
Overlay Vs Template
Overlay Vs Template
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Oet Speaking British Academy 01-256-314Document59 pagesOet Speaking British Academy 01-256-314Muhammad Aleem100% (1)
- Contradictions of Plato's IdeasDocument6 pagesContradictions of Plato's Ideaskissinger2020No ratings yet
- CIE Publist 2011 FebruaryDocument11 pagesCIE Publist 2011 FebruaryMido AbdoNo ratings yet
- Assessment Template COMPLETE 30 DecemberDocument7 pagesAssessment Template COMPLETE 30 DecemberMuhammad AleemNo ratings yet
- TEACHIO OET Writing Short FormsDocument5 pagesTEACHIO OET Writing Short FormsMuhammad AleemNo ratings yet
- Ijerph 18 06356Document10 pagesIjerph 18 06356Muhammad AleemNo ratings yet
- Archive of SID: Evaluation of Acquired Cystic Kidney Disease in Patients On Hemodialysis With UltrasonographyDocument4 pagesArchive of SID: Evaluation of Acquired Cystic Kidney Disease in Patients On Hemodialysis With UltrasonographyMuhammad AleemNo ratings yet
- Correlation of Arch Length and Width To Anteroposterior Lip Position in Class I Non Extraction MalocclusionDocument4 pagesCorrelation of Arch Length and Width To Anteroposterior Lip Position in Class I Non Extraction MalocclusionMuhammad AleemNo ratings yet
- Liver Function Tests A Marker of Severity in COVID-19 PatientsDocument4 pagesLiver Function Tests A Marker of Severity in COVID-19 PatientsMuhammad AleemNo ratings yet
- Ramadan and Fasting 25th AprilDocument45 pagesRamadan and Fasting 25th AprilMuhammad AleemNo ratings yet
- Model Analysison Smart PhoneDocument4 pagesModel Analysison Smart PhoneMuhammad AleemNo ratings yet
- Technique NewDocument5 pagesTechnique NewMuhammad AleemNo ratings yet
- Instant Sto 2Document4 pagesInstant Sto 2Muhammad AleemNo ratings yet
- Autorotation & 6 SG Options FishDocument28 pagesAutorotation & 6 SG Options FishMuhammad Aleem100% (1)
- Prediction in An Ortho Surgical Case: A ReportDocument7 pagesPrediction in An Ortho Surgical Case: A ReportMuhammad AleemNo ratings yet
- Validity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyDocument10 pagesValidity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyMuhammad AleemNo ratings yet
- Autorotation Angle 2Document4 pagesAutorotation Angle 2Muhammad AleemNo ratings yet
- Benchtop Universal Testing MachineDocument8 pagesBenchtop Universal Testing Machineharan2000No ratings yet
- 18300038, Assignment 1, Bus 411Document5 pages18300038, Assignment 1, Bus 411Md RifatNo ratings yet
- MicrosoftDocument20 pagesMicrosoftSagar PatelNo ratings yet
- Lab Report No 06: Digital Signal ProcessingDocument9 pagesLab Report No 06: Digital Signal ProcessingMahnoor InamNo ratings yet
- Chiller Unit CostDocument3 pagesChiller Unit CostKullamas UdoNo ratings yet
- Li Kolar Li Et Al Research Development of Preload Technology On Angular Contact Ball Bearing of High Speed Spindle A Review (2020) PUBV 340215Document23 pagesLi Kolar Li Et Al Research Development of Preload Technology On Angular Contact Ball Bearing of High Speed Spindle A Review (2020) PUBV 340215fog900No ratings yet
- Elective 1 Chapter 6 Lesson 1Document15 pagesElective 1 Chapter 6 Lesson 1Naughty or NiceNo ratings yet
- Drive Test (Solano)Document12 pagesDrive Test (Solano)Héctor Palomino SánchezNo ratings yet
- Receptionists Competency Standard Booklet Printed PDFDocument19 pagesReceptionists Competency Standard Booklet Printed PDFMicula OanaNo ratings yet
- Isolve Sata: Product Features and BenefitsDocument2 pagesIsolve Sata: Product Features and BenefitsShah DhavalNo ratings yet
- Transportation Asset Management GuideDocument140 pagesTransportation Asset Management GuideChewfy1100% (2)
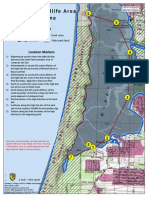
- Morro Bay Wildlife Area Hunt Zone: Map LegendDocument1 pageMorro Bay Wildlife Area Hunt Zone: Map LegendZarahNo ratings yet
- DLP PolgovDocument2 pagesDLP PolgovJuna Silawan Babatu-onNo ratings yet
- Anatomy Reviewer: Body Cavity Is Any Fluid-Filled Space in A Multicellular Organism Other Than Those of VesselsDocument3 pagesAnatomy Reviewer: Body Cavity Is Any Fluid-Filled Space in A Multicellular Organism Other Than Those of VesselsIvan LimNo ratings yet
- MIR - LML - Golovina L. I. and Yaglom I. M. - Induction in GeometryDocument134 pagesMIR - LML - Golovina L. I. and Yaglom I. M. - Induction in Geometryavast2008100% (2)
- A Survey On Intraday Traders - Google FormsDocument8 pagesA Survey On Intraday Traders - Google FormsAnju tpNo ratings yet
- Delayed Ettringite FormationDocument7 pagesDelayed Ettringite Formationvthamarai999543No ratings yet
- Pee Question BankDocument9 pagesPee Question BanklavanyaNo ratings yet
- Practicum Narrative Report FormatDocument8 pagesPracticum Narrative Report FormatJC GAMINGNo ratings yet
- Dr.R.A.Mashelkar Bio-DataDocument43 pagesDr.R.A.Mashelkar Bio-DatacalpineNo ratings yet
- Effects of Parental Warmth and Academic Pressure On Anxiety and Depression Symptoms in Chinese AdolescentsDocument11 pagesEffects of Parental Warmth and Academic Pressure On Anxiety and Depression Symptoms in Chinese AdolescentsJr SparkNo ratings yet
- E WIMA MKP 4Document11 pagesE WIMA MKP 4kmyisusNo ratings yet
- A For and Against Essay - Exercises 1Document4 pagesA For and Against Essay - Exercises 1vaisacrujirNo ratings yet
- Essential Oil Nanoemulsions As Antimicrobial Agents in FoodDocument19 pagesEssential Oil Nanoemulsions As Antimicrobial Agents in FoodpradeepqNo ratings yet
- Lucchini Poly MilanoDocument26 pagesLucchini Poly MilanoAghajaniNo ratings yet
- BATCH 1 PPT Major Project AykDocument18 pagesBATCH 1 PPT Major Project AykAliseriyashwanth24No ratings yet
- KSF V4.0 CastingDocument27 pagesKSF V4.0 CastingBobby WongNo ratings yet
- Humphree Course StabilisingDocument8 pagesHumphree Course StabilisingMatNo ratings yet




















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Oet Speaking British Academy 01-256-314Document59 pagesOet Speaking British Academy 01-256-314Muhammad Aleem100% (1)
- Contradictions of Plato's IdeasDocument6 pagesContradictions of Plato's Ideaskissinger2020No ratings yet
- CIE Publist 2011 FebruaryDocument11 pagesCIE Publist 2011 FebruaryMido AbdoNo ratings yet
- Assessment Template COMPLETE 30 DecemberDocument7 pagesAssessment Template COMPLETE 30 DecemberMuhammad AleemNo ratings yet
- TEACHIO OET Writing Short FormsDocument5 pagesTEACHIO OET Writing Short FormsMuhammad AleemNo ratings yet
- Ijerph 18 06356Document10 pagesIjerph 18 06356Muhammad AleemNo ratings yet
- Archive of SID: Evaluation of Acquired Cystic Kidney Disease in Patients On Hemodialysis With UltrasonographyDocument4 pagesArchive of SID: Evaluation of Acquired Cystic Kidney Disease in Patients On Hemodialysis With UltrasonographyMuhammad AleemNo ratings yet
- Correlation of Arch Length and Width To Anteroposterior Lip Position in Class I Non Extraction MalocclusionDocument4 pagesCorrelation of Arch Length and Width To Anteroposterior Lip Position in Class I Non Extraction MalocclusionMuhammad AleemNo ratings yet
- Liver Function Tests A Marker of Severity in COVID-19 PatientsDocument4 pagesLiver Function Tests A Marker of Severity in COVID-19 PatientsMuhammad AleemNo ratings yet
- Ramadan and Fasting 25th AprilDocument45 pagesRamadan and Fasting 25th AprilMuhammad AleemNo ratings yet
- Model Analysison Smart PhoneDocument4 pagesModel Analysison Smart PhoneMuhammad AleemNo ratings yet
- Technique NewDocument5 pagesTechnique NewMuhammad AleemNo ratings yet
- Instant Sto 2Document4 pagesInstant Sto 2Muhammad AleemNo ratings yet
- Autorotation & 6 SG Options FishDocument28 pagesAutorotation & 6 SG Options FishMuhammad Aleem100% (1)
- Prediction in An Ortho Surgical Case: A ReportDocument7 pagesPrediction in An Ortho Surgical Case: A ReportMuhammad AleemNo ratings yet
- Validity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyDocument10 pagesValidity of A Manual Soft Tissue Profile Prediction Method Following Mandibular Setback OsteotomyMuhammad AleemNo ratings yet
- Autorotation Angle 2Document4 pagesAutorotation Angle 2Muhammad AleemNo ratings yet
- Benchtop Universal Testing MachineDocument8 pagesBenchtop Universal Testing Machineharan2000No ratings yet
- 18300038, Assignment 1, Bus 411Document5 pages18300038, Assignment 1, Bus 411Md RifatNo ratings yet
- MicrosoftDocument20 pagesMicrosoftSagar PatelNo ratings yet
- Lab Report No 06: Digital Signal ProcessingDocument9 pagesLab Report No 06: Digital Signal ProcessingMahnoor InamNo ratings yet
- Chiller Unit CostDocument3 pagesChiller Unit CostKullamas UdoNo ratings yet
- Li Kolar Li Et Al Research Development of Preload Technology On Angular Contact Ball Bearing of High Speed Spindle A Review (2020) PUBV 340215Document23 pagesLi Kolar Li Et Al Research Development of Preload Technology On Angular Contact Ball Bearing of High Speed Spindle A Review (2020) PUBV 340215fog900No ratings yet
- Elective 1 Chapter 6 Lesson 1Document15 pagesElective 1 Chapter 6 Lesson 1Naughty or NiceNo ratings yet
- Drive Test (Solano)Document12 pagesDrive Test (Solano)Héctor Palomino SánchezNo ratings yet
- Receptionists Competency Standard Booklet Printed PDFDocument19 pagesReceptionists Competency Standard Booklet Printed PDFMicula OanaNo ratings yet
- Isolve Sata: Product Features and BenefitsDocument2 pagesIsolve Sata: Product Features and BenefitsShah DhavalNo ratings yet
- Transportation Asset Management GuideDocument140 pagesTransportation Asset Management GuideChewfy1100% (2)
- Morro Bay Wildlife Area Hunt Zone: Map LegendDocument1 pageMorro Bay Wildlife Area Hunt Zone: Map LegendZarahNo ratings yet
- DLP PolgovDocument2 pagesDLP PolgovJuna Silawan Babatu-onNo ratings yet
- Anatomy Reviewer: Body Cavity Is Any Fluid-Filled Space in A Multicellular Organism Other Than Those of VesselsDocument3 pagesAnatomy Reviewer: Body Cavity Is Any Fluid-Filled Space in A Multicellular Organism Other Than Those of VesselsIvan LimNo ratings yet
- MIR - LML - Golovina L. I. and Yaglom I. M. - Induction in GeometryDocument134 pagesMIR - LML - Golovina L. I. and Yaglom I. M. - Induction in Geometryavast2008100% (2)
- A Survey On Intraday Traders - Google FormsDocument8 pagesA Survey On Intraday Traders - Google FormsAnju tpNo ratings yet
- Delayed Ettringite FormationDocument7 pagesDelayed Ettringite Formationvthamarai999543No ratings yet
- Pee Question BankDocument9 pagesPee Question BanklavanyaNo ratings yet
- Practicum Narrative Report FormatDocument8 pagesPracticum Narrative Report FormatJC GAMINGNo ratings yet
- Dr.R.A.Mashelkar Bio-DataDocument43 pagesDr.R.A.Mashelkar Bio-DatacalpineNo ratings yet
- Effects of Parental Warmth and Academic Pressure On Anxiety and Depression Symptoms in Chinese AdolescentsDocument11 pagesEffects of Parental Warmth and Academic Pressure On Anxiety and Depression Symptoms in Chinese AdolescentsJr SparkNo ratings yet
- E WIMA MKP 4Document11 pagesE WIMA MKP 4kmyisusNo ratings yet
- A For and Against Essay - Exercises 1Document4 pagesA For and Against Essay - Exercises 1vaisacrujirNo ratings yet
- Essential Oil Nanoemulsions As Antimicrobial Agents in FoodDocument19 pagesEssential Oil Nanoemulsions As Antimicrobial Agents in FoodpradeepqNo ratings yet
- Lucchini Poly MilanoDocument26 pagesLucchini Poly MilanoAghajaniNo ratings yet
- BATCH 1 PPT Major Project AykDocument18 pagesBATCH 1 PPT Major Project AykAliseriyashwanth24No ratings yet
- KSF V4.0 CastingDocument27 pagesKSF V4.0 CastingBobby WongNo ratings yet
- Humphree Course StabilisingDocument8 pagesHumphree Course StabilisingMatNo ratings yet