
RV Infarction
RV Infarction
You might also like
- Cycle SyncingDocument43 pagesCycle SyncingHeShot MeDown100% (1)
- MC Case PDFDocument20 pagesMC Case PDFShivani KarkeraNo ratings yet
- Epson 3800 3880 SMDocument306 pagesEpson 3800 3880 SMIon IonutNo ratings yet
- Zoom Final PA CathetherDocument45 pagesZoom Final PA Cathetherhasanafridi.mechNo ratings yet
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- RV InfarctDocument2 pagesRV Infarctintrovoyz041No ratings yet
- Cardiothoracics ReviewDocument44 pagesCardiothoracics ReviewGrace LNo ratings yet
- Atrial Septal Defects: Imaging Conference December 10, 2008 Angela Morello, M.DDocument49 pagesAtrial Septal Defects: Imaging Conference December 10, 2008 Angela Morello, M.Dkiritokazuto35No ratings yet
- Aortic Stenosis:: Updates in Diagnosis & ManagementDocument48 pagesAortic Stenosis:: Updates in Diagnosis & ManagementCuca PcelaNo ratings yet
- Asd - TheDocument40 pagesAsd - TheguidanceNo ratings yet
- Cardio 2020 MedantaDocument454 pagesCardio 2020 Medantadoc339No ratings yet
- Tetralogy of FallotDocument41 pagesTetralogy of Fallotthecount28991No ratings yet
- 991111 EUS教學 (6) 重點式急診心臟超音波之應用Document67 pages991111 EUS教學 (6) 重點式急診心臟超音波之應用juice119100% (5)
- Hemodynamic MonitoringDocument117 pagesHemodynamic MonitoringItinderpal SinghNo ratings yet
- Valvular UpdateDocument44 pagesValvular UpdateUlmi FadillahNo ratings yet
- Valvular Heart Diseases: Elias S. (MD+) March 2015 DBUDocument68 pagesValvular Heart Diseases: Elias S. (MD+) March 2015 DBUMed PoxNo ratings yet
- Aortic Regurgitation by DR DilmoDocument37 pagesAortic Regurgitation by DR Dilmosinan kNo ratings yet
- Sat 1315-1415 Cardiac AngiogDocument47 pagesSat 1315-1415 Cardiac AngiogbenypermadiNo ratings yet
- Cardiacmanuveres 160818075238Document56 pagesCardiacmanuveres 160818075238Rapmle PrasadNo ratings yet
- CCPACatheter Basics 07 MedicineDocument44 pagesCCPACatheter Basics 07 MedicinerinbijoyNo ratings yet
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument76 pagesAdult Congenital Heart Disease Board ReviewOQAB13No ratings yet
- AMIwithnormal ECGDocument42 pagesAMIwithnormal ECGamirchughtaiNo ratings yet
- Achd LectureDocument48 pagesAchd LecturedrmdsaeedNo ratings yet
- Aortic RegurgitationDocument41 pagesAortic RegurgitationMedi PutraNo ratings yet
- Cath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDocument38 pagesCath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDr. TomNo ratings yet
- Hemodynamic Failure March 2016Document61 pagesHemodynamic Failure March 2016Adriana VillarrealNo ratings yet
- CMR Guide CHD 2014 PDFDocument105 pagesCMR Guide CHD 2014 PDFBasemAlharbiNo ratings yet
- Valvular DiseasesDocument45 pagesValvular DiseasesKen WayNo ratings yet
- Mitral Stenosis Mitral RegurgitationDocument66 pagesMitral Stenosis Mitral RegurgitationMarshellaTriPradilagaNo ratings yet
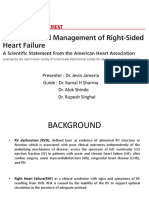
- Evaluation and Management of Right-SidedDocument65 pagesEvaluation and Management of Right-SidedJevin JameriaNo ratings yet
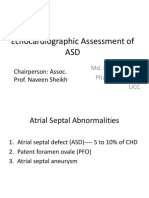
- Echocardiographic Assessment of ASD: Chairperson: Assoc. Prof. Naveen SheikhDocument53 pagesEchocardiographic Assessment of ASD: Chairperson: Assoc. Prof. Naveen SheikhWyahmp WyahmpNo ratings yet
- Echo PresentationDocument36 pagesEcho PresentationSalman MajidNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- 2019 - MCardiology - Clinical Features of Val HT 2019 2Document72 pages2019 - MCardiology - Clinical Features of Val HT 2019 2Vaenusha MuruganNo ratings yet
- Pulmonary Artery Catheters and Hemodynamic MonitoringDocument32 pagesPulmonary Artery Catheters and Hemodynamic Monitoringjpsahni100% (1)
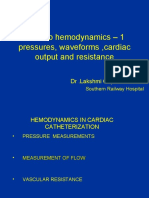
- DR Lakshmi MMM 2009 FINALDocument33 pagesDR Lakshmi MMM 2009 FINALsubha shreeNo ratings yet
- Asessement of RV Function: by Rakshitha NayakDocument41 pagesAsessement of RV Function: by Rakshitha NayakSAI HARSHITHA PulluruNo ratings yet
- Hemodaynamic Monitoring KHDocument91 pagesHemodaynamic Monitoring KHomar kmr97No ratings yet
- Valvular Heart Disease To TW FinalDocument13 pagesValvular Heart Disease To TW FinalMohammed ElSayedNo ratings yet
- Thoracicanaesthesia 180527045849Document122 pagesThoracicanaesthesia 180527045849rinduNo ratings yet
- ArrhythmiaDocument59 pagesArrhythmiaUWIMANA Jean ClaudeNo ratings yet
- Supraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, MysoreDocument81 pagesSupraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, Mysorerobinjohn06No ratings yet
- Swan Ganz FinalDocument36 pagesSwan Ganz FinalDanial HassanNo ratings yet
- Physiologic Basis For Hemodynamic MonitoringDocument36 pagesPhysiologic Basis For Hemodynamic MonitoringEshwar Chandra VidyasagarNo ratings yet
- Jugular Venous Pressure: It's Easier Than It LooksDocument25 pagesJugular Venous Pressure: It's Easier Than It LooksManggarsari SdwqNo ratings yet
- Hemodynamic Monitoring Riding The Waves in California Renee SmithDocument30 pagesHemodynamic Monitoring Riding The Waves in California Renee SmithSanaz NikiNo ratings yet
- DR - Sfeir Principles+of+Cardiac+SurgeryDocument91 pagesDR - Sfeir Principles+of+Cardiac+SurgeryFrida AtallahNo ratings yet
- ELECTROCARDIOGRAMDocument63 pagesELECTROCARDIOGRAMMbah GapinbissiNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- RHF CausesDocument25 pagesRHF CausesKarozh Jalal DuskiNo ratings yet
- 113959Document19 pages113959Andrea San AntonioNo ratings yet
- Cardiogenic Shock and Pulmonary EdemaDocument41 pagesCardiogenic Shock and Pulmonary EdemaChristian Gallardo, MD100% (7)
- CC, CVP MonitoringDocument5 pagesCC, CVP MonitoringM7md Al-HuwaitiNo ratings yet
- Utz - Focus, DVT, RenalDocument112 pagesUtz - Focus, DVT, RenalJuster AbuegNo ratings yet
- Hemodynamic Monitoring: Amber Arsenault, MSN, FNP-BC, RNDocument41 pagesHemodynamic Monitoring: Amber Arsenault, MSN, FNP-BC, RNmandy nationsNo ratings yet
- Assessment of Right Ventricular FunctionDocument41 pagesAssessment of Right Ventricular FunctionAditya MadhavpeddiNo ratings yet
- Rosenberg Circulatory Assist DevicesDocument61 pagesRosenberg Circulatory Assist DevicesMilisha Albro100% (1)
- Mitral StenosisDocument17 pagesMitral StenosisMuhammad Alauddin Sarwar100% (9)
- Natalya Master CardioDocument71 pagesNatalya Master CardioTaman Hoang100% (1)
- Law of Mother Earth BoliviaDocument3 pagesLaw of Mother Earth Boliviarahul banerjeeNo ratings yet
- Industrial RoboticsDocument77 pagesIndustrial RoboticsIslam Fouad100% (4)
- WiringDocument147 pagesWiringYovani Cortes50% (2)
- Transport Phenomena: τ =μ dv dyDocument2 pagesTransport Phenomena: τ =μ dv dySYED ASGHAR ALI SULTANNo ratings yet
- Ignatian SpiritualityDocument16 pagesIgnatian SpiritualityMihai Frentz100% (2)
- Everlast INTERVAL TRAINING ROUND TIMER PDFDocument1 pageEverlast INTERVAL TRAINING ROUND TIMER PDFanniaanniaNo ratings yet
- Technical Specification: 1) Filter Feed Pump With Motor 1 NosDocument4 pagesTechnical Specification: 1) Filter Feed Pump With Motor 1 NosKamatchi NathanNo ratings yet
- CESCCommunityProjectPlan Brgy - MacarioDaconDocument6 pagesCESCCommunityProjectPlan Brgy - MacarioDaconKennedy BalmoriNo ratings yet
- Quatre Agro Enterprise Private LimitedDocument25 pagesQuatre Agro Enterprise Private Limitedp23pallavNo ratings yet
- Catalogo ColonneDocument140 pagesCatalogo Colonneapi-18378576No ratings yet
- Rotorcraft Aerodynamics: Muhammad Abdullah Tahir 180101034 Aero 17 (A)Document15 pagesRotorcraft Aerodynamics: Muhammad Abdullah Tahir 180101034 Aero 17 (A)Abdullah CheemaNo ratings yet
- Biology Investigatory Project: Malaria: Its Effects and CausesDocument17 pagesBiology Investigatory Project: Malaria: Its Effects and CausesRishi KeshavNo ratings yet
- He Is A Chocolate Lover: Kamaladevi RengasamyDocument4 pagesHe Is A Chocolate Lover: Kamaladevi RengasamyKamala DeviNo ratings yet
- S900 Inverter User Manualv1.5 PDFDocument86 pagesS900 Inverter User Manualv1.5 PDFOmar ShadyNo ratings yet
- The Evolution of Video Streaming and Digital Content DeliveryDocument8 pagesThe Evolution of Video Streaming and Digital Content DeliveryBrookings InstitutionNo ratings yet
- Uremic EncephalophatyDocument48 pagesUremic EncephalophatySindi LadayaNo ratings yet
- New WITTMANN Robots For Large and Small Injection Molding MachinesDocument4 pagesNew WITTMANN Robots For Large and Small Injection Molding MachinesMonark HunyNo ratings yet
- Schiavi Enc Met Page015Document1 pageSchiavi Enc Met Page015Adel AdelNo ratings yet
- Gennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's IndianDocument130 pagesGennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's Indiancodonauta100% (1)
- 3.1 Clothing Performance Requirements - March 22Document60 pages3.1 Clothing Performance Requirements - March 22Rohan KabirNo ratings yet
- Bsme 3-B: Me 114 - Heat Transfer Bachelor of Science in Mechanical EngineeringDocument3 pagesBsme 3-B: Me 114 - Heat Transfer Bachelor of Science in Mechanical EngineeringJethro Briza GaneloNo ratings yet
- WATERGUARD 45 (Acrylic Waterproofing Coating)Document3 pagesWATERGUARD 45 (Acrylic Waterproofing Coating)Santosh Kumar PatnaikNo ratings yet
- LTE TDD - Network - Export - 2018 - 07 - 04Document3,760 pagesLTE TDD - Network - Export - 2018 - 07 - 04saadNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- Structural Engineering Professor Step III: Ucsd Academic Biography/Bibliography FormDocument30 pagesStructural Engineering Professor Step III: Ucsd Academic Biography/Bibliography FormCesar Paul Purihuaman MoraNo ratings yet
- ManvantaraDocument3 pagesManvantaraafterragnarokNo ratings yet
- Visual Storytelling The Digital Video Documentary - Original PDFDocument44 pagesVisual Storytelling The Digital Video Documentary - Original PDFjparanoti100% (1)






















































































Download as pdf or txt
You might also like
- Cycle SyncingDocument43 pagesCycle SyncingHeShot MeDown100% (1)
- MC Case PDFDocument20 pagesMC Case PDFShivani KarkeraNo ratings yet
- Epson 3800 3880 SMDocument306 pagesEpson 3800 3880 SMIon IonutNo ratings yet
- Zoom Final PA CathetherDocument45 pagesZoom Final PA Cathetherhasanafridi.mechNo ratings yet
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- RV InfarctDocument2 pagesRV Infarctintrovoyz041No ratings yet
- Cardiothoracics ReviewDocument44 pagesCardiothoracics ReviewGrace LNo ratings yet
- Atrial Septal Defects: Imaging Conference December 10, 2008 Angela Morello, M.DDocument49 pagesAtrial Septal Defects: Imaging Conference December 10, 2008 Angela Morello, M.Dkiritokazuto35No ratings yet
- Aortic Stenosis:: Updates in Diagnosis & ManagementDocument48 pagesAortic Stenosis:: Updates in Diagnosis & ManagementCuca PcelaNo ratings yet
- Asd - TheDocument40 pagesAsd - TheguidanceNo ratings yet
- Cardio 2020 MedantaDocument454 pagesCardio 2020 Medantadoc339No ratings yet
- Tetralogy of FallotDocument41 pagesTetralogy of Fallotthecount28991No ratings yet
- 991111 EUS教學 (6) 重點式急診心臟超音波之應用Document67 pages991111 EUS教學 (6) 重點式急診心臟超音波之應用juice119100% (5)
- Hemodynamic MonitoringDocument117 pagesHemodynamic MonitoringItinderpal SinghNo ratings yet
- Valvular UpdateDocument44 pagesValvular UpdateUlmi FadillahNo ratings yet
- Valvular Heart Diseases: Elias S. (MD+) March 2015 DBUDocument68 pagesValvular Heart Diseases: Elias S. (MD+) March 2015 DBUMed PoxNo ratings yet
- Aortic Regurgitation by DR DilmoDocument37 pagesAortic Regurgitation by DR Dilmosinan kNo ratings yet
- Sat 1315-1415 Cardiac AngiogDocument47 pagesSat 1315-1415 Cardiac AngiogbenypermadiNo ratings yet
- Cardiacmanuveres 160818075238Document56 pagesCardiacmanuveres 160818075238Rapmle PrasadNo ratings yet
- CCPACatheter Basics 07 MedicineDocument44 pagesCCPACatheter Basics 07 MedicinerinbijoyNo ratings yet
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument76 pagesAdult Congenital Heart Disease Board ReviewOQAB13No ratings yet
- AMIwithnormal ECGDocument42 pagesAMIwithnormal ECGamirchughtaiNo ratings yet
- Achd LectureDocument48 pagesAchd LecturedrmdsaeedNo ratings yet
- Aortic RegurgitationDocument41 pagesAortic RegurgitationMedi PutraNo ratings yet
- Cath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDocument38 pagesCath Lab Essentials: Basic Hemodynamics For The Cath Lab and ICUDr. TomNo ratings yet
- Hemodynamic Failure March 2016Document61 pagesHemodynamic Failure March 2016Adriana VillarrealNo ratings yet
- CMR Guide CHD 2014 PDFDocument105 pagesCMR Guide CHD 2014 PDFBasemAlharbiNo ratings yet
- Valvular DiseasesDocument45 pagesValvular DiseasesKen WayNo ratings yet
- Mitral Stenosis Mitral RegurgitationDocument66 pagesMitral Stenosis Mitral RegurgitationMarshellaTriPradilagaNo ratings yet
- Evaluation and Management of Right-SidedDocument65 pagesEvaluation and Management of Right-SidedJevin JameriaNo ratings yet
- Echocardiographic Assessment of ASD: Chairperson: Assoc. Prof. Naveen SheikhDocument53 pagesEchocardiographic Assessment of ASD: Chairperson: Assoc. Prof. Naveen SheikhWyahmp WyahmpNo ratings yet
- Echo PresentationDocument36 pagesEcho PresentationSalman MajidNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- 2019 - MCardiology - Clinical Features of Val HT 2019 2Document72 pages2019 - MCardiology - Clinical Features of Val HT 2019 2Vaenusha MuruganNo ratings yet
- Pulmonary Artery Catheters and Hemodynamic MonitoringDocument32 pagesPulmonary Artery Catheters and Hemodynamic Monitoringjpsahni100% (1)
- DR Lakshmi MMM 2009 FINALDocument33 pagesDR Lakshmi MMM 2009 FINALsubha shreeNo ratings yet
- Asessement of RV Function: by Rakshitha NayakDocument41 pagesAsessement of RV Function: by Rakshitha NayakSAI HARSHITHA PulluruNo ratings yet
- Hemodaynamic Monitoring KHDocument91 pagesHemodaynamic Monitoring KHomar kmr97No ratings yet
- Valvular Heart Disease To TW FinalDocument13 pagesValvular Heart Disease To TW FinalMohammed ElSayedNo ratings yet
- Thoracicanaesthesia 180527045849Document122 pagesThoracicanaesthesia 180527045849rinduNo ratings yet
- ArrhythmiaDocument59 pagesArrhythmiaUWIMANA Jean ClaudeNo ratings yet
- Supraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, MysoreDocument81 pagesSupraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, Mysorerobinjohn06No ratings yet
- Swan Ganz FinalDocument36 pagesSwan Ganz FinalDanial HassanNo ratings yet
- Physiologic Basis For Hemodynamic MonitoringDocument36 pagesPhysiologic Basis For Hemodynamic MonitoringEshwar Chandra VidyasagarNo ratings yet
- Jugular Venous Pressure: It's Easier Than It LooksDocument25 pagesJugular Venous Pressure: It's Easier Than It LooksManggarsari SdwqNo ratings yet
- Hemodynamic Monitoring Riding The Waves in California Renee SmithDocument30 pagesHemodynamic Monitoring Riding The Waves in California Renee SmithSanaz NikiNo ratings yet
- DR - Sfeir Principles+of+Cardiac+SurgeryDocument91 pagesDR - Sfeir Principles+of+Cardiac+SurgeryFrida AtallahNo ratings yet
- ELECTROCARDIOGRAMDocument63 pagesELECTROCARDIOGRAMMbah GapinbissiNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- RHF CausesDocument25 pagesRHF CausesKarozh Jalal DuskiNo ratings yet
- 113959Document19 pages113959Andrea San AntonioNo ratings yet
- Cardiogenic Shock and Pulmonary EdemaDocument41 pagesCardiogenic Shock and Pulmonary EdemaChristian Gallardo, MD100% (7)
- CC, CVP MonitoringDocument5 pagesCC, CVP MonitoringM7md Al-HuwaitiNo ratings yet
- Utz - Focus, DVT, RenalDocument112 pagesUtz - Focus, DVT, RenalJuster AbuegNo ratings yet
- Hemodynamic Monitoring: Amber Arsenault, MSN, FNP-BC, RNDocument41 pagesHemodynamic Monitoring: Amber Arsenault, MSN, FNP-BC, RNmandy nationsNo ratings yet
- Assessment of Right Ventricular FunctionDocument41 pagesAssessment of Right Ventricular FunctionAditya MadhavpeddiNo ratings yet
- Rosenberg Circulatory Assist DevicesDocument61 pagesRosenberg Circulatory Assist DevicesMilisha Albro100% (1)
- Mitral StenosisDocument17 pagesMitral StenosisMuhammad Alauddin Sarwar100% (9)
- Natalya Master CardioDocument71 pagesNatalya Master CardioTaman Hoang100% (1)
- Law of Mother Earth BoliviaDocument3 pagesLaw of Mother Earth Boliviarahul banerjeeNo ratings yet
- Industrial RoboticsDocument77 pagesIndustrial RoboticsIslam Fouad100% (4)
- WiringDocument147 pagesWiringYovani Cortes50% (2)
- Transport Phenomena: τ =μ dv dyDocument2 pagesTransport Phenomena: τ =μ dv dySYED ASGHAR ALI SULTANNo ratings yet
- Ignatian SpiritualityDocument16 pagesIgnatian SpiritualityMihai Frentz100% (2)
- Everlast INTERVAL TRAINING ROUND TIMER PDFDocument1 pageEverlast INTERVAL TRAINING ROUND TIMER PDFanniaanniaNo ratings yet
- Technical Specification: 1) Filter Feed Pump With Motor 1 NosDocument4 pagesTechnical Specification: 1) Filter Feed Pump With Motor 1 NosKamatchi NathanNo ratings yet
- CESCCommunityProjectPlan Brgy - MacarioDaconDocument6 pagesCESCCommunityProjectPlan Brgy - MacarioDaconKennedy BalmoriNo ratings yet
- Quatre Agro Enterprise Private LimitedDocument25 pagesQuatre Agro Enterprise Private Limitedp23pallavNo ratings yet
- Catalogo ColonneDocument140 pagesCatalogo Colonneapi-18378576No ratings yet
- Rotorcraft Aerodynamics: Muhammad Abdullah Tahir 180101034 Aero 17 (A)Document15 pagesRotorcraft Aerodynamics: Muhammad Abdullah Tahir 180101034 Aero 17 (A)Abdullah CheemaNo ratings yet
- Biology Investigatory Project: Malaria: Its Effects and CausesDocument17 pagesBiology Investigatory Project: Malaria: Its Effects and CausesRishi KeshavNo ratings yet
- He Is A Chocolate Lover: Kamaladevi RengasamyDocument4 pagesHe Is A Chocolate Lover: Kamaladevi RengasamyKamala DeviNo ratings yet
- S900 Inverter User Manualv1.5 PDFDocument86 pagesS900 Inverter User Manualv1.5 PDFOmar ShadyNo ratings yet
- The Evolution of Video Streaming and Digital Content DeliveryDocument8 pagesThe Evolution of Video Streaming and Digital Content DeliveryBrookings InstitutionNo ratings yet
- Uremic EncephalophatyDocument48 pagesUremic EncephalophatySindi LadayaNo ratings yet
- New WITTMANN Robots For Large and Small Injection Molding MachinesDocument4 pagesNew WITTMANN Robots For Large and Small Injection Molding MachinesMonark HunyNo ratings yet
- Schiavi Enc Met Page015Document1 pageSchiavi Enc Met Page015Adel AdelNo ratings yet
- Gennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's IndianDocument130 pagesGennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's Indiancodonauta100% (1)
- 3.1 Clothing Performance Requirements - March 22Document60 pages3.1 Clothing Performance Requirements - March 22Rohan KabirNo ratings yet
- Bsme 3-B: Me 114 - Heat Transfer Bachelor of Science in Mechanical EngineeringDocument3 pagesBsme 3-B: Me 114 - Heat Transfer Bachelor of Science in Mechanical EngineeringJethro Briza GaneloNo ratings yet
- WATERGUARD 45 (Acrylic Waterproofing Coating)Document3 pagesWATERGUARD 45 (Acrylic Waterproofing Coating)Santosh Kumar PatnaikNo ratings yet
- LTE TDD - Network - Export - 2018 - 07 - 04Document3,760 pagesLTE TDD - Network - Export - 2018 - 07 - 04saadNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- Structural Engineering Professor Step III: Ucsd Academic Biography/Bibliography FormDocument30 pagesStructural Engineering Professor Step III: Ucsd Academic Biography/Bibliography FormCesar Paul Purihuaman MoraNo ratings yet
- ManvantaraDocument3 pagesManvantaraafterragnarokNo ratings yet
- Visual Storytelling The Digital Video Documentary - Original PDFDocument44 pagesVisual Storytelling The Digital Video Documentary - Original PDFjparanoti100% (1)