Download as docx, pdf, or txt
You might also like
- Cleanroom Contamination Prevention & Control: A Practical Guide To The ScienceDocument13 pagesCleanroom Contamination Prevention & Control: A Practical Guide To The ScienceTim Sandle56% (9)
- Calcium Homeostasis and Osteoporosis - McMaster Pathophysiology ReviewDocument8 pagesCalcium Homeostasis and Osteoporosis - McMaster Pathophysiology ReviewEzayu AzeraNo ratings yet
- Seminar On Bone and CalciumDocument4 pagesSeminar On Bone and Calciumtshireletso “TROY” nkunaNo ratings yet
- Intro Tothe Function of Parathyroid Gland, ConciseDocument34 pagesIntro Tothe Function of Parathyroid Gland, Conciseinka.elseNo ratings yet
- New Microsoft Office Word DocumentDocument11 pagesNew Microsoft Office Word Documentrain_puvNo ratings yet
- PHD 7Document7 pagesPHD 7Elham AlwagaaNo ratings yet
- Schenck 2007Document16 pagesSchenck 2007Luisa Fernanda Rojas DiazNo ratings yet
- Agents That Affect Bone Mineral Homeostasis: Department of PharmacologyDocument44 pagesAgents That Affect Bone Mineral Homeostasis: Department of Pharmacologymichaelcyl100% (1)
- DN - AJ Metabolisme Tulang Dan SendiDocument46 pagesDN - AJ Metabolisme Tulang Dan SendiJohn Felix SitumorangNo ratings yet
- Physiology of BoneDocument22 pagesPhysiology of BoneKhairaFirselNo ratings yet
- 7 CalciumDocument83 pages7 Calciumtmqt2fbnzgNo ratings yet
- Drugs Bone DisordersDocument38 pagesDrugs Bone Disordersalizwaxabanisa8No ratings yet
- หกสหสดหวกสหาดวสดกDocument25 pagesหกสหสดหวกสหาดวสดกJames RatchanontNo ratings yet
- DR Naveed Seminar PPT 2Document60 pagesDR Naveed Seminar PPT 2mohammad abdul naveedNo ratings yet
- Lecture Notes in Medical Technology - Lecture #6 - The PARATHYROID GLANDDocument15 pagesLecture Notes in Medical Technology - Lecture #6 - The PARATHYROID GLANDKat JornadalNo ratings yet
- The Musculoskeletal SystemDocument56 pagesThe Musculoskeletal SystemMaria Dini AdmiratiNo ratings yet
- Fisiologi Molekuler TulangDocument42 pagesFisiologi Molekuler TulangKhairaFirselNo ratings yet
- Calcium and Its Significance in The Bone MetabolismDocument26 pagesCalcium and Its Significance in The Bone MetabolismVamsi MurthyNo ratings yet
- General Instructions: - The Search Should Contain The FollowingsDocument15 pagesGeneral Instructions: - The Search Should Contain The FollowingsDr-AHmad Fasfous AL-QaisiNo ratings yet
- Calcium Homeostasis: Normal Plasma LevelsDocument5 pagesCalcium Homeostasis: Normal Plasma LevelsE MeerNo ratings yet
- Bone and Mineral Metabolism in Health and DiseaseDocument14 pagesBone and Mineral Metabolism in Health and Diseasebiniam MesfinNo ratings yet
- The Calcium Regulating HormonesDocument57 pagesThe Calcium Regulating Hormonesdrsanju17No ratings yet
- 6.1 Agents That Affect Bone Mineral HomeostasisDocument17 pages6.1 Agents That Affect Bone Mineral HomeostasisAsem AlhazmiNo ratings yet
- Calcium Concentrations: MetabolismDocument6 pagesCalcium Concentrations: MetabolismSupriti Verma BhatnagarNo ratings yet
- Department of Periodontics and Implantology: Calcium MetabolismDocument63 pagesDepartment of Periodontics and Implantology: Calcium Metabolismrasagna reddy100% (1)
- Parathyroid Hormone XXXDocument5 pagesParathyroid Hormone XXXrachellouis973No ratings yet
- Kontrol Hormonal Metabolisme Kalsium - DR - Etriyel (Finish)Document30 pagesKontrol Hormonal Metabolisme Kalsium - DR - Etriyel (Finish)faris.surgeonNo ratings yet
- Calcium Homeostasis: General PhysiologyDocument6 pagesCalcium Homeostasis: General PhysiologyE MeerNo ratings yet
- Calcium HomeostasisDocument10 pagesCalcium Homeostasiszsf8m52ky4No ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- MK Biokimia - Metabolisme MineralDocument84 pagesMK Biokimia - Metabolisme MineralmusimsemiNo ratings yet
- Parathyroid: Calcium and Vitamin DDocument135 pagesParathyroid: Calcium and Vitamin DPhysiology by Dr Raghuveer100% (1)
- Formation: Blood Calcium Level - Calcium HydroxyapatiteDocument13 pagesFormation: Blood Calcium Level - Calcium HydroxyapatiteClarissa IsuriñaNo ratings yet
- Disorders of CA+ MetabolismDocument41 pagesDisorders of CA+ MetabolismSuliman GarallehNo ratings yet
- Bone Basic Science: Presenter: DR Nshimiyimana Alexis Orthopedic Resident-UrDocument36 pagesBone Basic Science: Presenter: DR Nshimiyimana Alexis Orthopedic Resident-UrNshimiyimana AlexisNo ratings yet
- Hormones of Parathyroid and Regulation of Blood Calcium LevelDocument9 pagesHormones of Parathyroid and Regulation of Blood Calcium Levelriskyy1No ratings yet
- Hormonal Control of Calcium Homeostasis Chapter 9Document8 pagesHormonal Control of Calcium Homeostasis Chapter 9Roua SafwatNo ratings yet
- Hormonal Control of Calcium and Phosphate MetabolismDocument50 pagesHormonal Control of Calcium and Phosphate MetabolismhamidNo ratings yet
- Parathyroid Hormone: Shahab Ullah Khan Ayub Medical CollegeDocument28 pagesParathyroid Hormone: Shahab Ullah Khan Ayub Medical CollegeDr KhanNo ratings yet
- Calcium Salts Calcitonin and CA RegulatorsDocument40 pagesCalcium Salts Calcitonin and CA RegulatorsSudhakar LakavathNo ratings yet
- Calcium Metabolism PraveenDocument42 pagesCalcium Metabolism PraveenDr PraveenNo ratings yet
- Lecture 8 - 15Document28 pagesLecture 8 - 15margaritaNo ratings yet
- Calcium and Phosphate Homeostasis - Endotext - NCBI BookshelfDocument32 pagesCalcium and Phosphate Homeostasis - Endotext - NCBI BookshelfdrvancedNo ratings yet
- Study Guide For Calcium and Phosphate MetabolismDocument74 pagesStudy Guide For Calcium and Phosphate MetabolismMohammad MamunuzzamanNo ratings yet
- MatthewVaracalloMD PhysiologyBoneDocument5 pagesMatthewVaracalloMD PhysiologyBonetulipaNo ratings yet
- Control Blood of Calcium LevelsDocument2 pagesControl Blood of Calcium Levelswoman in stemNo ratings yet
- CalciumDocument41 pagesCalciumIka Nindyas RanitadewiNo ratings yet
- Silva 2015Document10 pagesSilva 2015Jia-PeiWuNo ratings yet
- Bone Formation: Hypothalamic Hormone, CRH, and The Pituitary Hormone, ACTHDocument3 pagesBone Formation: Hypothalamic Hormone, CRH, and The Pituitary Hormone, ACTHSimon AvilaNo ratings yet
- MSK NotesDocument83 pagesMSK NotesabdulNo ratings yet
- Metabolisme Calsium Dan Hormon PTHDocument71 pagesMetabolisme Calsium Dan Hormon PTHzeddNo ratings yet
- Basic Science: Metabolisme Kalsium Fosfat & Vit DDocument17 pagesBasic Science: Metabolisme Kalsium Fosfat & Vit DDerly Barino HasdiNo ratings yet
- Calcium & Phospate: Kuliah Gizi MikroDocument78 pagesCalcium & Phospate: Kuliah Gizi MikroriayuniatiNo ratings yet
- Metabolic & Endocrine Bone DiseaseDocument9 pagesMetabolic & Endocrine Bone DiseaseJulian HuningkorNo ratings yet
- Biochem 38 - Bone MetabolismDocument4 pagesBiochem 38 - Bone MetabolismParker GoldsteinNo ratings yet
- Parathyroid Hormone, Calcitonin, Calcium andDocument61 pagesParathyroid Hormone, Calcitonin, Calcium andchayChay gapolNo ratings yet
- Hormonal Control of Calcium PDFDocument28 pagesHormonal Control of Calcium PDFmina hishamNo ratings yet
- Kalsifikasi, Deposisi Dan Resorpsi TulangDocument40 pagesKalsifikasi, Deposisi Dan Resorpsi TulangrifkaNo ratings yet
- ParathyroidglandsDocument32 pagesParathyroidglandsMohamed Hassan MohamudNo ratings yet
- Biochem 11Document5 pagesBiochem 11Abdullah RaufNo ratings yet
- Soft Computing Module IDocument161 pagesSoft Computing Module INatarajanSubramanyamNo ratings yet
- Piping Info - Pipe Support Design GuidelinesDocument4 pagesPiping Info - Pipe Support Design GuidelinesSUSHANTBIJAM100% (1)
- TAS Product Catalog 2020 01Document210 pagesTAS Product Catalog 2020 01ct0720054858No ratings yet
- Verb Patterns: Verb + Infinitive or Verb + - Ing?: Verbs Followed by A To-InfinitiveDocument5 pagesVerb Patterns: Verb + Infinitive or Verb + - Ing?: Verbs Followed by A To-InfinitiveTeodora PluskoskaNo ratings yet
- ASHRAE-tables Lighting Power Density PDFDocument3 pagesASHRAE-tables Lighting Power Density PDFDan MolloyNo ratings yet
- Effects of Maize-Legume Intercrops On Termite Damage To Maize, Activityof Predatoryants and Maize Yields in UgandaDocument7 pagesEffects of Maize-Legume Intercrops On Termite Damage To Maize, Activityof Predatoryants and Maize Yields in UgandasedianpoNo ratings yet
- PaintsDocument20 pagesPaintsPashmi Shah100% (1)
- Edux110 SimDocument307 pagesEdux110 SimElijahNo ratings yet
- ColaTeric BE 16Document2 pagesColaTeric BE 16mndmattNo ratings yet
- Dismantling Joints: DN350 To DN1800 (PN25)Document2 pagesDismantling Joints: DN350 To DN1800 (PN25)Boris MoreiraNo ratings yet
- Physics of Everyday Phenomena A Conceptual Introduction To Physics 8th Edition Griffith Test BankDocument14 pagesPhysics of Everyday Phenomena A Conceptual Introduction To Physics 8th Edition Griffith Test Bankdavidhallwopkseimgc100% (32)
- Narrative Text - Infografis - KurmerDocument2 pagesNarrative Text - Infografis - KurmerCitra Arba RojunaNo ratings yet
- Preguntas y Respuestas de LESSON 16Document4 pagesPreguntas y Respuestas de LESSON 16Sebastián Monroy CatrilNo ratings yet
- MODULE-4 21BE45 - PPT FinalDocument55 pagesMODULE-4 21BE45 - PPT Finalezekiel david100% (1)
- MSD Numbers 0410612020 Am: ClosingDocument11 pagesMSD Numbers 0410612020 Am: ClosingSanjeev JayaratnaNo ratings yet
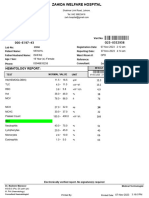
- Hematology Report:: MRN: Visit NoDocument1 pageHematology Report:: MRN: Visit Nojuniadsheikh6No ratings yet
- So-Called Logical Levels WoodsmallDocument29 pagesSo-Called Logical Levels WoodsmallDan Paris100% (2)
- Gateway To Art - 1.08Document40 pagesGateway To Art - 1.08i am bubbleNo ratings yet
- Clean and GreenDocument9 pagesClean and GreenDanny Dancel100% (1)
- What Aspects of "Life" Are Covered by Vedic AstrologyDocument4 pagesWhat Aspects of "Life" Are Covered by Vedic AstrologyMariana SantosNo ratings yet
- Healthy Lifestyle Ideas For Truck Drivers: EFS-IFR Anul I UBB Cluj 2019Document12 pagesHealthy Lifestyle Ideas For Truck Drivers: EFS-IFR Anul I UBB Cluj 2019Pap RobertNo ratings yet
- LDPDocument46 pagesLDPSoundradevi ArumugamNo ratings yet
- Drug Induced OsteoporosisDocument8 pagesDrug Induced OsteoporosislueglemeNo ratings yet
- E-SQUARE LOTO Catalogue No. 8 PDFDocument16 pagesE-SQUARE LOTO Catalogue No. 8 PDFkishoretrkNo ratings yet
- Méthodes de Dissolution FDADocument129 pagesMéthodes de Dissolution FDACH NarimaneNo ratings yet
- Renoise User ManualDocument198 pagesRenoise User Manualdrkstr77No ratings yet
- A2QVP2 TrainingDocument9 pagesA2QVP2 Trainingdanny wangNo ratings yet
- EEE40003 Digital Signal and Image Processing: LAB 3: Discrete LTI SystemsDocument13 pagesEEE40003 Digital Signal and Image Processing: LAB 3: Discrete LTI SystemsKai JieNo ratings yet
- 143 Modele CV Etats Unis ResumeDocument2 pages143 Modele CV Etats Unis ResumeGaoussou SangareNo ratings yet