Download as pdf or txt
You might also like
- FDR Smart X Operation ManualDocument115 pagesFDR Smart X Operation ManualchronisNo ratings yet
- Comprehensive Nursing Assessment ToolDocument7 pagesComprehensive Nursing Assessment ToolRamesh KandagatlaNo ratings yet
- Falla InmunologicaDocument10 pagesFalla InmunologicaAlejandra OrtizNo ratings yet
- Artigo Sobre AidsDocument7 pagesArtigo Sobre AidscamilatututNo ratings yet
- s12879 021 06459 ZDocument11 pagess12879 021 06459 ZCliff Daniel DIANZOLE MOUNKANANo ratings yet
- Cohorte 10 PDFDocument7 pagesCohorte 10 PDFLaura MottaNo ratings yet
- s12889 019 7980 XDocument12 pagess12889 019 7980 XYayew MaruNo ratings yet
- Healthcare Associated Infection and Its Risk Factors Among Patients Admitted To A Tertiary Hospital in Ethiopia: Longitudinal StudyDocument9 pagesHealthcare Associated Infection and Its Risk Factors Among Patients Admitted To A Tertiary Hospital in Ethiopia: Longitudinal StudycarlosNo ratings yet
- Determinants of HIV Infection Among Children Born To HIV Positive Mothers On Prevention of Mother To Child Transmission Program at Referral Hospitals in West Amhara 2022Document9 pagesDeterminants of HIV Infection Among Children Born To HIV Positive Mothers On Prevention of Mother To Child Transmission Program at Referral Hospitals in West Amhara 2022masiNo ratings yet
- Adhearence GechoDocument9 pagesAdhearence Gechosinte beyuNo ratings yet
- AIDS Research and TherapyDocument10 pagesAIDS Research and TherapyDjamal ToeNo ratings yet
- Research On Prevalence of TB FinalDocument9 pagesResearch On Prevalence of TB FinalBontuNo ratings yet
- 2020 Article 722Document7 pages2020 Article 722Grâce KabengeleNo ratings yet
- 2018 Article 314Document11 pages2018 Article 314marisaNo ratings yet
- Researcharticle Open Access: Tigist EngdaDocument12 pagesResearcharticle Open Access: Tigist EngdasitiNo ratings yet
- Predictors of Tuberculosis (TBDocument11 pagesPredictors of Tuberculosis (TBchikomuezza19No ratings yet
- Piaa 030Document10 pagesPiaa 030Suryadi LimardiNo ratings yet
- 2018 - Baraki Et AlDocument8 pages2018 - Baraki Et AlazeemathmariyamNo ratings yet
- Ambo UniversityDocument12 pagesAmbo UniversityArarsa TolasaNo ratings yet
- Comparison of Antiretroviral Therapy Adherence Among HIV Infected Older Adults With Younger Adults in Africa: Systematic Review and Meta AnalysisDocument14 pagesComparison of Antiretroviral Therapy Adherence Among HIV Infected Older Adults With Younger Adults in Africa: Systematic Review and Meta AnalysisCliff Daniel DIANZOLE MOUNKANANo ratings yet
- Determinants of First Line Antiretroviral Therapy Treatment Failure Among Adult Patients On ART at Central Ethiopia: Un-Matched Case Control StudyDocument13 pagesDeterminants of First Line Antiretroviral Therapy Treatment Failure Among Adult Patients On ART at Central Ethiopia: Un-Matched Case Control Studyn.m.l.h.189No ratings yet
- ART Access-Related Barriers Faced by HIV-positiveDocument13 pagesART Access-Related Barriers Faced by HIV-positiveZay YaNo ratings yet
- 3 Non Adherence and Its Contributing PDFDocument9 pages3 Non Adherence and Its Contributing PDFODONG MARTINNo ratings yet
- 2015 Article 1098Document12 pages2015 Article 1098Irenius TenaNo ratings yet
- 2017 Article 2184Document11 pages2017 Article 2184diana sulistianNo ratings yet
- Barriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVDocument15 pagesBarriers To Early Treatment Seeking Among Patients With Sexually Transmitted Infections in A Rural Community Setting at Kaproron Health Centre IVKIU PUBLICATION AND EXTENSIONNo ratings yet
- Preventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberDocument9 pagesPreventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberKnowledge PepalaNo ratings yet
- 42B169F57392Document6 pages42B169F57392denekeNo ratings yet
- 18586-Article Text-77701-1-10-20190219Document15 pages18586-Article Text-77701-1-10-20190219AyitenewNo ratings yet
- Vake's Proposal On HepatitisDocument26 pagesVake's Proposal On HepatitisVake MtongaNo ratings yet
- Breastfeeding Counseling and SupportDocument8 pagesBreastfeeding Counseling and SupportJohanna MoralesNo ratings yet
- The Association Between Diagnosis Disclosure and Adherence To Antiretroviral Therapy Among Adolescents Living With HIV in Sub-Saharan Africa: A Protocol For Systematic Review and Meta-AnalysisDocument5 pagesThe Association Between Diagnosis Disclosure and Adherence To Antiretroviral Therapy Among Adolescents Living With HIV in Sub-Saharan Africa: A Protocol For Systematic Review and Meta-AnalysisMelkamuMeridNo ratings yet
- Tuberculosis Vih EthiopiaDocument9 pagesTuberculosis Vih Ethiopiajulma1306No ratings yet
- Ali2016 Article OutcomesOfTBTreatmentInHIVCo-iDocument9 pagesAli2016 Article OutcomesOfTBTreatmentInHIVCo-itishaNo ratings yet
- Child Health and TBDocument3 pagesChild Health and TBsoukumar8305No ratings yet
- Vih Ingreso Al Cuidado VihDocument15 pagesVih Ingreso Al Cuidado Vihsamuro625No ratings yet
- Influencing Factors To Adherence To ArvDocument8 pagesInfluencing Factors To Adherence To ArvOBIOMA LILIAN OKWUONUNo ratings yet
- Clinically Relevant Pharmacokinetic Knowledge On Antibiotic Dosing Among Intensive Care Professionals Is Insufficient: A Cross-Sectional StudyDocument9 pagesClinically Relevant Pharmacokinetic Knowledge On Antibiotic Dosing Among Intensive Care Professionals Is Insufficient: A Cross-Sectional StudyNguyễn Đức LongNo ratings yet
- My ThesisDocument8 pagesMy ThesisYirgalem YosefNo ratings yet
- Researcharticle Open AccessDocument12 pagesResearcharticle Open Accesswosen wondNo ratings yet
- Eclinicalmedicine: Contents Lists Available atDocument9 pagesEclinicalmedicine: Contents Lists Available atOmong KosongNo ratings yet
- Immunization Coverage of 12 - 23 Months Old Children and Associated Factors in Jigjiga District, Somali National Regional State, EthiopiaDocument9 pagesImmunization Coverage of 12 - 23 Months Old Children and Associated Factors in Jigjiga District, Somali National Regional State, EthiopiaAMANUEL TEREFENo ratings yet
- Zambia Study Dec 2019Document9 pagesZambia Study Dec 2019AbiodunOlaiyaPaulNo ratings yet
- First and Second Line Highly Active Anti-Retroviral Therapy Failure in HIV Infected Nigerian Children at University of Abuja Teaching Hospital Gwagwalada, NigeriaDocument6 pagesFirst and Second Line Highly Active Anti-Retroviral Therapy Failure in HIV Infected Nigerian Children at University of Abuja Teaching Hospital Gwagwalada, NigeriaPeertechz Publications Inc.No ratings yet
- 2020 Article 5324Document8 pages2020 Article 5324Sorina ElenaNo ratings yet
- BMC Medicine: Patient-Centred Tuberculosis Treatment Delivery Under Programmatic Conditions in Tanzania: A Cohort StudyDocument10 pagesBMC Medicine: Patient-Centred Tuberculosis Treatment Delivery Under Programmatic Conditions in Tanzania: A Cohort StudyNay Lin HtikeNo ratings yet
- Access N PMTCTDocument21 pagesAccess N PMTCTByaruhanga EmmanuelNo ratings yet
- Evaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictDocument17 pagesEvaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Detectable Viral Load and Human Immuno Deficiency Drug ResistanceDocument11 pagesDetectable Viral Load and Human Immuno Deficiency Drug ResistanceFelistus KanjiraNo ratings yet
- Overuse of AntibioticDocument10 pagesOveruse of AntibioticshinNo ratings yet
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicineFdo RMNo ratings yet
- 1472 6874 10 8 PDFDocument7 pages1472 6874 10 8 PDFhirsi200518No ratings yet
- Influenza Vaccination Coverage in Patients Treated With ChemotherapyDocument12 pagesInfluenza Vaccination Coverage in Patients Treated With Chemotherapyنبأ فؤاد سالمNo ratings yet
- Association of Pre-Antiretroviral Treatment Body Mass Index With Cd4 T-Lymphocyte Immune Reconstitution Among HIV-Infected Adults and AdolescentsDocument8 pagesAssociation of Pre-Antiretroviral Treatment Body Mass Index With Cd4 T-Lymphocyte Immune Reconstitution Among HIV-Infected Adults and Adolescentsadelin ransunNo ratings yet
- Adherence To Antiretroviral Therapy and The Associated Factors Among People Living With HIV/AIDS in Northern Peru: A Cross Sectional StudyDocument12 pagesAdherence To Antiretroviral Therapy and The Associated Factors Among People Living With HIV/AIDS in Northern Peru: A Cross Sectional StudyALEX AARÓN COLLAZOS FLORESNo ratings yet
- HIV Patients Retention and Attrition in Care and Determinants in EthiopiaDocument24 pagesHIV Patients Retention and Attrition in Care and Determinants in EthiopiaDouglas ChukwuNo ratings yet
- Abstract 59Document3 pagesAbstract 59Jarvis WheelerNo ratings yet
- Improving Survival With TBDocument8 pagesImproving Survival With TBdani catriaNo ratings yet
- (Pro) Ing 1, Ada Kuesioner Juga12Document8 pages(Pro) Ing 1, Ada Kuesioner Juga12ilhamNo ratings yet
- 5744cb41-031d-4226-9cea-07098cf4c210Document28 pages5744cb41-031d-4226-9cea-07098cf4c210wahyuna lidwina samosirNo ratings yet
- HIV Prevention in Primary Care Practice: A PrEP PrimerFrom EverandHIV Prevention in Primary Care Practice: A PrEP PrimerNo ratings yet
- Dyspareunia Due To A General Medical ConditionDocument18 pagesDyspareunia Due To A General Medical ConditionanisNo ratings yet
- Follow-Up of A Healthy Lifestyle Education Program (The Edal Study) : Four Years After Cessation of Randomized Controlled Trial InterventionDocument12 pagesFollow-Up of A Healthy Lifestyle Education Program (The Edal Study) : Four Years After Cessation of Randomized Controlled Trial InterventionanisNo ratings yet
- Epidemiology and Etiology of Childhood PneumoniaDocument13 pagesEpidemiology and Etiology of Childhood PneumoniaanisNo ratings yet
- Pneumonia MayoclinicDocument3 pagesPneumonia MayoclinicanisNo ratings yet
- Pulmonary Tuberculosis - Curitana BSN 2bDocument10 pagesPulmonary Tuberculosis - Curitana BSN 2bDrex CuritanaNo ratings yet
- 65wd17e Rev1 TBActionPlan 150588 Withcover PDFDocument17 pages65wd17e Rev1 TBActionPlan 150588 Withcover PDFFlorentina LucanNo ratings yet
- 20 Things That Someone With An Eating Disorder Wishes They Were Able To Tell YouDocument10 pages20 Things That Someone With An Eating Disorder Wishes They Were Able To Tell Youmorgs39No ratings yet
- Dulcolax® (Adult Supp) : ConstipationDocument8 pagesDulcolax® (Adult Supp) : ConstipationStephany Rae MamauagNo ratings yet
- Endometriosis in PregnancyDocument31 pagesEndometriosis in PregnancyRadius KusumaNo ratings yet
- Optometry: Accommodative and Binocular Dysfunctions: Prevalence in A Randomised Sample of University StudentsDocument9 pagesOptometry: Accommodative and Binocular Dysfunctions: Prevalence in A Randomised Sample of University StudentsShyannaNo ratings yet
- Nso ErcpDocument3 pagesNso Ercptry dokkNo ratings yet
- A Comparative Study of Relationship Between Vegetarians and Non-Vegetarians - Diet, Blood Pressure and Body Fat CompositionDocument3 pagesA Comparative Study of Relationship Between Vegetarians and Non-Vegetarians - Diet, Blood Pressure and Body Fat CompositionmamtakumariNo ratings yet
- Chronic Myelogenous Leukemia: The PH ChromosomeDocument1 pageChronic Myelogenous Leukemia: The PH ChromosomeJolaine ValloNo ratings yet
- Case Scenerio PneumoniaDocument8 pagesCase Scenerio PneumoniaEllen AngelNo ratings yet
- Sample Clinical Pharmacy CaseDocument41 pagesSample Clinical Pharmacy CaseLouie Fernand LegaspiNo ratings yet
- Bill of Supply/Cash Receipt: (Please Bring This Receipt For Report Collection)Document2 pagesBill of Supply/Cash Receipt: (Please Bring This Receipt For Report Collection)saurabhkatiyarNo ratings yet
- Neonatal Hypoglycemia (Infant of Diabetic Mother)Document15 pagesNeonatal Hypoglycemia (Infant of Diabetic Mother)diana rossNo ratings yet
- Morey, J. N., Boggero, I. A., Scott, A. B., & Segerstrom, S. C. (2015) - Current Directions in Stress and Human Immune FunctionDocument5 pagesMorey, J. N., Boggero, I. A., Scott, A. B., & Segerstrom, S. C. (2015) - Current Directions in Stress and Human Immune FunctionFranco Paolo Maray-GhigliottoNo ratings yet
- (Journal Q2 2023) Heart Arrhythmia Detection and Classification A Comparative StudyDocument21 pages(Journal Q2 2023) Heart Arrhythmia Detection and Classification A Comparative StudyVideo GratisNo ratings yet
- Idiopatik LeukoplakiaDocument2 pagesIdiopatik LeukoplakiaAfiyatul IsnainiNo ratings yet
- PPP - Listening C - Test 3 Question PaperDocument4 pagesPPP - Listening C - Test 3 Question PaperLina CornickNo ratings yet
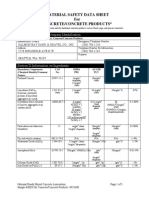
- Material Safety Data Sheet For Concrete/Concrete Products : Section I-Product and Company IdentificationDocument5 pagesMaterial Safety Data Sheet For Concrete/Concrete Products : Section I-Product and Company Identificationmalaya tripathyNo ratings yet
- Schizophrenia NotesDocument10 pagesSchizophrenia NotesJamesNo ratings yet
- Fresenius+Dialysis+Machine+Disinfection V1 0Document7 pagesFresenius+Dialysis+Machine+Disinfection V1 0Mendes NovatoNo ratings yet
- 30 Day Clean Eating PDFDocument47 pages30 Day Clean Eating PDFIreneo100% (3)
- Os 1Document3 pagesOs 1rizwanNo ratings yet
- List of New Drugs Approved in The Year 2023decDocument4 pagesList of New Drugs Approved in The Year 2023decJassu J CNo ratings yet
- Obstructed LaborDocument4 pagesObstructed LaborSojiro JiroNo ratings yet
- EpistigminDocument2 pagesEpistigminmahgadNo ratings yet
- Case Study GonorrheaDocument19 pagesCase Study GonorrheaErika ThereseNo ratings yet
- Hemiclonic Seizures - MedLink NeurologyDocument6 pagesHemiclonic Seizures - MedLink NeurologyRamo EdumNo ratings yet
- Sohail Reports PDFDocument2 pagesSohail Reports PDFMunazza SohailNo ratings yet