Download as pdf or txt
You might also like
- Westmead Obstetric Anaesthesia Manual 2020Document72 pagesWestmead Obstetric Anaesthesia Manual 2020DavidNo ratings yet
- PCP Western Visayad Panay Chapter Rite/Psbim ReviewDocument6 pagesPCP Western Visayad Panay Chapter Rite/Psbim ReviewKarl Pineda0% (1)
- Naloxone and Benzylpenicillin DRUG STUDYDocument3 pagesNaloxone and Benzylpenicillin DRUG STUDYNasrah N. Musa100% (3)
- Nitroglycerin Drug StudyDocument2 pagesNitroglycerin Drug StudyNasrah N. Musa100% (6)
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- Awareness Under AnesthesiaDocument27 pagesAwareness Under AnesthesiaagatakassaNo ratings yet
- Anesthesia For Patients With Thyroid Disease - UpToDateDocument12 pagesAnesthesia For Patients With Thyroid Disease - UpToDateJavier GlezqNo ratings yet
- FINAL CA-1 Tutorial Textbook 2017Document74 pagesFINAL CA-1 Tutorial Textbook 2017Farjad IkramNo ratings yet
- Thyroid Disease Anesthetic ConsiderationsDocument30 pagesThyroid Disease Anesthetic Considerationssachin10dulkarNo ratings yet
- Failed Spinal AnaesthesiaDocument10 pagesFailed Spinal Anaesthesian12345678n100% (1)
- Anesthesia PresentationDocument19 pagesAnesthesia PresentationJohnyNo ratings yet
- TIVA - Copy (2) - Copy-1Document34 pagesTIVA - Copy (2) - Copy-1Keerthikumar Parvatha100% (2)
- Obesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghDocument56 pagesObesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghRafi ramdhanNo ratings yet
- 7..intravenous Anaesthesia 2Document23 pages7..intravenous Anaesthesia 2Mwiliza BrendaNo ratings yet
- FCA 2 Trials MindmapDocument1 pageFCA 2 Trials MindmapameenallyNo ratings yet
- Total Intravenous Anaesthesia in Children-1 PDFDocument6 pagesTotal Intravenous Anaesthesia in Children-1 PDFAurora TrifaNo ratings yet
- A Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionDocument6 pagesA Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionInternational Organization of Scientific Research (IOSR)No ratings yet
- Post Op DeliriumDocument26 pagesPost Op DeliriumKannan GNo ratings yet
- @anesthesia Books 2018 Neuroanesthesia Crisis Manual DepartmentDocument56 pages@anesthesia Books 2018 Neuroanesthesia Crisis Manual DepartmentLizzeth Inés Sánchez MendozaNo ratings yet
- Journal ClubDocument26 pagesJournal Clubysindhura23gmailcom100% (1)
- Perioperative Fluid Management OptimizedDocument52 pagesPerioperative Fluid Management OptimizedIndah Fitri Okta100% (3)
- Severe Dengue in ICUDocument35 pagesSevere Dengue in ICUanaeshklNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- Anaesthesia For Neuroradiological Procedures Premalatha SDocument48 pagesAnaesthesia For Neuroradiological Procedures Premalatha SPrema LathaNo ratings yet
- Enhanced Recovery After Surgery (ERAS) in Emergency Abdominal Surgery: Background, Preoperative Components of ERAS, Intraoperative Components of ERASDocument9 pagesEnhanced Recovery After Surgery (ERAS) in Emergency Abdominal Surgery: Background, Preoperative Components of ERAS, Intraoperative Components of ERASAndre F SusantioNo ratings yet
- Anesthesia For GeriatricDocument21 pagesAnesthesia For GeriatricintanNo ratings yet
- 029 Reddy PDFDocument59 pages029 Reddy PDFKonas Xi PalembangNo ratings yet
- List of Must Read Books and Journals For DNB AnaesthesiaDocument2 pagesList of Must Read Books and Journals For DNB AnaesthesiaSirisha CkvNo ratings yet
- Asa 2013Document1,076 pagesAsa 2013Marwa Mahrous100% (4)
- Anesthesia For Kidney TransplantDocument6 pagesAnesthesia For Kidney TransplantachyutsharmaNo ratings yet
- AnaesthesiaDocument8 pagesAnaesthesiarakeeb qadriNo ratings yet
- Anesthesia For Tracheoesophageal Fistula RepairDocument29 pagesAnesthesia For Tracheoesophageal Fistula RepairArop AkechNo ratings yet
- Anaesthesia and Sedation Outside TheatresDocument15 pagesAnaesthesia and Sedation Outside Theatresمحمد زينNo ratings yet
- Cyprian Mendonca The Structured Oral Examination in AnesthesiaDocument578 pagesCyprian Mendonca The Structured Oral Examination in AnesthesiaNawaz ShaikNo ratings yet
- OSA and Periop Complications 2012Document9 pagesOSA and Periop Complications 2012cjbae22No ratings yet
- Anesthesia TechnicianDocument1 pageAnesthesia TechnicianmahbbobNo ratings yet
- Perioperative Management of Fluids and Electrolytes in ChildrenDocument6 pagesPerioperative Management of Fluids and Electrolytes in ChildrenBetyCamarilloNo ratings yet
- Epidural AnaesthesiaDocument99 pagesEpidural AnaesthesiaabhinavguttikondaNo ratings yet
- How To Prepare For The EDAIC 2019Document17 pagesHow To Prepare For The EDAIC 2019sand52525No ratings yet
- Awareness in Anesthesia FinalisedDocument42 pagesAwareness in Anesthesia FinalisedLean CyNo ratings yet
- Epidural Anatomy & PhysiologyDocument14 pagesEpidural Anatomy & PhysiologyAbel AxelNo ratings yet
- Anesthetic Machine For StudentDocument76 pagesAnesthetic Machine For StudentMohmmed MousaNo ratings yet
- Pediatric Regional Anesthesia 2005Document66 pagesPediatric Regional Anesthesia 2005tameem89No ratings yet
- Extubation After AnaesthesiaDocument7 pagesExtubation After AnaesthesiaaksinuNo ratings yet
- Anaesthesia For Trauma PatientsDocument42 pagesAnaesthesia For Trauma PatientsMerindukan Surga MuNo ratings yet
- Premedication: by Alif Moderator: Dr. JasmineDocument45 pagesPremedication: by Alif Moderator: Dr. JasmineAlef AminNo ratings yet
- Airway ManagmentDocument42 pagesAirway Managmentkader abdiNo ratings yet
- Recommended Reading List For EDAICDocument5 pagesRecommended Reading List For EDAICManuela CormioNo ratings yet
- Anesthesia TechnologyDocument56 pagesAnesthesia TechnologyDeepali SinghNo ratings yet
- Update in AnaesthesiaDocument49 pagesUpdate in AnaesthesiawahyuwirawanNo ratings yet
- Anaesthesia For Cardiac DiseaseDocument26 pagesAnaesthesia For Cardiac DiseasePrabhu KumarNo ratings yet
- Context Sensitive Half Time (CSHT) - The Lay Medical ManDocument3 pagesContext Sensitive Half Time (CSHT) - The Lay Medical Manpradeep danielNo ratings yet
- Regional AnesthesiaDocument54 pagesRegional AnesthesiaIdza Fariha AfriNo ratings yet
- Anesthesia For TurpDocument5 pagesAnesthesia For Turpdrkadiyala2No ratings yet
- Update EmergenciesDocument84 pagesUpdate EmergenciesElaineNo ratings yet
- Effect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyDocument10 pagesEffect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyIOSRjournalNo ratings yet
- Anesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaDocument3 pagesAnesthesia - State of Narcosis, Analgesia, Relaxation, and Loss of Reflex. Effects of AnesthesiaJhevilin RMNo ratings yet
- Diploma Guide - EnglishDocument11 pagesDiploma Guide - EnglishAndra Victoria TitaNo ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- Pediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderFrom EverandPediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderNo ratings yet
- Evidence-Based Obstetric AnesthesiaFrom EverandEvidence-Based Obstetric AnesthesiaStephen H. HalpernNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- Helical VS Axial CT ScanningDocument1 pageHelical VS Axial CT ScanningNasrah N. MusaNo ratings yet
- NEURO Myasthenia GravisDocument25 pagesNEURO Myasthenia GravisNasrah N. MusaNo ratings yet
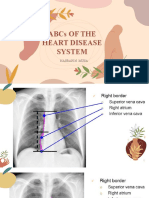
- ABCs of The Heart - Appendix DDocument25 pagesABCs of The Heart - Appendix DNasrah N. MusaNo ratings yet
- Potassium Drug StudyDocument2 pagesPotassium Drug StudyNasrah N. Musa100% (2)
- Paracetamol Drug StudyDocument2 pagesParacetamol Drug StudyNasrah N. MusaNo ratings yet
- Dopamine HydrochlorideDocument2 pagesDopamine HydrochlorideNasrah N. MusaNo ratings yet
- Atropine Sulfate Drug StudyDocument2 pagesAtropine Sulfate Drug StudyNasrah N. Musa67% (6)
- 3-4 Epinephrine & LidocaineDocument3 pages3-4 Epinephrine & LidocaineNasrah N. MusaNo ratings yet
- S.5 BIO Reproduction in Animals NOTESDocument18 pagesS.5 BIO Reproduction in Animals NOTESmusokelukia6No ratings yet
- Miasm BerkshireDocument20 pagesMiasm Berkshirehyder2oo9No ratings yet
- Turner SyndromeDocument12 pagesTurner Syndromenouval_iqbalNo ratings yet
- Determination of Blood GlucoseDocument3 pagesDetermination of Blood GlucoseAki OtaniNo ratings yet
- Thyrotoxicosis: Giridhar MF 9 TermDocument19 pagesThyrotoxicosis: Giridhar MF 9 TermGiridhar MFNo ratings yet
- Endocrine Male-FemaleDocument4 pagesEndocrine Male-FemaleMoatasem AhmedNo ratings yet
- W02 - Diabetic Emergencies in CCDocument36 pagesW02 - Diabetic Emergencies in CCHelene AlawamiNo ratings yet
- RSSDI 2021 Scientific Program N 211110 092720Document28 pagesRSSDI 2021 Scientific Program N 211110 092720Meera FarmsNo ratings yet
- Thyroid CancerDocument22 pagesThyroid CancerHidayah JaiNo ratings yet
- UTS Physical Sexual Self ActivityDocument3 pagesUTS Physical Sexual Self ActivityHanna CasasNo ratings yet
- ST 2 Gr. 5 Science With TosDocument4 pagesST 2 Gr. 5 Science With TosEG Bitong-AlamaniNo ratings yet
- Physical ChangesDocument2 pagesPhysical ChangesSarra GrandeNo ratings yet
- Senior Six Biology Paper 1 Exam 12 For Consultation Call 0776802709Document13 pagesSenior Six Biology Paper 1 Exam 12 For Consultation Call 0776802709Nsubuga ArthurNo ratings yet
- Diabetes Insipidus - NIDDKDocument9 pagesDiabetes Insipidus - NIDDKAnam MirNo ratings yet
- Glandular EpitheliumDocument34 pagesGlandular EpitheliumAnonymous WBMLOgPNo ratings yet
- Chemistry InvestigatoryDocument19 pagesChemistry Investigatoryakhilnz06No ratings yet
- Hyper Parathyroid IsmDocument7 pagesHyper Parathyroid IsmEllene Mae Dejapa VillasisNo ratings yet
- Asesmen Keterampilan Berpikir Tingkat Tinggi PDFDocument23 pagesAsesmen Keterampilan Berpikir Tingkat Tinggi PDFFitria HandayaniNo ratings yet
- Lesson 6 Thyroid and Antithyroid DrugsDocument28 pagesLesson 6 Thyroid and Antithyroid DrugstheintrovNo ratings yet
- Female Reproductive AnatomyDocument28 pagesFemale Reproductive AnatomySuho Leexokleader KimNo ratings yet
- GynecologyDocument124 pagesGynecologyrajkumar871992No ratings yet
- Repoductive SystemDocument14 pagesRepoductive SystemJhoanna Marie RebutNo ratings yet
- History of Pump TechnologyDocument9 pagesHistory of Pump TechnologyMridula Ayush BhargavaNo ratings yet
- HipothiroidDocument27 pagesHipothiroidYuji AdityaNo ratings yet
- The Weekly Time Table For Year I Semester II of 2016 - 2017 FinalDocument26 pagesThe Weekly Time Table For Year I Semester II of 2016 - 2017 FinalsoeNo ratings yet
- Terapijski Pristup Lecenju EndometriozeDocument16 pagesTerapijski Pristup Lecenju EndometriozeMiraNo ratings yet
- Down Syndrome and Thyroid Disorders: A Review: 25 V. P. PrasherDocument18 pagesDown Syndrome and Thyroid Disorders: A Review: 25 V. P. PrasherErNi CiewekwekcrewetNo ratings yet
- Case Report Amenore SekunderDocument16 pagesCase Report Amenore SekunderNinta Karina Astila SembiringNo ratings yet
- Anatomi Dan Fisiologi KuliitDocument40 pagesAnatomi Dan Fisiologi KuliitZulfani AdhiyatmiNo ratings yet