Download as pdf or txt
You might also like
- UndergroundG StyleHandgunMainManual PDFDocument46 pagesUndergroundG StyleHandgunMainManual PDFRick Gaines100% (2)
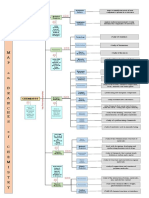
- Concept MapDocument1 pageConcept MapLesley Joy T. BaldonadoNo ratings yet
- Chronic Kidney Disease StagesDocument62 pagesChronic Kidney Disease StagesBryant Munoz100% (3)
- Understanding Chronic Kidney Disease: A guide for the non-specialistFrom EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistRating: 4 out of 5 stars4/5 (3)
- Chronic Kidney DiseaseDocument48 pagesChronic Kidney DiseaseDaniel Apuan SalviejoNo ratings yet
- Patofisiologi Penyakit Ginjal KronikDocument35 pagesPatofisiologi Penyakit Ginjal KronikEgy Sunanda Putra Direktorat Poltekkes JambiNo ratings yet
- CKD 2016Document39 pagesCKD 2016husnaNo ratings yet
- CKD - Case StudyDocument48 pagesCKD - Case StudyEdmond DontessNo ratings yet
- CKD, Mbbs LectureDocument25 pagesCKD, Mbbs LectureElvis obajeNo ratings yet
- 12B. Kuliah CKD 2017Document44 pages12B. Kuliah CKD 2017yussikafernandaNo ratings yet
- Chronic Kidney Disease (CKD)Document22 pagesChronic Kidney Disease (CKD)Jevon AndraNo ratings yet
- Gagal Ginjal Akut & Gagal Ginjal KronikDocument63 pagesGagal Ginjal Akut & Gagal Ginjal KronikSuf YusufNo ratings yet
- Chronic Kidney Disease (CKD) in Children: DR Saiel Al Sarhan MD, PHDDocument48 pagesChronic Kidney Disease (CKD) in Children: DR Saiel Al Sarhan MD, PHDMAYSAA HamarnehNo ratings yet
- Chronic Kidney Disease: Wondifraw A. (MD)Document38 pagesChronic Kidney Disease: Wondifraw A. (MD)SebliNo ratings yet
- Hasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityDocument51 pagesHasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityMuhammad Yasdar BahriNo ratings yet
- Chronic Kidney DiseaseDocument39 pagesChronic Kidney DiseaseAgatha RogerNo ratings yet
- Chronic Kidney Disease: The BasicsDocument56 pagesChronic Kidney Disease: The BasicsAlmas Safina KauserNo ratings yet
- Chronic Kidney DiseaseDocument39 pagesChronic Kidney DiseaseGumarbio Setiadi Zakaria100% (1)
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseIda Bagus Putu Swabawa100% (1)
- Chronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaDocument62 pagesChronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaSamuel LalNo ratings yet
- Chronic Kidney DiseaseDocument34 pagesChronic Kidney DiseaseVina ZulfianiNo ratings yet
- Chronic Kidney Disease: Disampaikan Oleh: Wilda Maula Miftah Nur Aknowledgement: Dr. Mia Melinda, SP - PDDocument32 pagesChronic Kidney Disease: Disampaikan Oleh: Wilda Maula Miftah Nur Aknowledgement: Dr. Mia Melinda, SP - PDErryz JogjuzzNo ratings yet
- Chronic Kidney DiseaseDocument49 pagesChronic Kidney Diseasesarguss1471% (7)
- DR. Butar Butar - Diabetic Kidney Disease How To Regress (PIT MAKASAR, 23-26 Nov 06)Document42 pagesDR. Butar Butar - Diabetic Kidney Disease How To Regress (PIT MAKASAR, 23-26 Nov 06)Didi RaufNo ratings yet
- CKD AnDocument44 pagesCKD AndimbrutNo ratings yet
- Chronic Kidney DiseaseDocument24 pagesChronic Kidney DiseasepradeepnagdaNo ratings yet
- Modul 1Document270 pagesModul 1Ailsa ZahraniNo ratings yet
- Gagal Ginjal Kronik FarmakoDocument28 pagesGagal Ginjal Kronik FarmakoIkhza Yasyifa RusydaNo ratings yet
- CKD CHCRTDocument28 pagesCKD CHCRTNurhidayati KeriyunNo ratings yet
- Chronic Kidney Disease: by Hasyim KasimDocument31 pagesChronic Kidney Disease: by Hasyim KasimFauziah AbidahNo ratings yet
- Diagnosa Penyakit Ginjal Kronik Dan Indikasi TPG RRTDocument56 pagesDiagnosa Penyakit Ginjal Kronik Dan Indikasi TPG RRTASIS ADRINo ratings yet
- CKD PDFDocument15 pagesCKD PDFJendrale SudirmanNo ratings yet
- CKD Du 22Document76 pagesCKD Du 22PUTROSM DARSONONo ratings yet
- Chronic Kidney Disease: Progression Modifying TherapiesDocument29 pagesChronic Kidney Disease: Progression Modifying Therapiesdfsdsfsd100% (1)
- Chronic Kidney Disease: Bobby Laksana D Putri Priela Pembimbing: Dr. Nursamsu, SPPDDocument30 pagesChronic Kidney Disease: Bobby Laksana D Putri Priela Pembimbing: Dr. Nursamsu, SPPDfrostedsurgeonNo ratings yet
- Chronic Kidney Disease: DR - SarmisthaDocument19 pagesChronic Kidney Disease: DR - SarmisthaGebby MamuayaNo ratings yet
- Clinicopathological Conference 2Document23 pagesClinicopathological Conference 2Rem AlfelorNo ratings yet
- Chronic Kidney Disease LIFA FixxxDocument19 pagesChronic Kidney Disease LIFA FixxxMuzdalifa MohamadNo ratings yet
- Management of Hypertension in CKDDocument40 pagesManagement of Hypertension in CKDPratik TripathiNo ratings yet
- GGK PKMRS PugerDocument12 pagesGGK PKMRS Pugersyamsul arifinNo ratings yet
- Chronic Kidney DiseaseDocument3 pagesChronic Kidney Diseaseapi-668470097No ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Chronic Disease: KidneyDocument31 pagesChronic Disease: KidneyHazel Marie EchavezNo ratings yet
- Chronic Kidney Disease - EMEDICINE 3020.docx.2021Document56 pagesChronic Kidney Disease - EMEDICINE 3020.docx.2021qayyum consultantfpscNo ratings yet
- Toronto Notes Nephrology 2015 20Document1 pageToronto Notes Nephrology 2015 20JUSASBNo ratings yet
- Chronic Kidney Disease (Kuliah Mhs SMT IV FK Unud 08)Document23 pagesChronic Kidney Disease (Kuliah Mhs SMT IV FK Unud 08)Arvindan Subramaniam100% (1)
- Chronic Kidney Disease: Rizki Aliana AgustinaDocument85 pagesChronic Kidney Disease: Rizki Aliana AgustinaRofi IrmanNo ratings yet
- Chronic Kidney DiseaseDocument18 pagesChronic Kidney DiseaseAde Cahyo IslamiNo ratings yet
- Chronic Kidney DiseaseDocument18 pagesChronic Kidney DiseaseAde Cahyo IslamiNo ratings yet
- Chronic Kidney Disease - UnhaluDocument57 pagesChronic Kidney Disease - UnhaluRahmawati HamudiNo ratings yet
- PPT CKDDocument35 pagesPPT CKDCandice LavigneNo ratings yet
- Chronic Kidney DiseaseDocument11 pagesChronic Kidney DiseaseSalma Mohamed RezkNo ratings yet
- Gagal Ginjal Kuliah FarmakoterapiDocument39 pagesGagal Ginjal Kuliah FarmakoterapiriyuNo ratings yet
- CKD MedscapeDocument65 pagesCKD MedscapeLuses Shantia HaryantoNo ratings yet
- Chronic Kidney DiseaseDocument35 pagesChronic Kidney DiseaseCindyNo ratings yet
- Supplementary Information To Chapter 27: Kidney Function Tests Markers For Renal Assessment (Old and New)Document10 pagesSupplementary Information To Chapter 27: Kidney Function Tests Markers For Renal Assessment (Old and New)Aaron JoseNo ratings yet
- Supplementary Information To Chapter 27: Kidney Function Tests Markers For Renal Assessment (Old and New)Document10 pagesSupplementary Information To Chapter 27: Kidney Function Tests Markers For Renal Assessment (Old and New)Aaron JoseNo ratings yet
- Chronic Kidney Disease: Diagnosis and TherapyDocument21 pagesChronic Kidney Disease: Diagnosis and TherapyLindsNo ratings yet
- CKD Kdigo 2012Document27 pagesCKD Kdigo 2012giggs_libraNo ratings yet
- Curs 5 Nefro Boala Cronica de RinichiDocument113 pagesCurs 5 Nefro Boala Cronica de RinichiAdriana Vladutu100% (2)
- ChalazionDocument5 pagesChalazionSzakál Timea-BlankaNo ratings yet
- ModulationDocument7 pagesModulationSyeda MiznaNo ratings yet
- Sailing With Paul - IronsideDocument3 pagesSailing With Paul - IronsideLawrence GarnerNo ratings yet
- InglesDocument5 pagesInglesJessi mondragonNo ratings yet
- Rmit PHD Thesis GuidelinesDocument7 pagesRmit PHD Thesis Guidelinesdwnt5e3k100% (2)
- Physical Education - 12th PDFDocument340 pagesPhysical Education - 12th PDFGunal Agarwal100% (1)
- Piano Solo XXDocument6 pagesPiano Solo XXschweyermatthieuNo ratings yet
- Butterflies and MothsDocument59 pagesButterflies and MothsReegen Tee100% (3)
- Adebabay AbayDocument23 pagesAdebabay Abaymaheder wegayehuNo ratings yet
- Lab 6 Shouq PDFDocument10 pagesLab 6 Shouq PDFreemy100% (1)
- Pgcet Environmental Engineering PaperDocument10 pagesPgcet Environmental Engineering PaperRamNo ratings yet
- Conceptual Design of An Automotive Composite Brake Pedal: Mohd Sapuan Salit, Mohd Syed Ali Molla and MD Liakot AliDocument5 pagesConceptual Design of An Automotive Composite Brake Pedal: Mohd Sapuan Salit, Mohd Syed Ali Molla and MD Liakot Aliseran ünalNo ratings yet
- Popular Dance: Isaac. Alexandra Nicole Q BSA-1CDocument5 pagesPopular Dance: Isaac. Alexandra Nicole Q BSA-1CAlexandra Nicole IsaacNo ratings yet
- Characteristics of LDCsDocument22 pagesCharacteristics of LDCstinsaeres100% (2)
- LED Large Digital Stopwatch Timer - Electronics USADocument5 pagesLED Large Digital Stopwatch Timer - Electronics USAmrdadeNo ratings yet
- BSI BCI Horizon Scan Report 2016 PDFDocument32 pagesBSI BCI Horizon Scan Report 2016 PDFSandraNo ratings yet
- Accounting Standards - Handwritten Notes - Udesh Regular - Group 1Document24 pagesAccounting Standards - Handwritten Notes - Udesh Regular - Group 1Uday TomarNo ratings yet
- Effect of Bolt Pretension in Single Lap Bolted Joint IJERTV4IS010269Document4 pagesEffect of Bolt Pretension in Single Lap Bolted Joint IJERTV4IS010269ayush100% (1)
- Communication MatrixDocument1 pageCommunication Matrixrohini kadamNo ratings yet
- If I Ain't Got You - Alicia KeysDocument4 pagesIf I Ain't Got You - Alicia Keysyoropih188No ratings yet
- Nuclear PhysicsDocument85 pagesNuclear PhysicsKy2ST3z4No ratings yet
- APP Modified Bituminous Waterproofing and Damp-Proofing Membrane With Polyester Reinforcement - SpecificationDocument15 pagesAPP Modified Bituminous Waterproofing and Damp-Proofing Membrane With Polyester Reinforcement - Specificationjitendra0% (1)
- Application DevelopmentDocument14 pagesApplication DevelopmentReema MubarakNo ratings yet
- Sliding Doors Standard Sizes NSWDocument3 pagesSliding Doors Standard Sizes NSWCorey WardNo ratings yet
- Satellite CommunicationsDocument57 pagesSatellite Communicationsheritage336No ratings yet
- Naet Basic 15 GuideDocument6 pagesNaet Basic 15 Guidesissicarranza100% (1)
- Cooling Tower AshraeDocument18 pagesCooling Tower AshraeMAITREE JHANo ratings yet
- Ncert Solutions Class 6 Civics Chapter 3 PDFDocument2 pagesNcert Solutions Class 6 Civics Chapter 3 PDFSabaNo ratings yet