6 pagesReview Adnexal Masses Pregnancy Rcog PDFRosália Coutada100% (1)
- APBIDocument28 pagesAPBIWindy HardiyantyNo ratings yet
- Ann Oncol 2011 Balmaña Vi31 4Document4 pagesAnn Oncol 2011 Balmaña Vi31 4andiramasNo ratings yet
- Handbook Rhabdomyosarcoma Winter2018Document14 pagesHandbook Rhabdomyosarcoma Winter2018Rizky AmaliahNo ratings yet
- Intl J Gynecology Obste - 2021 - AdamsDocument9 pagesIntl J Gynecology Obste - 2021 - AdamsKalaivathanan VathananNo ratings yet
- Clinical Evaluation of The BreasDocument6 pagesClinical Evaluation of The BreasSalim Mwiti NabeaNo ratings yet
- Dissertation Cervical CancerDocument5 pagesDissertation Cervical CancerWriteMySociologyPaperAnchorage100% (2)
- Current Diagnosis and Management of Ovarian Cysts: Review ArticlesDocument4 pagesCurrent Diagnosis and Management of Ovarian Cysts: Review ArticlesFelNo ratings yet
- Cro0002 0030Document9 pagesCro0002 0030Balaji MallaNo ratings yet
- Chondrosarcoma of Breast - A Case ReportDocument2 pagesChondrosarcoma of Breast - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardDocument6 pagesJournal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardJethro ConcepcionNo ratings yet
- Breast Cancer Staging PDFDocument12 pagesBreast Cancer Staging PDFDanu BagoesNo ratings yet
- Carcinoma of The Breast - Bailey & LoveDocument5 pagesCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Kader2018 Atypical Ductal Hyperplasia - Update On Diagnosis, Management, and Molecular LandscapeDocument11 pagesKader2018 Atypical Ductal Hyperplasia - Update On Diagnosis, Management, and Molecular LandscapeLyka MahrNo ratings yet
- Clinical Services 4Document3 pagesClinical Services 4Jaisurya SharmaNo ratings yet
- Kiran sapru-NEWDocument4 pagesKiran sapru-NEWEvelyn ChacónNo ratings yet
- Ca de Colon y Polipos PDFDocument24 pagesCa de Colon y Polipos PDFGabriela Zavaleta CamachoNo ratings yet
- Ecgy 05 00131Document4 pagesEcgy 05 00131Zaniru Raúl Marín MartínezNo ratings yet
- Maeshima 2021Document7 pagesMaeshima 2021Maryam MohamedaliNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- Breast Disease: Diagnosis and Pathology, Volume 1From EverandBreast Disease: Diagnosis and Pathology, Volume 1Adnan AydinerNo ratings yet
- Breast Cancer in Young WomenFrom EverandBreast Cancer in Young WomenOreste GentiliniNo ratings yet
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceFrom EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceNo ratings yet
- Radiationproctitis 090421073253 Phpapp02Document18 pagesRadiationproctitis 090421073253 Phpapp02Ricky Aris FandikaNo ratings yet
- Specialconsiderationobturatorhernia 110210102125 Phpapp02Document17 pagesSpecialconsiderationobturatorhernia 110210102125 Phpapp02Ricky Aris FandikaNo ratings yet
- Diverticulardiseasecolon 130106062944 Phpapp02Document79 pagesDiverticulardiseasecolon 130106062944 Phpapp02Ricky Aris FandikaNo ratings yet
- 2015 Primary Breast Sarcoma A Retrospective Study Over 35 Years From A Single InstitutionDocument8 pages2015 Primary Breast Sarcoma A Retrospective Study Over 35 Years From A Single InstitutionRicky Aris FandikaNo ratings yet
- Neoadjuvant Chemotherapy For Primary Sarcoma of The Breast: A Case ReportDocument6 pagesNeoadjuvant Chemotherapy For Primary Sarcoma of The Breast: A Case ReportRicky Aris FandikaNo ratings yet
- Primary Breast Sarcoma: Clinicopathologic Series From The Mayo Clinic and Review of The LiteratureDocument5 pagesPrimary Breast Sarcoma: Clinicopathologic Series From The Mayo Clinic and Review of The LiteratureRicky Aris FandikaNo ratings yet
- Primary Breast Sarcoma: A Rare Pathology in Women From The National Cancer Institute (Incan) of MexicoDocument3 pagesPrimary Breast Sarcoma: A Rare Pathology in Women From The National Cancer Institute (Incan) of MexicoRicky Aris FandikaNo ratings yet
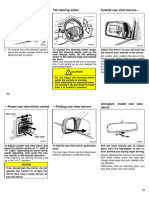
- Tilt Steering Wheel Outside Rear View MirrorsDocument3 pagesTilt Steering Wheel Outside Rear View MirrorsRicky Aris FandikaNo ratings yet
- 2008 Evaluation and Management of Persistent Problems After Surgery For Hirschsprung Disease in A ChildDocument7 pages2008 Evaluation and Management of Persistent Problems After Surgery For Hirschsprung Disease in A ChildRicky Aris FandikaNo ratings yet
- Harris Hip ScoreDocument2 pagesHarris Hip ScoreRicky Aris Fandika50% (2)
- Engineered Nanoparticles For Drug Delivery in CancerTherapyDocument45 pagesEngineered Nanoparticles For Drug Delivery in CancerTherapyLinh Bao NguyenNo ratings yet
- Medicine: Clinical Trial/Experimental StudyDocument10 pagesMedicine: Clinical Trial/Experimental StudyIchaNo ratings yet
- Care of The Clients With Cancer: Prof. Hashim N. Alawi Jr. RN, MANDocument78 pagesCare of The Clients With Cancer: Prof. Hashim N. Alawi Jr. RN, MANjisooNo ratings yet
- Milta 4Document14 pagesMilta 4Victor RoticivNo ratings yet
- Tumor Phyloides JurnalDocument5 pagesTumor Phyloides JurnalSuzika DewiNo ratings yet
- 10.1016@S1470 20451930821 6Document11 pages10.1016@S1470 20451930821 6arifudin_achmadNo ratings yet
- BREAST CANCER & TCM. DR Fatima Manesh PDFDocument140 pagesBREAST CANCER & TCM. DR Fatima Manesh PDFmehranerezvani50% (2)
- Beird Hannah C Osteosarcoma 2022 12Document19 pagesBeird Hannah C Osteosarcoma 2022 12najibNo ratings yet
- Applications of Uv in ClinicalDocument13 pagesApplications of Uv in ClinicalAnonymous Z7myJpGfRNo ratings yet
- NCCN HCC For Patients 2020Document76 pagesNCCN HCC For Patients 2020Dona LagurinNo ratings yet
- Cancer in The Spine PDFDocument369 pagesCancer in The Spine PDFMateo CortesNo ratings yet
- Never Smokers With Lung Cancer in Morocco: Epidemiology and Gender DifferencesDocument6 pagesNever Smokers With Lung Cancer in Morocco: Epidemiology and Gender DifferencesIJPHSNo ratings yet
- Oropharyngeal Cancer: Current Understanding and ManagementDocument7 pagesOropharyngeal Cancer: Current Understanding and ManagementbgdNo ratings yet
- Diagnosis, Treatment, and Nursing ResponsibilitiesDocument109 pagesDiagnosis, Treatment, and Nursing ResponsibilitiespachichoyNo ratings yet
- Neoplastic Disease 1Document69 pagesNeoplastic Disease 1Heba IyadNo ratings yet
- The Role of Molecular Testing in The Differential Diagnosis of Salivary Gland CarcinomasDocument17 pagesThe Role of Molecular Testing in The Differential Diagnosis of Salivary Gland CarcinomasMariela Judith UCNo ratings yet
- Malignant MelanomaDocument29 pagesMalignant MelanomaHealth Education Library for People100% (2)
- Path Questions (USMLE)Document27 pagesPath Questions (USMLE)Goljan UsmleNo ratings yet
- Superficial ParotidectomyDocument7 pagesSuperficial ParotidectomySajid Hussain ShahNo ratings yet
- Testicular Tumor - Dr. FaizDocument54 pagesTesticular Tumor - Dr. FaizFemale calmNo ratings yet
- Guia Europea Evaluación Lesiones Anexiales PreqxDocument40 pagesGuia Europea Evaluación Lesiones Anexiales PreqxfranciscaNo ratings yet
- Matary Surgitoons General 2013Document155 pagesMatary Surgitoons General 2013Raouf Ra'fat Soliman100% (10)
- Breast CancerDocument22 pagesBreast CancerCasey Vergara TañedoNo ratings yet
- Eighth Edition of The UICC Classification of Malignant TumoursDocument14 pagesEighth Edition of The UICC Classification of Malignant TumoursСергей СадовниковNo ratings yet
- The Eighth Edition American Joint Committee On Cancer (AJCC) Melanoma Staging System Implications For Melanoma Treatment and CareDocument23 pagesThe Eighth Edition American Joint Committee On Cancer (AJCC) Melanoma Staging System Implications For Melanoma Treatment and CareValentina IndahNo ratings yet
- CancerDocument5 pagesCancerDins PutrajayaNo ratings yet
- Breast Cancer Facts and Figures 2017 2018 PDFDocument44 pagesBreast Cancer Facts and Figures 2017 2018 PDFamir altaf100% (1)