Download as docx, pdf, or txt
You might also like
- RPT Maths Form 5 DLP 2022 - 2023Document16 pagesRPT Maths Form 5 DLP 2022 - 2023PETER WONG YUNG MING Moe50% (2)
- Occlusion in Complete Denture Part IIDocument48 pagesOcclusion in Complete Denture Part IIهجرسNo ratings yet
- Schuyler1953 PDFDocument11 pagesSchuyler1953 PDFMayank MalraNo ratings yet
- Balanced OcclusionDocument9 pagesBalanced OcclusionDrShweta Saini100% (1)
- Balanced Occlu HandoutDocument9 pagesBalanced Occlu HandoutMostafa FayadNo ratings yet
- Lec 6 Occluson of Complete Denture 2Document6 pagesLec 6 Occluson of Complete Denture 2pxb8dhqgs9No ratings yet
- Laws of Articulation - PPTX FinalDocument119 pagesLaws of Articulation - PPTX FinalParmod Gulia100% (1)
- علي صادق جعفرDocument6 pagesعلي صادق جعفرعلي صادق جعفرNo ratings yet
- Assignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'Document19 pagesAssignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'nivitha naidu100% (1)
- Dent 343 Lect 9 - HandoutDocument18 pagesDent 343 Lect 9 - HandoutAnas AmerNo ratings yet
- سمنار كراونDocument6 pagesسمنار كراونعلي صادق جعفرNo ratings yet
- Types of Balanced OcclusionDocument6 pagesTypes of Balanced Occlusionعلي صادق جعفرNo ratings yet
- سمنار كراونDocument6 pagesسمنار كراونعلي صادق جعفرNo ratings yet
- Principles - of - Occlusion - in - Complete - DentureDocument72 pagesPrinciples - of - Occlusion - in - Complete - DentureDaniel AtiehNo ratings yet
- Principles of Occlusion in Complete DentureDocument72 pagesPrinciples of Occlusion in Complete DentureDaniel AtiehNo ratings yet
- 1,2-Prosthodontic - Docx (1,2) Fifth ClassDocument6 pages1,2-Prosthodontic - Docx (1,2) Fifth Classjbkw2hcnfpNo ratings yet
- Balanced OcclusionDocument120 pagesBalanced Occlusionrahel sukma100% (5)
- Principles of Occlusion in Complete DentureDocument72 pagesPrinciples of Occlusion in Complete DentureMohammed NabeelNo ratings yet
- Textbook of Prosthodontics SECOND EDITIO RemovedDocument78 pagesTextbook of Prosthodontics SECOND EDITIO Removeddelfi simatupangNo ratings yet
- 01 Balanced OcclusionDocument46 pages01 Balanced OcclusionAceNo ratings yet
- Concept of OcclusionDocument81 pagesConcept of Occlusionchawalito27100% (1)
- Occlusion in Fixed ProsthodonticsDocument14 pagesOcclusion in Fixed ProsthodonticsGayathri GangadharanNo ratings yet
- Concepts of Complete Denture OcclusionDocument39 pagesConcepts of Complete Denture Occlusionaziz2007100% (1)
- Balanced Occl PDFDocument31 pagesBalanced Occl PDFggNo ratings yet
- LEC OcclusionDocument11 pagesLEC OcclusionFatimaNo ratings yet
- Occlussion in Complete Dentures ProsthoDocument59 pagesOcclussion in Complete Dentures ProsthoFourthMolar.com100% (3)
- L1&2 Occlusion ProsDocument10 pagesL1&2 Occlusion ProsMaria EvergardenNo ratings yet
- OcclusionDocument49 pagesOcclusionRajsandeep SinghNo ratings yet
- GPT 9Document37 pagesGPT 9MohamedNo ratings yet
- تقرير crownDocument3 pagesتقرير crownمحمد نعيمNo ratings yet
- Fundamentals of Occlusion: Reference: Shillingburg Funamentals of Fixed Prosthodontics, Third Edition Chapter TwoDocument44 pagesFundamentals of Occlusion: Reference: Shillingburg Funamentals of Fixed Prosthodontics, Third Edition Chapter Twoوا إسلاماه100% (2)
- Oclusion in CD ProsthoDocument62 pagesOclusion in CD ProsthoFourthMolar.com50% (2)
- Balanced Occlusion: by Reema Talat Ayesha Final Year R.R.D.CDocument31 pagesBalanced Occlusion: by Reema Talat Ayesha Final Year R.R.D.CArunNo ratings yet
- Occlusion in Complete DentureDocument35 pagesOcclusion in Complete DentureAkash Sikka100% (1)
- Occlusion in Complete DentureDocument64 pagesOcclusion in Complete Denturepuja singhNo ratings yet
- Đề Cương Khớp Cắn 2023Document23 pagesĐề Cương Khớp Cắn 2023Nguyễn Quang Trung Kiên (22100359)No ratings yet
- Occlusion / Orthodontic Courses by Indian Dental AcademyDocument90 pagesOcclusion / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- OcclusionDocument49 pagesOcclusionزياد حميد رشيدNo ratings yet
- Occlusion of Crown BridgeDocument39 pagesOcclusion of Crown BridgeRawzh Salih MuhammadNo ratings yet
- Occlusion Concepts in DentistryDocument81 pagesOcclusion Concepts in Dentistrydorasani99No ratings yet
- Complete Denture OcclusionDocument54 pagesComplete Denture OcclusionDr. Aysha Sadaf100% (2)
- Balanced Occlusion: Dr. Rakshith HegdeDocument104 pagesBalanced Occlusion: Dr. Rakshith HegdePragya Jain67% (3)
- Occlusion in Complete DentureDocument6 pagesOcclusion in Complete DentureSaif HashimNo ratings yet
- Lec8 ArangementDocument5 pagesLec8 ArangementHassan BotaniNo ratings yet
- Requirements of Complete Denture OcclusionDocument8 pagesRequirements of Complete Denture Occlusionkhaled allaNo ratings yet
- Stabilityincompletedentures 150913085317 Lva1 App6892Document31 pagesStabilityincompletedentures 150913085317 Lva1 App6892Krupali JainNo ratings yet
- Occlusion in Complete DentureDocument12 pagesOcclusion in Complete DentureNadeemNo ratings yet
- Chapter 5 OcclusionDocument14 pagesChapter 5 OcclusionYoussef ElkomatyNo ratings yet
- OcclusionDocument14 pagesOcclusionpasser byNo ratings yet
- LoDocument43 pagesLoAwani GuptaNo ratings yet
- The Function and Importance of Incisal Guidance inDocument75 pagesThe Function and Importance of Incisal Guidance inPragya Jain100% (1)
- 3 Factorsaffectingbalancedocclusionfinal 190120212520Document100 pages3 Factorsaffectingbalancedocclusionfinal 190120212520Beniamin TicaratNo ratings yet
- Anterior - GuidanceDocument21 pagesAnterior - GuidanceAayushi VaidyaNo ratings yet
- Functional Occlusion and The Mounting of The CastsDocument88 pagesFunctional Occlusion and The Mounting of The CastsAina SalsaNo ratings yet
- Optimum OccDocument50 pagesOptimum OccdrrnonhelmyNo ratings yet
- Prosthodontics May 2015Document39 pagesProsthodontics May 2015samikshaNo ratings yet
- Centric and Eccentric OcclusionsDocument8 pagesCentric and Eccentric OcclusionsYan Lau100% (1)
- 301 - 488 Ramya Raghu Clinical Operative Dentistry Principles & PracticeDocument188 pages301 - 488 Ramya Raghu Clinical Operative Dentistry Principles & PracticesamikshaNo ratings yet
- 1 - 150 Ramya Raghu Clinical Operative Dentistry Principles & PracticeDocument150 pages1 - 150 Ramya Raghu Clinical Operative Dentistry Principles & PracticesamikshaNo ratings yet
- ODMR Short NotesDocument117 pagesODMR Short NotessamikshaNo ratings yet
- Prostho Short NotesDocument84 pagesProstho Short Notessamiksha100% (1)
- ODMR Long AnsDocument119 pagesODMR Long AnssamikshaNo ratings yet
- Prosthodontics May 2015Document39 pagesProsthodontics May 2015samikshaNo ratings yet
- Cons Endo Long AnsDocument72 pagesCons Endo Long AnssamikshaNo ratings yet
- Pedo Long AnswerDocument116 pagesPedo Long AnswersamikshaNo ratings yet
- Cons Endo Short NotesDocument128 pagesCons Endo Short NotessamikshaNo ratings yet
- Review Article: Contrast Agents in Computed Tomography: A ReviewDocument7 pagesReview Article: Contrast Agents in Computed Tomography: A ReviewsamikshaNo ratings yet
- Surgery ManipalDocument35 pagesSurgery Manipalsamiksha0% (1)
- 40 Day Language PracticeDocument29 pages40 Day Language PracticeAJ AndersonNo ratings yet
- C Language Awareness: More InformationDocument1 pageC Language Awareness: More InformationLUISA CASTRO CUNEONo ratings yet
- 4 - Web Enabled Business Processes AssignmentDocument16 pages4 - Web Enabled Business Processes Assignmentrahulsanas0% (1)
- Mil Week 2Document3 pagesMil Week 2Mhagz MaggieNo ratings yet
- IP Classless Addressing: Classless Inter-Domain Routing (CIDR) / "Supernetting"Document3 pagesIP Classless Addressing: Classless Inter-Domain Routing (CIDR) / "Supernetting"SHOBHA VERMANo ratings yet
- Allison Serie 9800Document2 pagesAllison Serie 9800Anonymous TEbcqw5RbT100% (2)
- Progressive Design Update 10.10.22Document9 pagesProgressive Design Update 10.10.22Vikas PaiNo ratings yet
- Low-Cost Multimodal Physiological Telemonitoring System Through Internet of ThingsDocument9 pagesLow-Cost Multimodal Physiological Telemonitoring System Through Internet of Thingsfaizal amriNo ratings yet
- The Plant Journal - 2023 - Selma Garc A - Engineering The Plant Metabolic System by Exploiting Metabolic RegulationDocument28 pagesThe Plant Journal - 2023 - Selma Garc A - Engineering The Plant Metabolic System by Exploiting Metabolic RegulationRodrigo ParolaNo ratings yet
- MMC Questions For Division Finals Grade 5 - 2Document2 pagesMMC Questions For Division Finals Grade 5 - 2Rocelia Abelardo100% (1)
- Night Vision Technology: Seminars Electronics & Communication EngineeringDocument2 pagesNight Vision Technology: Seminars Electronics & Communication Engineeringphani98No ratings yet
- Athena: Microsoft ® Encarta ® Encyclopedia 2002. © 1993-2001 Microsoft Corporation. All RightsDocument1 pageAthena: Microsoft ® Encarta ® Encyclopedia 2002. © 1993-2001 Microsoft Corporation. All RightsAnonymous ck0aGAqZlNo ratings yet
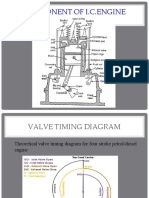
- Valve Timing DiagramDocument43 pagesValve Timing Diagramѕυdeѕн ĸNo ratings yet
- Chapter OneDocument5 pagesChapter OneJosam Montero FordNo ratings yet
- Lab Report Et 2Document19 pagesLab Report Et 2Peach BabyNo ratings yet
- Issues Surrounding Reliability and Validity-1Document38 pagesIssues Surrounding Reliability and Validity-1kylieverNo ratings yet
- Study ThisDocument83 pagesStudy Thispavithiran subramaniNo ratings yet
- The Yoga Sutras of Patanjali PDFDocument168 pagesThe Yoga Sutras of Patanjali PDFjhonprestonNo ratings yet
- EPC Saur Energy InternationalDocument3 pagesEPC Saur Energy InternationalNarendra PatelNo ratings yet
- Chemical Process Principles (CLB10904) : Chapter 2 Material Balance: (Part 3) : CombustionDocument18 pagesChemical Process Principles (CLB10904) : Chapter 2 Material Balance: (Part 3) : CombustionFATMIENo ratings yet
- IELTS Writing Task1 TableDocument16 pagesIELTS Writing Task1 TableRakesh Kumar Sharma100% (1)
- Problem 1Document8 pagesProblem 1KyleRhayneDiazCaliwagNo ratings yet
- Prince Ea-I Just Sued The School SystemDocument3 pagesPrince Ea-I Just Sued The School SystemTizioNo ratings yet
- Audit in A CIS Environment 4Document2 pagesAudit in A CIS Environment 4Shyrine EjemNo ratings yet
- No. in Sq. Ft. Sq. Yds. MarlasDocument7 pagesNo. in Sq. Ft. Sq. Yds. MarlasYasir ButtNo ratings yet
- Rand Oh Di So 22324668100220Document2 pagesRand Oh Di So 22324668100220Crystal RojasNo ratings yet
- Today1 AchievementTestUnits3 4extensionDocument2 pagesToday1 AchievementTestUnits3 4extensionEmii GarcíaNo ratings yet
- Bye Pass Rotameter: Eureka Industrial Equipments Pvt. LTDDocument2 pagesBye Pass Rotameter: Eureka Industrial Equipments Pvt. LTDArunasis KarmakarNo ratings yet
- Niagara Region Integrity Commissioner Report On West Lincoln Mayor David BylsmaDocument19 pagesNiagara Region Integrity Commissioner Report On West Lincoln Mayor David BylsmaGrant LaFlecheNo ratings yet