Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Naloxone and Benzylpenicillin DRUG STUDYDocument3 pagesNaloxone and Benzylpenicillin DRUG STUDYNasrah N. Musa100% (3)
- Nitroglycerin Drug StudyDocument2 pagesNitroglycerin Drug StudyNasrah N. Musa100% (6)
- Cara Urutan Minyak LintahDocument4 pagesCara Urutan Minyak Lintahaerohel100% (1)
- Treatment WorkbookDocument112 pagesTreatment Workbookkmurphy100% (15)
- Helical VS Axial CT ScanningDocument1 pageHelical VS Axial CT ScanningNasrah N. MusaNo ratings yet
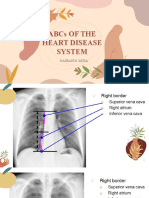
- ABCs of The Heart - Appendix DDocument25 pagesABCs of The Heart - Appendix DNasrah N. MusaNo ratings yet
- Anesthesiology Case PresDocument26 pagesAnesthesiology Case PresNasrah N. MusaNo ratings yet
- NEURO Myasthenia GravisDocument25 pagesNEURO Myasthenia GravisNasrah N. MusaNo ratings yet
- Paracetamol Drug StudyDocument2 pagesParacetamol Drug StudyNasrah N. MusaNo ratings yet
- Potassium Drug StudyDocument2 pagesPotassium Drug StudyNasrah N. Musa100% (2)
- Dopamine HydrochlorideDocument2 pagesDopamine HydrochlorideNasrah N. MusaNo ratings yet
- Atropine Sulfate Drug StudyDocument2 pagesAtropine Sulfate Drug StudyNasrah N. Musa67% (6)
- 3-4 Epinephrine & LidocaineDocument3 pages3-4 Epinephrine & LidocaineNasrah N. MusaNo ratings yet
- Joint Commission InternationalDocument44 pagesJoint Commission InternationalcicaklomenNo ratings yet
- Psychiatric Aspects of Diabetes MellitusDocument8 pagesPsychiatric Aspects of Diabetes MellitusKAUSHAL ARYANo ratings yet
- Benign Moles and LesionsDocument2 pagesBenign Moles and LesionsMari MariNo ratings yet
- AbpsyDocument43 pagesAbpsyLuisNo ratings yet
- FinalDocument329 pagesFinalRauof QaziNo ratings yet
- Pars Plana VitrectomyDocument6 pagesPars Plana VitrectomyAndreas OctavianoNo ratings yet
- Monthly HSE PerformanceReport REV2Document2 pagesMonthly HSE PerformanceReport REV2parthaNo ratings yet
- Chapter 5Document5 pagesChapter 5Friends ForeverNo ratings yet
- CH 21 Abdomen JARVISDocument34 pagesCH 21 Abdomen JARVISAndy NguyenNo ratings yet
- Full Chapter Percutaneous Collagen Induction With Microneedling A Step by Step Clinical Guide Emerson Lima PDFDocument53 pagesFull Chapter Percutaneous Collagen Induction With Microneedling A Step by Step Clinical Guide Emerson Lima PDFgloria.graves449100% (7)
- Nursing Care Plan Juvida, Clarissa A. BSN 2A: "Mainit Ang Anak Ko at Nanghihina ."Document3 pagesNursing Care Plan Juvida, Clarissa A. BSN 2A: "Mainit Ang Anak Ko at Nanghihina ."Clarissa JuvidaNo ratings yet
- Atropine Sulphate 1mg/1ml Emergency MedicationDocument2 pagesAtropine Sulphate 1mg/1ml Emergency MedicationRafiq EsufzaeNo ratings yet
- Wilkins Clinical Assessment in Respiratory Care 7th Edition Heuer Test BankDocument10 pagesWilkins Clinical Assessment in Respiratory Care 7th Edition Heuer Test Bankanthelioncingulumgvxq100% (26)
- Outpatient Art Therapy With A Suicidal AdolDocument16 pagesOutpatient Art Therapy With A Suicidal AdolEsteban Ferrandez MirallesNo ratings yet
- Borges, K. Et Al. (2018)Document7 pagesBorges, K. Et Al. (2018)Paulina Bermudez ValenzuelaNo ratings yet
- Vertigo and DizzinessDocument161 pagesVertigo and DizzinessSyariah KhilafahNo ratings yet
- Catholic University of America Student Health Plan For 2021-22 School YearDocument37 pagesCatholic University of America Student Health Plan For 2021-22 School YearThe College FixNo ratings yet
- AHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementDocument38 pagesAHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementPratik TripathiNo ratings yet
- Memory Loss & 10 Early Signs of Alzheimer's - Alzheimer's AssociationDocument9 pagesMemory Loss & 10 Early Signs of Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamNo ratings yet
- Injury and Overuse Injury.: Classification of Sports InjuriesDocument2 pagesInjury and Overuse Injury.: Classification of Sports InjuriesVladGrosuNo ratings yet
- Rle Lectures Medications: Arturo G. Garcia JR RN, MSN, U.S RNDocument33 pagesRle Lectures Medications: Arturo G. Garcia JR RN, MSN, U.S RNMaria Paula Amor GeronimoNo ratings yet
- NCP Knowledge Deficit PDFDocument2 pagesNCP Knowledge Deficit PDFskylertNo ratings yet
- Test Bank For Principles and Practice of Radiation Therapy 4th Edition Charles M Washington Dennis T LeaverDocument24 pagesTest Bank For Principles and Practice of Radiation Therapy 4th Edition Charles M Washington Dennis T LeaverLisaFloresxtyc100% (43)
- HHS Public AccessDocument16 pagesHHS Public AccessintanNo ratings yet
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaNo ratings yet
- 2019 StromDocument8 pages2019 Stromfabian.balazs.93No ratings yet
- تقرير طبيDocument3 pagesتقرير طبيSmart Certified Translation ServicesNo ratings yet
- (Download PDF) Essentials of Radiology Common Indications and Interpretation 4Th Edition Mettler JR MD MPH Online Ebook All Chapter PDFDocument42 pages(Download PDF) Essentials of Radiology Common Indications and Interpretation 4Th Edition Mettler JR MD MPH Online Ebook All Chapter PDFtracy.freeman317100% (14)