
(13C) The Role of Dental Calculus and Other Local Predisposing Factors
(13C) The Role of Dental Calculus and Other Local Predisposing Factors
You might also like
- Giovanni Zucchelli - Mucogingival Esthetic Surgery-Quintessence Pub Co (2013)Document832 pagesGiovanni Zucchelli - Mucogingival Esthetic Surgery-Quintessence Pub Co (2013)Negrus Stefan100% (1)
- Pocketbook of Oral Diseases PDFDocument453 pagesPocketbook of Oral Diseases PDFAkash Anilkumar Malini100% (1)
- Case History, Diagnosis and Treatment Planning For Removable Partial DenturesDocument149 pagesCase History, Diagnosis and Treatment Planning For Removable Partial DenturesShilpi Sanghvi100% (5)
- White1997 Dental Calculus Formation EtcDocument16 pagesWhite1997 Dental Calculus Formation EtcJose Salas AdragnaNo ratings yet
- Biological Guides To The Positioning of The Artificial Teeth in Complete DenturesDocument4 pagesBiological Guides To The Positioning of The Artificial Teeth in Complete DenturesDan Beznoiu100% (3)
- Bethany Pinnock - Perio IV Final PaperDocument4 pagesBethany Pinnock - Perio IV Final PaperBethany PinnockNo ratings yet
- Etiology of Periodontal Diseases: Dental Plaque (Microorganisms)Document9 pagesEtiology of Periodontal Diseases: Dental Plaque (Microorganisms)محمد محمود القحيفNo ratings yet
- Management of Deep Carious LesionDocument14 pagesManagement of Deep Carious Lesionahmedstar162000No ratings yet
- Endo Perio LesionsDocument10 pagesEndo Perio LesionsAlin OdorNo ratings yet
- Bun InTech-Orthodontics and CariesDocument19 pagesBun InTech-Orthodontics and CariescareNo ratings yet
- Management of Internal Root Resorption A ReviewDocument8 pagesManagement of Internal Root Resorption A ReviewDana StanciuNo ratings yet
- Davis 2014Document11 pagesDavis 2014Monica JohanaNo ratings yet
- Dental Caries DevelopmentDocument8 pagesDental Caries Developmentريام الموسويNo ratings yet
- 32 V PDFDocument7 pages32 V PDFNabil AlkaffNo ratings yet
- Nibali Development of The Gingival Sulcus 2017 AcceptedDocument14 pagesNibali Development of The Gingival Sulcus 2017 AcceptedLily BrostNo ratings yet
- Periodontics I/Lecture3 Etiology of Periodontal Diseases: Dental PlaqueDocument12 pagesPeriodontics I/Lecture3 Etiology of Periodontal Diseases: Dental Plaqueربيد احمد مثنى يحيى كلية طب الاسنان - جامعة عدنNo ratings yet
- The Aetiology of Gingival RecessionDocument4 pagesThe Aetiology of Gingival RecessionshahidibrarNo ratings yet
- Cap 22Document15 pagesCap 22Maria Fernanda Gallon SotoNo ratings yet
- Dental Caries A ReviewDocument7 pagesDental Caries A ReviewAndrei PaşaniucNo ratings yet
- Tissue Response To Dental CariesDocument24 pagesTissue Response To Dental CariesGabriel Miloiu100% (1)
- Discussion 3Document33 pagesDiscussion 3navyaharitha nandinaNo ratings yet
- Preven Lec 2Document7 pagesPreven Lec 2ريام الموسويNo ratings yet
- CHAP 10 Dental Calculus SelfDocument38 pagesCHAP 10 Dental Calculus SelfarshmeentariqNo ratings yet
- Dental Radiology LectureDocument40 pagesDental Radiology LectureAbdullahayad farouqNo ratings yet
- Dental HygieneDocument8 pagesDental HygieneNurul HanifahNo ratings yet
- Endo-Perio Lesions Diagnosis and Clinical ConsiderationsDocument8 pagesEndo-Perio Lesions Diagnosis and Clinical ConsiderationsBejan OvidiuNo ratings yet
- Gingiva and Orthodontic Treatment PDFDocument15 pagesGingiva and Orthodontic Treatment PDFmutansNo ratings yet
- Eb 79Document5 pagesEb 79mohammad naufalNo ratings yet
- Endodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda SahaDocument6 pagesEndodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda Sahanovia chantikaNo ratings yet
- Gingival Recession and Root Coverage Up To Date A Liter 2022 Dentistry RevDocument10 pagesGingival Recession and Root Coverage Up To Date A Liter 2022 Dentistry RevDavid ABCNo ratings yet
- Prevention of Dental CariesDocument6 pagesPrevention of Dental CariesRadhwan Hameed AsadNo ratings yet
- Pubmed 9395117Document3 pagesPubmed 9395117Nabilaa PutriNo ratings yet
- Dental Caries MSCDocument137 pagesDental Caries MSCNahla OthmanNo ratings yet
- 7 L0910 - ENG - 4year - VIIISemester - VNicolaiciucDocument16 pages7 L0910 - ENG - 4year - VIIISemester - VNicolaiciucShany SchwarzwaldNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Pulp Therapy in Maxillary Fused Primary Central and Lateral Incisor: A Case ReportDocument6 pagesPulp Therapy in Maxillary Fused Primary Central and Lateral Incisor: A Case ReportAsriNo ratings yet
- Case Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisDocument5 pagesCase Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisSarah Ariefah SantriNo ratings yet
- Dental CalculusDocument70 pagesDental CalculusDUKUZIMANA CONCORDENo ratings yet
- Dental CalculusDocument10 pagesDental Calculusاحمد سلامNo ratings yet
- Perio RestorativeDocument5 pagesPerio RestorativeErdeli StefaniaNo ratings yet
- Extreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical ManagementDocument8 pagesExtreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical Managementcarmen espinozaNo ratings yet
- Gingival Recession and Various Root Coverage ProceduresDocument6 pagesGingival Recession and Various Root Coverage ProceduresKhalid G. AzouniNo ratings yet
- Endo Perio RelationsDocument28 pagesEndo Perio RelationsMunish BatraNo ratings yet
- 2005 Gulavibala - Effects of Mechanical and Chemical Procedures On Root Canal SurfacesDocument20 pages2005 Gulavibala - Effects of Mechanical and Chemical Procedures On Root Canal SurfacesCarlos San MartinNo ratings yet
- 24-Sequelae of Wearing Complete Dentures - Rajat DangDocument19 pages24-Sequelae of Wearing Complete Dentures - Rajat DangNaunit Vaid100% (1)
- Course 7Document6 pagesCourse 7Tal ShvetsNo ratings yet
- Perio AssiDocument9 pagesPerio AssiKarim Mohamed Fayez Farahat MahmoudNo ratings yet
- Pulp Dentin BiologyDocument21 pagesPulp Dentin BiologyCristiane VazNo ratings yet
- Mucogingival Conditions in The Natural DentitionDocument9 pagesMucogingival Conditions in The Natural Dentitionclaudyedith197527No ratings yet
- Current Concepts in The Management of Periodontitis: Concise Clinical ReviewDocument15 pagesCurrent Concepts in The Management of Periodontitis: Concise Clinical ReviewAlexandru Codrin-IonutNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- The Development of Dental CariesDocument6 pagesThe Development of Dental CariesHaider F YehyaNo ratings yet
- Periodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental AcademyDocument81 pagesPeriodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Periodontology 2000 - 2003 - DeSANCTIS - The Role of Resective Periodontal Surgery in The Treatment of Furcation DefectsDocument15 pagesPeriodontology 2000 - 2003 - DeSANCTIS - The Role of Resective Periodontal Surgery in The Treatment of Furcation Defectscarla lopezNo ratings yet
- Dental PlaqueDocument9 pagesDental PlaqueDrAbhishek SinhaNo ratings yet
- Dentistry 10 00150Document10 pagesDentistry 10 00150Sam RasydNo ratings yet
- Alternative - Interventions To FormocrescolDocument9 pagesAlternative - Interventions To FormocrescolAsh PeiNo ratings yet
- Cariology I and II Text NotesDocument10 pagesCariology I and II Text NotesdudeNo ratings yet
- Pulp and InjuryDocument13 pagesPulp and InjuryAfin Aslihatul UmmahNo ratings yet
- The Structure of Dental Plaque - Listgarten (1994)Document14 pagesThe Structure of Dental Plaque - Listgarten (1994)madiesNo ratings yet
- Wjarr 2023 0689Document10 pagesWjarr 2023 0689Naliana LupascuNo ratings yet
- Prevention PeriodontalDocument12 pagesPrevention PeriodontalmuhammadNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- (6P) Basic Concepts in Immunity and InflammationDocument6 pages(6P) Basic Concepts in Immunity and InflammationNegrus Stefan100% (1)
- (6C) Fundamentals in EpidemiologyDocument7 pages(6C) Fundamentals in EpidemiologyNegrus StefanNo ratings yet
- (8C) Periodontal MicrobiologyDocument9 pages(8C) Periodontal MicrobiologyNegrus StefanNo ratings yet
- (7P) Host-Microbial Interactions in Periodontal DiseasesDocument6 pages(7P) Host-Microbial Interactions in Periodontal DiseasesNegrus StefanNo ratings yet
- A Fixed-Removable Type of Telescopic Prosthesis: A Clinical-ReportDocument4 pagesA Fixed-Removable Type of Telescopic Prosthesis: A Clinical-ReportNegrus StefanNo ratings yet
- LP 3 - Cephalometric TWEED AnalysisDocument47 pagesLP 3 - Cephalometric TWEED AnalysisNegrus StefanNo ratings yet
- The Marginal Fit of Lithium Disilicate Crowns: Press vs. CAD/CAMDocument7 pagesThe Marginal Fit of Lithium Disilicate Crowns: Press vs. CAD/CAMNegrus StefanNo ratings yet
- Flap SurgeryDocument38 pagesFlap SurgeryChauhan Naresh100% (1)
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- 21 Principles of Smile DesignDocument44 pages21 Principles of Smile DesignOT100% (2)
- Periodontium (2) - Gingiva: Microscopic Features of GingivaDocument8 pagesPeriodontium (2) - Gingiva: Microscopic Features of Gingivaمحمد محمود القحيفNo ratings yet
- March Rqs COMPILED BY DR. STRANGEDocument89 pagesMarch Rqs COMPILED BY DR. STRANGEghassan100% (1)
- Gingivitis Experimental LoeDocument11 pagesGingivitis Experimental LoeCarla Itzel C SánchezNo ratings yet
- Locally Administered Probiotic, RCT-articleDocument7 pagesLocally Administered Probiotic, RCT-articleDebjyoti DebnathNo ratings yet
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiNo ratings yet
- Harmony of Smile Design in The Facial Context: Clinical ResearchDocument16 pagesHarmony of Smile Design in The Facial Context: Clinical ResearchAarónNo ratings yet
- Resective Osseous SurgeryDocument57 pagesResective Osseous SurgeryМихаил Танев100% (1)
- ProsthoDocument59 pagesProsthoramNo ratings yet
- Gingivitis Vs PeriodontitisDocument2 pagesGingivitis Vs Periodontitisandreas kevinNo ratings yet
- Retrocuspid Papilla Presenting As A Giant Cell F - 2022 - Journal of Dental ScieDocument2 pagesRetrocuspid Papilla Presenting As A Giant Cell F - 2022 - Journal of Dental ScieDavid ABCNo ratings yet
- The Eight Components of A Balanced SmileDocument13 pagesThe Eight Components of A Balanced SmileMeshari Al- NafisiNo ratings yet
- Late-Stage Care: Providing Care and Comfort During The Late Stage of Alzheimer'S DiseaseDocument12 pagesLate-Stage Care: Providing Care and Comfort During The Late Stage of Alzheimer'S DiseaseマガラノチャールNo ratings yet
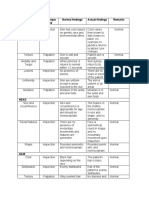
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosNo ratings yet
- 1 Fluid ControlDocument27 pages1 Fluid ControlVikas Aggarwal100% (1)
- Diagnosis and Treatment Plan in FPD - PPTX NewDocument99 pagesDiagnosis and Treatment Plan in FPD - PPTX Newreshma shaikNo ratings yet
- Os ProposalDocument20 pagesOs ProposalBipin SunarNo ratings yet
- Perio PrelimsDocument12 pagesPerio PrelimsathenaNo ratings yet
- Plaque IndexDocument2 pagesPlaque Indexkarthik33% (3)
- Diseases and Their Suitable Gem RemedyDocument14 pagesDiseases and Their Suitable Gem RemedyRajesh DeziNo ratings yet
- Analysis of The Socket Bone Wall Dimensions in The Upper Maxilla in Relation To Immediate Implant PlacementDocument6 pagesAnalysis of The Socket Bone Wall Dimensions in The Upper Maxilla in Relation To Immediate Implant PlacementLeonardo PolitoNo ratings yet
- The Connective Tissue Platform Technique For Soft Tissue AugmentationDocument13 pagesThe Connective Tissue Platform Technique For Soft Tissue Augmentation李潮忠No ratings yet
- AIPG 2006 (Dental)Document14 pagesAIPG 2006 (Dental)DENTALORG.COM0% (1)
- Manual Ortoimplantes PDFDocument22 pagesManual Ortoimplantes PDFSantos LopNo ratings yet
- Guideline For Veneer PrepDocument8 pagesGuideline For Veneer Prepnobelcyril100% (1)
































































































Download as docx, pdf, or txt
You might also like
- Giovanni Zucchelli - Mucogingival Esthetic Surgery-Quintessence Pub Co (2013)Document832 pagesGiovanni Zucchelli - Mucogingival Esthetic Surgery-Quintessence Pub Co (2013)Negrus Stefan100% (1)
- Pocketbook of Oral Diseases PDFDocument453 pagesPocketbook of Oral Diseases PDFAkash Anilkumar Malini100% (1)
- Case History, Diagnosis and Treatment Planning For Removable Partial DenturesDocument149 pagesCase History, Diagnosis and Treatment Planning For Removable Partial DenturesShilpi Sanghvi100% (5)
- White1997 Dental Calculus Formation EtcDocument16 pagesWhite1997 Dental Calculus Formation EtcJose Salas AdragnaNo ratings yet
- Biological Guides To The Positioning of The Artificial Teeth in Complete DenturesDocument4 pagesBiological Guides To The Positioning of The Artificial Teeth in Complete DenturesDan Beznoiu100% (3)
- Bethany Pinnock - Perio IV Final PaperDocument4 pagesBethany Pinnock - Perio IV Final PaperBethany PinnockNo ratings yet
- Etiology of Periodontal Diseases: Dental Plaque (Microorganisms)Document9 pagesEtiology of Periodontal Diseases: Dental Plaque (Microorganisms)محمد محمود القحيفNo ratings yet
- Management of Deep Carious LesionDocument14 pagesManagement of Deep Carious Lesionahmedstar162000No ratings yet
- Endo Perio LesionsDocument10 pagesEndo Perio LesionsAlin OdorNo ratings yet
- Bun InTech-Orthodontics and CariesDocument19 pagesBun InTech-Orthodontics and CariescareNo ratings yet
- Management of Internal Root Resorption A ReviewDocument8 pagesManagement of Internal Root Resorption A ReviewDana StanciuNo ratings yet
- Davis 2014Document11 pagesDavis 2014Monica JohanaNo ratings yet
- Dental Caries DevelopmentDocument8 pagesDental Caries Developmentريام الموسويNo ratings yet
- 32 V PDFDocument7 pages32 V PDFNabil AlkaffNo ratings yet
- Nibali Development of The Gingival Sulcus 2017 AcceptedDocument14 pagesNibali Development of The Gingival Sulcus 2017 AcceptedLily BrostNo ratings yet
- Periodontics I/Lecture3 Etiology of Periodontal Diseases: Dental PlaqueDocument12 pagesPeriodontics I/Lecture3 Etiology of Periodontal Diseases: Dental Plaqueربيد احمد مثنى يحيى كلية طب الاسنان - جامعة عدنNo ratings yet
- The Aetiology of Gingival RecessionDocument4 pagesThe Aetiology of Gingival RecessionshahidibrarNo ratings yet
- Cap 22Document15 pagesCap 22Maria Fernanda Gallon SotoNo ratings yet
- Dental Caries A ReviewDocument7 pagesDental Caries A ReviewAndrei PaşaniucNo ratings yet
- Tissue Response To Dental CariesDocument24 pagesTissue Response To Dental CariesGabriel Miloiu100% (1)
- Discussion 3Document33 pagesDiscussion 3navyaharitha nandinaNo ratings yet
- Preven Lec 2Document7 pagesPreven Lec 2ريام الموسويNo ratings yet
- CHAP 10 Dental Calculus SelfDocument38 pagesCHAP 10 Dental Calculus SelfarshmeentariqNo ratings yet
- Dental Radiology LectureDocument40 pagesDental Radiology LectureAbdullahayad farouqNo ratings yet
- Dental HygieneDocument8 pagesDental HygieneNurul HanifahNo ratings yet
- Endo-Perio Lesions Diagnosis and Clinical ConsiderationsDocument8 pagesEndo-Perio Lesions Diagnosis and Clinical ConsiderationsBejan OvidiuNo ratings yet
- Gingiva and Orthodontic Treatment PDFDocument15 pagesGingiva and Orthodontic Treatment PDFmutansNo ratings yet
- Eb 79Document5 pagesEb 79mohammad naufalNo ratings yet
- Endodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda SahaDocument6 pagesEndodontic-Periodontal Lesion: A Two-Way Traffic: Dr. Anindya Priya Saha, Dr. Anindya Chakraborty and Dr. Sananda Sahanovia chantikaNo ratings yet
- Gingival Recession and Root Coverage Up To Date A Liter 2022 Dentistry RevDocument10 pagesGingival Recession and Root Coverage Up To Date A Liter 2022 Dentistry RevDavid ABCNo ratings yet
- Prevention of Dental CariesDocument6 pagesPrevention of Dental CariesRadhwan Hameed AsadNo ratings yet
- Pubmed 9395117Document3 pagesPubmed 9395117Nabilaa PutriNo ratings yet
- Dental Caries MSCDocument137 pagesDental Caries MSCNahla OthmanNo ratings yet
- 7 L0910 - ENG - 4year - VIIISemester - VNicolaiciucDocument16 pages7 L0910 - ENG - 4year - VIIISemester - VNicolaiciucShany SchwarzwaldNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Pulp Therapy in Maxillary Fused Primary Central and Lateral Incisor: A Case ReportDocument6 pagesPulp Therapy in Maxillary Fused Primary Central and Lateral Incisor: A Case ReportAsriNo ratings yet
- Case Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisDocument5 pagesCase Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisSarah Ariefah SantriNo ratings yet
- Dental CalculusDocument70 pagesDental CalculusDUKUZIMANA CONCORDENo ratings yet
- Dental CalculusDocument10 pagesDental Calculusاحمد سلامNo ratings yet
- Perio RestorativeDocument5 pagesPerio RestorativeErdeli StefaniaNo ratings yet
- Extreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical ManagementDocument8 pagesExtreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical Managementcarmen espinozaNo ratings yet
- Gingival Recession and Various Root Coverage ProceduresDocument6 pagesGingival Recession and Various Root Coverage ProceduresKhalid G. AzouniNo ratings yet
- Endo Perio RelationsDocument28 pagesEndo Perio RelationsMunish BatraNo ratings yet
- 2005 Gulavibala - Effects of Mechanical and Chemical Procedures On Root Canal SurfacesDocument20 pages2005 Gulavibala - Effects of Mechanical and Chemical Procedures On Root Canal SurfacesCarlos San MartinNo ratings yet
- 24-Sequelae of Wearing Complete Dentures - Rajat DangDocument19 pages24-Sequelae of Wearing Complete Dentures - Rajat DangNaunit Vaid100% (1)
- Course 7Document6 pagesCourse 7Tal ShvetsNo ratings yet
- Perio AssiDocument9 pagesPerio AssiKarim Mohamed Fayez Farahat MahmoudNo ratings yet
- Pulp Dentin BiologyDocument21 pagesPulp Dentin BiologyCristiane VazNo ratings yet
- Mucogingival Conditions in The Natural DentitionDocument9 pagesMucogingival Conditions in The Natural Dentitionclaudyedith197527No ratings yet
- Current Concepts in The Management of Periodontitis: Concise Clinical ReviewDocument15 pagesCurrent Concepts in The Management of Periodontitis: Concise Clinical ReviewAlexandru Codrin-IonutNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- The Development of Dental CariesDocument6 pagesThe Development of Dental CariesHaider F YehyaNo ratings yet
- Periodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental AcademyDocument81 pagesPeriodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Periodontology 2000 - 2003 - DeSANCTIS - The Role of Resective Periodontal Surgery in The Treatment of Furcation DefectsDocument15 pagesPeriodontology 2000 - 2003 - DeSANCTIS - The Role of Resective Periodontal Surgery in The Treatment of Furcation Defectscarla lopezNo ratings yet
- Dental PlaqueDocument9 pagesDental PlaqueDrAbhishek SinhaNo ratings yet
- Dentistry 10 00150Document10 pagesDentistry 10 00150Sam RasydNo ratings yet
- Alternative - Interventions To FormocrescolDocument9 pagesAlternative - Interventions To FormocrescolAsh PeiNo ratings yet
- Cariology I and II Text NotesDocument10 pagesCariology I and II Text NotesdudeNo ratings yet
- Pulp and InjuryDocument13 pagesPulp and InjuryAfin Aslihatul UmmahNo ratings yet
- The Structure of Dental Plaque - Listgarten (1994)Document14 pagesThe Structure of Dental Plaque - Listgarten (1994)madiesNo ratings yet
- Wjarr 2023 0689Document10 pagesWjarr 2023 0689Naliana LupascuNo ratings yet
- Prevention PeriodontalDocument12 pagesPrevention PeriodontalmuhammadNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- (6P) Basic Concepts in Immunity and InflammationDocument6 pages(6P) Basic Concepts in Immunity and InflammationNegrus Stefan100% (1)
- (6C) Fundamentals in EpidemiologyDocument7 pages(6C) Fundamentals in EpidemiologyNegrus StefanNo ratings yet
- (8C) Periodontal MicrobiologyDocument9 pages(8C) Periodontal MicrobiologyNegrus StefanNo ratings yet
- (7P) Host-Microbial Interactions in Periodontal DiseasesDocument6 pages(7P) Host-Microbial Interactions in Periodontal DiseasesNegrus StefanNo ratings yet
- A Fixed-Removable Type of Telescopic Prosthesis: A Clinical-ReportDocument4 pagesA Fixed-Removable Type of Telescopic Prosthesis: A Clinical-ReportNegrus StefanNo ratings yet
- LP 3 - Cephalometric TWEED AnalysisDocument47 pagesLP 3 - Cephalometric TWEED AnalysisNegrus StefanNo ratings yet
- The Marginal Fit of Lithium Disilicate Crowns: Press vs. CAD/CAMDocument7 pagesThe Marginal Fit of Lithium Disilicate Crowns: Press vs. CAD/CAMNegrus StefanNo ratings yet
- Flap SurgeryDocument38 pagesFlap SurgeryChauhan Naresh100% (1)
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- 21 Principles of Smile DesignDocument44 pages21 Principles of Smile DesignOT100% (2)
- Periodontium (2) - Gingiva: Microscopic Features of GingivaDocument8 pagesPeriodontium (2) - Gingiva: Microscopic Features of Gingivaمحمد محمود القحيفNo ratings yet
- March Rqs COMPILED BY DR. STRANGEDocument89 pagesMarch Rqs COMPILED BY DR. STRANGEghassan100% (1)
- Gingivitis Experimental LoeDocument11 pagesGingivitis Experimental LoeCarla Itzel C SánchezNo ratings yet
- Locally Administered Probiotic, RCT-articleDocument7 pagesLocally Administered Probiotic, RCT-articleDebjyoti DebnathNo ratings yet
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiNo ratings yet
- Harmony of Smile Design in The Facial Context: Clinical ResearchDocument16 pagesHarmony of Smile Design in The Facial Context: Clinical ResearchAarónNo ratings yet
- Resective Osseous SurgeryDocument57 pagesResective Osseous SurgeryМихаил Танев100% (1)
- ProsthoDocument59 pagesProsthoramNo ratings yet
- Gingivitis Vs PeriodontitisDocument2 pagesGingivitis Vs Periodontitisandreas kevinNo ratings yet
- Retrocuspid Papilla Presenting As A Giant Cell F - 2022 - Journal of Dental ScieDocument2 pagesRetrocuspid Papilla Presenting As A Giant Cell F - 2022 - Journal of Dental ScieDavid ABCNo ratings yet
- The Eight Components of A Balanced SmileDocument13 pagesThe Eight Components of A Balanced SmileMeshari Al- NafisiNo ratings yet
- Late-Stage Care: Providing Care and Comfort During The Late Stage of Alzheimer'S DiseaseDocument12 pagesLate-Stage Care: Providing Care and Comfort During The Late Stage of Alzheimer'S DiseaseマガラノチャールNo ratings yet
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosNo ratings yet
- 1 Fluid ControlDocument27 pages1 Fluid ControlVikas Aggarwal100% (1)
- Diagnosis and Treatment Plan in FPD - PPTX NewDocument99 pagesDiagnosis and Treatment Plan in FPD - PPTX Newreshma shaikNo ratings yet
- Os ProposalDocument20 pagesOs ProposalBipin SunarNo ratings yet
- Perio PrelimsDocument12 pagesPerio PrelimsathenaNo ratings yet
- Plaque IndexDocument2 pagesPlaque Indexkarthik33% (3)
- Diseases and Their Suitable Gem RemedyDocument14 pagesDiseases and Their Suitable Gem RemedyRajesh DeziNo ratings yet
- Analysis of The Socket Bone Wall Dimensions in The Upper Maxilla in Relation To Immediate Implant PlacementDocument6 pagesAnalysis of The Socket Bone Wall Dimensions in The Upper Maxilla in Relation To Immediate Implant PlacementLeonardo PolitoNo ratings yet
- The Connective Tissue Platform Technique For Soft Tissue AugmentationDocument13 pagesThe Connective Tissue Platform Technique For Soft Tissue Augmentation李潮忠No ratings yet
- AIPG 2006 (Dental)Document14 pagesAIPG 2006 (Dental)DENTALORG.COM0% (1)
- Manual Ortoimplantes PDFDocument22 pagesManual Ortoimplantes PDFSantos LopNo ratings yet
- Guideline For Veneer PrepDocument8 pagesGuideline For Veneer Prepnobelcyril100% (1)