Download as pdf or txt
You might also like
- SFMA Shoulder Corrective Exercises by SportsRehabExpert - Com (C) 2010Document9 pagesSFMA Shoulder Corrective Exercises by SportsRehabExpert - Com (C) 2010Zachary Lee100% (3)
- Punters BibleDocument57 pagesPunters BibleFloat Kgb50% (2)
- Should College Athletes Be Paid - FinalDocument7 pagesShould College Athletes Be Paid - Finalapi-509669602No ratings yet
- Injury Patterns, Risk Factors, and Return To Sport in Brazilian Jiu Jitsu A Cross Sectional Study of 1140 AthletesDocument9 pagesInjury Patterns, Risk Factors, and Return To Sport in Brazilian Jiu Jitsu A Cross Sectional Study of 1140 Athletesvr9vwbbx9hNo ratings yet
- 84524-Texto Del Artículo-310829-1-10-20210819Document7 pages84524-Texto Del Artículo-310829-1-10-20210819Yosmar QuintanaNo ratings yet
- Prevalence and Pattern of Musculoskeletal Injuries Among Amateur Basketball Players in Bowen University Teaching Hospital and Ladoke Akintola University of Technology Ogbomosho EditedDocument25 pagesPrevalence and Pattern of Musculoskeletal Injuries Among Amateur Basketball Players in Bowen University Teaching Hospital and Ladoke Akintola University of Technology Ogbomosho Editednwogu.kamsiyoNo ratings yet
- Prevalence and Pattern of Musculoskeletal Injuries Among Amateur Basketball Players in Bowen University Teaching Hospital and Ladoke Akintola University of Technology OgbomoshoDocument29 pagesPrevalence and Pattern of Musculoskeletal Injuries Among Amateur Basketball Players in Bowen University Teaching Hospital and Ladoke Akintola University of Technology Ogbomoshonwogu.kamsiyoNo ratings yet
- Epidemiology of Injuries During Judo TournamentsDocument14 pagesEpidemiology of Injuries During Judo TournamentsNico Duran CostaNo ratings yet
- Prevalence and Pattern of Musculoskeletal Injuries Among Amateur Basketball Players in Bowen University Teaching Hospital and Ladoke Akintola University of Technology Ogbomosho CorrectedDocument26 pagesPrevalence and Pattern of Musculoskeletal Injuries Among Amateur Basketball Players in Bowen University Teaching Hospital and Ladoke Akintola University of Technology Ogbomosho Correctednwogu.kamsiyoNo ratings yet
- Injury in Brazilian Jiu-Jitsu TrainingDocument8 pagesInjury in Brazilian Jiu-Jitsu Trainingvr9vwbbx9hNo ratings yet
- 2018 Article 150Document8 pages2018 Article 150Saffa AzharaaniNo ratings yet
- Epidemiology of Injuries in Young Volleyball Athletes: A Systematic ReviewDocument9 pagesEpidemiology of Injuries in Young Volleyball Athletes: A Systematic Reviewgonzalo osorioNo ratings yet
- Sport InjuriesDocument8 pagesSport InjuriesmikudadoNo ratings yet
- Injury Prevalence in Brazilian Jiu-Jitsu and Mitigation Strategies For Brazilian Jiu-Jitsu Practitioners and Instructors A Literature ReviewDocument44 pagesInjury Prevalence in Brazilian Jiu-Jitsu and Mitigation Strategies For Brazilian Jiu-Jitsu Practitioners and Instructors A Literature Reviewvr9vwbbx9hNo ratings yet
- Sports-Related Injuries in Athletes With Disabilities: ReviewDocument12 pagesSports-Related Injuries in Athletes With Disabilities: Reviewangelica barrazaNo ratings yet
- BJJ INJURIES Orthopaedic Journal of Sports Medicine-2014-ScogginDocument7 pagesBJJ INJURIES Orthopaedic Journal of Sports Medicine-2014-ScogginSNo ratings yet
- Current Review of Injuries Sustained in Mixed Martial Arts (MMA)Document2 pagesCurrent Review of Injuries Sustained in Mixed Martial Arts (MMA)tastytanyaNo ratings yet
- Factors That Influence Injuries Occurrence in Jiu-Jitsu Competitors For ReferenceDocument9 pagesFactors That Influence Injuries Occurrence in Jiu-Jitsu Competitors For Referencevr9vwbbx9hNo ratings yet
- Physical Therapy in Sport: Ilana N. Ackerman, Megan A. Bohensky, Joanne L. Kemp, Richard de SteigerDocument7 pagesPhysical Therapy in Sport: Ilana N. Ackerman, Megan A. Bohensky, Joanne L. Kemp, Richard de SteigerFloriqueNo ratings yet
- Injury Incidence Characteristics and Timing in AmaDocument11 pagesInjury Incidence Characteristics and Timing in AmaDale NewtonNo ratings yet
- Epidemiology of School Fractures: A 1-Year Experience in Greek Facilitation ClassesDocument10 pagesEpidemiology of School Fractures: A 1-Year Experience in Greek Facilitation Classesanon_634779017No ratings yet
- Epidemiology of Sports-Related Musculoskeletal Injuries in Young Athletes in United StatesDocument7 pagesEpidemiology of Sports-Related Musculoskeletal Injuries in Young Athletes in United StatesPatrick JeffersonNo ratings yet
- Cervantes Et Al 2021Document7 pagesCervantes Et Al 2021henriquetaranNo ratings yet
- Prevalência de Lesões em Atletas de Brazilian Jiu-Jitsu Comparação Entre Diferentes Níveis CompetitivosDocument10 pagesPrevalência de Lesões em Atletas de Brazilian Jiu-Jitsu Comparação Entre Diferentes Níveis CompetitivosLuadoMar Foto&ArteNo ratings yet
- Injuries in Martial ArtsDocument6 pagesInjuries in Martial ArtsLucas CardealNo ratings yet
- Incidencia de Lesiones en El LCA en Atletas AdolescentesDocument11 pagesIncidencia de Lesiones en El LCA en Atletas AdolescentesAna Paula TorresNo ratings yet
- A Novel Approach To Enhance ACL Injury PreventionDocument6 pagesA Novel Approach To Enhance ACL Injury PreventionFelipe SaoNo ratings yet
- Injuries Among Judokas During CompetitionDocument6 pagesInjuries Among Judokas During CompetitionMaria MaríaNo ratings yet
- Importance of Sports Medicine in Prevention of Overused Injuries in Rugby in CameroonDocument4 pagesImportance of Sports Medicine in Prevention of Overused Injuries in Rugby in CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Injuries in National Olympic Level Judo Athletes: An Epidemiological StudyDocument8 pagesInjuries in National Olympic Level Judo Athletes: An Epidemiological StudyMaria MaríaNo ratings yet
- Injury Prevention in Youth Sports.Document5 pagesInjury Prevention in Youth Sports.drmanupvNo ratings yet
- Injury Patterns in Swedish Elite Athletics Annual Incidence, Injury Types and Risk FactorsDocument14 pagesInjury Patterns in Swedish Elite Athletics Annual Incidence, Injury Types and Risk FactorsJairBurboaNo ratings yet
- Back Pain and Body Posture of Non - Professional Brazilian Jiu-Jitsu PractitionersDocument13 pagesBack Pain and Body Posture of Non - Professional Brazilian Jiu-Jitsu Practitionersvr9vwbbx9hNo ratings yet
- 2018 Risk Factors For Musculoskeletal Injuries in Elite Junior Tennis PlayerDocument8 pages2018 Risk Factors For Musculoskeletal Injuries in Elite Junior Tennis Playerktan.lboroNo ratings yet
- Orthopaedic Injuries in Equestrian Sports: A Current Concepts ReviewDocument7 pagesOrthopaedic Injuries in Equestrian Sports: A Current Concepts ReviewJuanjo AlvarezNo ratings yet
- Final DraftDocument9 pagesFinal Draftapi-680733184No ratings yet
- SM October 2021 AbdallahDocument8 pagesSM October 2021 AbdallahQuenton CompasNo ratings yet
- 1 s2.0 S2095254621000545 MainDocument11 pages1 s2.0 S2095254621000545 Mainmarcus souzaNo ratings yet
- Lesiones en La AUDLDocument10 pagesLesiones en La AUDLJorge Andres Suarez CameroNo ratings yet
- 1 s2.0 S2095254612000452 Main PDFDocument10 pages1 s2.0 S2095254612000452 Main PDFanettepardedeNo ratings yet
- Epidemiology of NCAA Bone Stress Injuries A Comparison of Athletes in Divisions I, II, and IIIDocument7 pagesEpidemiology of NCAA Bone Stress Injuries A Comparison of Athletes in Divisions I, II, and IIIMarliNo ratings yet
- Sci 2Document7 pagesSci 2anna widiaNo ratings yet
- Handball Scandinavian JournalDocument8 pagesHandball Scandinavian JournalnetoNo ratings yet
- Injuries and Complaints in The Brazilian National Volleyball Male Team: A Case StudyDocument9 pagesInjuries and Complaints in The Brazilian National Volleyball Male Team: A Case Studygonzalo osorioNo ratings yet
- A Review of The Benefits and Risks Associated With The Practice of Martial ArtsDocument15 pagesA Review of The Benefits and Risks Associated With The Practice of Martial ArtsAssessoria AcademicaNo ratings yet
- Finalresearchreport JBMDocument23 pagesFinalresearchreport JBMapi-289445562No ratings yet
- Epidemiology of Knee Injuries Among Boys and Girls in US High School AthleticsDocument7 pagesEpidemiology of Knee Injuries Among Boys and Girls in US High School AthleticsbomgorilaoNo ratings yet
- 2018 Una Revisión de Una Década de Epidemiología de Lesiones de La Unión de Rugby 2007-2017.Document5 pages2018 Una Revisión de Una Década de Epidemiología de Lesiones de La Unión de Rugby 2007-2017.contact.movementsiteNo ratings yet
- 156.full (1) Badminton InjuriesDocument5 pages156.full (1) Badminton InjuriesRaul ValldecabresNo ratings yet
- International Olympic Committee ConsensusDocument18 pagesInternational Olympic Committee ConsensusGabriella CananNo ratings yet
- Kamitani 2013Document8 pagesKamitani 2013Maria MaríaNo ratings yet
- J PTSP 2015 02 003Document26 pagesJ PTSP 2015 02 003Paula Pérez EspinosaNo ratings yet
- Sport Injuries of Karate During Training An Epidemiologic Study in IranDocument3 pagesSport Injuries of Karate During Training An Epidemiologic Study in Irangerardo davidNo ratings yet
- Psychology of Sport Injury Rehabilitation A Review of Models and Interventions - AspDocument17 pagesPsychology of Sport Injury Rehabilitation A Review of Models and Interventions - AspKoffi Gábor50% (2)
- Art 4Document7 pagesArt 4Cláudia SilvaNo ratings yet
- What's New in Sports Medicine (Primary Care) - UpToDateDocument8 pagesWhat's New in Sports Medicine (Primary Care) - UpToDateManuel OpazoNo ratings yet
- Sport Injuries Sustained by Athletes With Disability - A Systematic ReviewDocument13 pagesSport Injuries Sustained by Athletes With Disability - A Systematic Review2psdbwq4zbNo ratings yet
- 10.26773 smj.191005Document4 pages10.26773 smj.191005gonzalo osorioNo ratings yet
- Isquiotibiales TestDocument6 pagesIsquiotibiales TestHugo TintiNo ratings yet
- Shoulder InjuriesDocument8 pagesShoulder InjurieswernsickleNo ratings yet
- Developing A Model of Risk Factors of Injury in TRDocument11 pagesDeveloping A Model of Risk Factors of Injury in TRLuis Briones Lau.LiNo ratings yet
- Boxing Injuries Anatomical Location ReviewDocument8 pagesBoxing Injuries Anatomical Location ReviewRenaldiPrimaSaputraNo ratings yet
- Elbow Injury Guidelines for Grappling AthletesFrom EverandElbow Injury Guidelines for Grappling AthletesNo ratings yet
- Combat Time PublicadoDocument17 pagesCombat Time PublicadoMarco FerreiraNo ratings yet
- AaaaaaDocument9 pagesAaaaaaMarco FerreiraNo ratings yet
- A Review of Return To Plau Issues and Sports Related ConcussionDocument8 pagesA Review of Return To Plau Issues and Sports Related ConcussionMarco FerreiraNo ratings yet
- (18997562 - Journal of Human Kinetics) Immunological Responses To A Brazilian Jiu Jitsu High Intensity Interval Training SessionDocument10 pages(18997562 - Journal of Human Kinetics) Immunological Responses To A Brazilian Jiu Jitsu High Intensity Interval Training SessionMarco FerreiraNo ratings yet
- Potain MCT88 Top Slewing Tower Cranes Product GuideDocument6 pagesPotain MCT88 Top Slewing Tower Cranes Product GuideCompass equipmentNo ratings yet
- Cookie Crumbles Preview 1Document3 pagesCookie Crumbles Preview 1thorney33No ratings yet
- MCFC Financial ReportDocument50 pagesMCFC Financial ReportYell GeorgeNo ratings yet
- ឧបសម្ព័ន្ធស្តីពីសញ្ញាចរាចរណ៍ផ្លូវគោកDocument116 pagesឧបសម្ព័ន្ធស្តីពីសញ្ញាចរាចរណ៍ផ្លូវគោកKong SothearaNo ratings yet
- Introduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesDocument36 pagesIntroduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Taylor Timothy - Pawn Sacrifice - Winning at Chess The Adventurous Way, 2008-OCR, Everyman, 241pDocument241 pagesTaylor Timothy - Pawn Sacrifice - Winning at Chess The Adventurous Way, 2008-OCR, Everyman, 241pJamie Steiner100% (4)
- Columbine Report Pgs 3501-3600Document100 pagesColumbine Report Pgs 3501-3600columbinefamilyrequestNo ratings yet
- Michelle Sands 2 Day Smoothie ChallengeDocument7 pagesMichelle Sands 2 Day Smoothie Challengedayonara2003No ratings yet
- Italian Tennis TermsDocument2 pagesItalian Tennis TermsMiodrag UroševićNo ratings yet
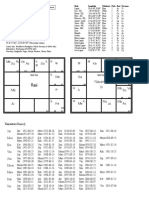
- As Ve Sa Su Me Ra Ke: NavamsaDocument1 pageAs Ve Sa Su Me Ra Ke: NavamsaAstroAnudeepNo ratings yet
- Child in Time - AcorduriDocument2 pagesChild in Time - AcorduriMădălina VinceneNo ratings yet
- Glycolysis: by Meroka A. Biochemistry DPT, KemuDocument40 pagesGlycolysis: by Meroka A. Biochemistry DPT, KemuGish KioiNo ratings yet
- Tornillos de RuedaDocument69 pagesTornillos de RuedamyaddyNo ratings yet
- Sparks 3 Worksheet 2Document20 pagesSparks 3 Worksheet 2Quil Réjane100% (4)
- MA2040: Probability, Statistics and Stochastic Processes Problem Set-IDocument6 pagesMA2040: Probability, Statistics and Stochastic Processes Problem Set-IRam Lakhan MeenaNo ratings yet
- ST1 PeDocument4 pagesST1 PeJohn Paul Paladin CuevasNo ratings yet
- Codex Imperial Guard FAQ 5th EditionDocument3 pagesCodex Imperial Guard FAQ 5th EditionJohn McLeishNo ratings yet
- Week 12 - Into FalaiseDocument3 pagesWeek 12 - Into FalaiseLord KhizirNo ratings yet
- Physics Test Review QuestionsDocument1 pagePhysics Test Review QuestionsGisele PhaloNo ratings yet
- Ten Years After - Slow Blues In' CDocument3 pagesTen Years After - Slow Blues In' CEtinho SouzaNo ratings yet
- Super Goal 4 Revision U2Document5 pagesSuper Goal 4 Revision U25plc qNo ratings yet
- City of Malolos, Bulacan: Republic of The Philippines Bulacan State University Tel/Fax (004) 791-0513Document9 pagesCity of Malolos, Bulacan: Republic of The Philippines Bulacan State University Tel/Fax (004) 791-0513KristelNavarroNo ratings yet
- CS335 Introduction To AI: Francisco Iacobelli June 25, 2015Document49 pagesCS335 Introduction To AI: Francisco Iacobelli June 25, 2015Tariq IqbalNo ratings yet
- Awakened Edition Rulebook-2024Document76 pagesAwakened Edition Rulebook-2024JoelNo ratings yet
- Cranes - Rough Terrain Crane Specifications - RT300-1 SeriesDocument4 pagesCranes - Rough Terrain Crane Specifications - RT300-1 SeriesJuan VarelaNo ratings yet
- Solutions To AIEEE: 2006-PHYSICSDocument12 pagesSolutions To AIEEE: 2006-PHYSICSAmanuel GaromsaNo ratings yet
- Anabolic Steroid ProfilesDocument135 pagesAnabolic Steroid ProfilesX-ON FITNESS100% (2)