Download as pdf or txt
You might also like
- Abnormal Psychology 17th Edition Butcher Test Bank Full Chapter PDFDocument67 pagesAbnormal Psychology 17th Edition Butcher Test Bank Full Chapter PDFDouglasRubiopger100% (17)
- IbogaineDocument11 pagesIbogaineAkanksha SinghNo ratings yet
- Update On The Use of Cyclooxygenase-2-Selective Nonsteroidal Anti-Inflammatory Drugs in Horses Review ArticleDocument4 pagesUpdate On The Use of Cyclooxygenase-2-Selective Nonsteroidal Anti-Inflammatory Drugs in Horses Review ArticleSusanaNo ratings yet
- Walker 2017Document18 pagesWalker 2017ericdgNo ratings yet
- Review Article: Alleviating Promotion of Inflammation and Cancer Induced by Nonsteroidal Anti-Inflammatory DrugsDocument18 pagesReview Article: Alleviating Promotion of Inflammation and Cancer Induced by Nonsteroidal Anti-Inflammatory DrugsNadiaa MJNo ratings yet
- Batlouni Introduação PDFDocument8 pagesBatlouni Introduação PDFEryclisNunesNo ratings yet
- Use of NSAIDS in Treating Patients With ArthritisDocument10 pagesUse of NSAIDS in Treating Patients With ArthritisajengmdNo ratings yet
- HNPDocument10 pagesHNPPattia1980No ratings yet
- COX-2 Inhibitors and Cardiovascular RiskDocument3 pagesCOX-2 Inhibitors and Cardiovascular RiskelhierofanteNo ratings yet
- BMRC Rainsford Ibuprofen09Review PDFDocument68 pagesBMRC Rainsford Ibuprofen09Review PDFAsma nurNo ratings yet
- The Cardiovascular Pharmacology of COX-2 Inhibition: Susanne Fries and Tilo GrosserDocument7 pagesThe Cardiovascular Pharmacology of COX-2 Inhibition: Susanne Fries and Tilo GrosserFernandiita de LopezNo ratings yet
- Update On The Clinical Pharmacology of Etoricoxib A Potent Cyclooxygenase2 InhibitorDocument21 pagesUpdate On The Clinical Pharmacology of Etoricoxib A Potent Cyclooxygenase2 InhibitorAnh Quoc LeNo ratings yet
- Clinical Pharmacology of Non Steroidal A20151118 17879 2qewjq WithDocument14 pagesClinical Pharmacology of Non Steroidal A20151118 17879 2qewjq WithAli KareemNo ratings yet
- Pharmacology of MeloxicamDocument9 pagesPharmacology of MeloxicamkwadwobrosNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs in Animals - Pharmacology - MSD Veterinary ManualDocument12 pagesNonsteroidal Anti-Inflammatory Drugs in Animals - Pharmacology - MSD Veterinary ManualFairuz Nanda MarhabanazNo ratings yet
- KetorolacDocument8 pagesKetorolacwalit1101 mukrininNo ratings yet
- NsaidDocument51 pagesNsaidRaj KumarNo ratings yet
- Coxibs and Heart Disease: What We Have Learned and What Else We Need To KnowDocument14 pagesCoxibs and Heart Disease: What We Have Learned and What Else We Need To KnowYariCárdenasNo ratings yet
- Cyclooxygenase-2 in Cardiovascular Biology: BackgroundDocument6 pagesCyclooxygenase-2 in Cardiovascular Biology: BackgroundDiego PicchioNo ratings yet
- Selective COX-2 Inhibitors: A Review of Their Structure-Activity RelationshipsDocument30 pagesSelective COX-2 Inhibitors: A Review of Their Structure-Activity RelationshipsMona SalihNo ratings yet
- Analgesicos No Opiodes No Esteroideos y Cox SelectivosDocument14 pagesAnalgesicos No Opiodes No Esteroideos y Cox SelectivosXY PragmaNo ratings yet
- Different Mechanisms in Formation and Prevention of Indomethacin-Induced Gastric UlcersDocument12 pagesDifferent Mechanisms in Formation and Prevention of Indomethacin-Induced Gastric UlcersEsti Suryani Haro MuntheNo ratings yet
- Cox 2 DocumentDocument29 pagesCox 2 DocumentLanggeng Perdhana Jangan MenyerahNo ratings yet
- Cox 2 InhibitorsDocument9 pagesCox 2 InhibitorsirlandagarandaNo ratings yet
- Aines HorseDocument15 pagesAines HorseOscar Ivan AngaritaNo ratings yet
- A15 DifferentMechanismsinFormationDocument11 pagesA15 DifferentMechanismsinFormationshabbirNo ratings yet
- Renal Effects of NSAIDDocument8 pagesRenal Effects of NSAIDtaner_soysurenNo ratings yet
- NSAIDSDocument12 pagesNSAIDSNikita ShokurNo ratings yet
- Using N, N, N',N'-tetramethyl-p-phenylenediamine (TMPD) To Assay Cyclooxygenase Activity in VitroDocument13 pagesUsing N, N, N',N'-tetramethyl-p-phenylenediamine (TMPD) To Assay Cyclooxygenase Activity in VitroTatianaAlejandraCárdenasSolanoNo ratings yet
- Evolution of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) Cyclooxygenase (COX) Inhibition and BeyondDocument31 pagesEvolution of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) Cyclooxygenase (COX) Inhibition and BeyondAlexandru SavaNo ratings yet
- Selective Cox-2 Inhibitor: Visha.M.GDocument6 pagesSelective Cox-2 Inhibitor: Visha.M.GinventionjournalsNo ratings yet
- Piroxicam Article: Journal of Pharmacy Research April 2018Document7 pagesPiroxicam Article: Journal of Pharmacy Research April 2018Ulfah RahmanNo ratings yet
- NSAIDsDocument45 pagesNSAIDsAnamta AshfaqNo ratings yet
- Piroxicamarticle PDFDocument7 pagesPiroxicamarticle PDFPriska FebiolaNo ratings yet
- Piroxicamarticle PDFDocument7 pagesPiroxicamarticle PDFPriska FebiolaNo ratings yet
- Pharmacologictreatment Fortemporomandibular Andtemporomandibularjoint DisordersDocument11 pagesPharmacologictreatment Fortemporomandibular Andtemporomandibularjoint DisordersDušanNo ratings yet
- Daniel HassDocument7 pagesDaniel HasssrinidhiNo ratings yet
- Cycloxygenase Enzymes COX I& IIDocument29 pagesCycloxygenase Enzymes COX I& IISufyan AshrafNo ratings yet
- Mechanisms Underlying The Cardiovascular Effects of COX-InhibitionDocument14 pagesMechanisms Underlying The Cardiovascular Effects of COX-InhibitionRangwani NesbitNo ratings yet
- Cardiovascular Risk of Nonsteroidal Anti-Inflammatory Drugs: An Under-Recognized Public Health IssueDocument12 pagesCardiovascular Risk of Nonsteroidal Anti-Inflammatory Drugs: An Under-Recognized Public Health IssueAri Dwi PrasetyoNo ratings yet
- NsaidDocument29 pagesNsaidAnonymous vMjb3lQOPoNo ratings yet
- Molecules 28 05374Document18 pagesMolecules 28 05374c.poncehenriquez24No ratings yet
- Risk PDFDocument50 pagesRisk PDFErick Antonio Castillo GurdianNo ratings yet
- NsaidDocument29 pagesNsaidEditya Apriliani100% (1)
- N A - D (Nsaid) : Onsteroidal NTI Inflammatory Rugs SDocument43 pagesN A - D (Nsaid) : Onsteroidal NTI Inflammatory Rugs STes B FourieNo ratings yet
- Acetaminofem ReceptorsDocument17 pagesAcetaminofem ReceptorsJuan Sebastian Largo ChaparroNo ratings yet
- Aspirin and Other Anti-Inflammatory Drugs: Sir John VaneDocument8 pagesAspirin and Other Anti-Inflammatory Drugs: Sir John VaneramoncobraNo ratings yet
- Evolution of Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : Cyclooxygenase (Cox) Inhibition and BeyondDocument30 pagesEvolution of Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : Cyclooxygenase (Cox) Inhibition and BeyondnesakusumaNo ratings yet
- EditorialDocument2 pagesEditorialWulandari EmyNo ratings yet
- Cox-1 and Cox-2 Inhibitor For Treatment Acute Chronic Pain, What's The Difference?Document57 pagesCox-1 and Cox-2 Inhibitor For Treatment Acute Chronic Pain, What's The Difference?EmranNo ratings yet
- Cox in Health & Disease.pDocument11 pagesCox in Health & Disease.pSuji SusanthNo ratings yet
- Indomethacin in 700100 PDFDocument28 pagesIndomethacin in 700100 PDFAdrien JacintoNo ratings yet
- 1087 Full PDFDocument7 pages1087 Full PDFTazkiya SalsabilaNo ratings yet
- Perspective: Structural and Functional Basis of Cyclooxygenase InhibitionDocument17 pagesPerspective: Structural and Functional Basis of Cyclooxygenase InhibitionAlexandre Valério MussioNo ratings yet
- Pharma Topic 2 NotesDocument8 pagesPharma Topic 2 NotesAshley Franceska CansanayNo ratings yet
- Aceclofenac For Pain ManagmentDocument11 pagesAceclofenac For Pain Managmentsyeda tahsin naharNo ratings yet
- Cells 11 03596Document16 pagesCells 11 03596Nelson FeitosaNo ratings yet
- Nonsteroidal Antiinflammatory DrugsDocument12 pagesNonsteroidal Antiinflammatory DrugsAlano S. LimgasNo ratings yet
- Selective COX-2 Inhibitors and Risk of Cardiovascular EventsDocument6 pagesSelective COX-2 Inhibitors and Risk of Cardiovascular EventsAditya Rahman RYNo ratings yet
- Farmakodinamika NSAID's TDocument43 pagesFarmakodinamika NSAID's TDantiNo ratings yet
- 8 Aa 1Document9 pages8 Aa 1Edy NoveryNo ratings yet
- Comparative Pathophysiology and Toxicology of CyclooxygenasesFrom EverandComparative Pathophysiology and Toxicology of CyclooxygenasesNo ratings yet
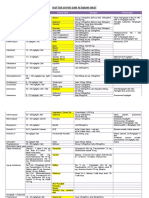
- Daftar Dosis Dan Sediaan ObatDocument7 pagesDaftar Dosis Dan Sediaan Obatdoru ubungNo ratings yet
- Illegal DrugsDocument5 pagesIllegal DrugsJOCELYN VARGASNo ratings yet
- Precedex DosingDocument4 pagesPrecedex DosingnonemiscNo ratings yet
- Different Kinds of Drugs (According To Law)Document4 pagesDifferent Kinds of Drugs (According To Law)PEMS Ivan Theodore P LopezNo ratings yet
- Chlorpheniramina Maleat: Dextromethorphan HBR Minyak Angin Safe Care 10 ML Kasa Streril Husada 16X16Document5 pagesChlorpheniramina Maleat: Dextromethorphan HBR Minyak Angin Safe Care 10 ML Kasa Streril Husada 16X16Ibnu HasanNo ratings yet
- Arrests Linked To Pablo Bergen's Heroin RingDocument6 pagesArrests Linked To Pablo Bergen's Heroin RingSteven BehrNo ratings yet
- OBat High Alert With MerkDocument2 pagesOBat High Alert With MerkMiftahkhul KhusnaNo ratings yet
- Medical Administration RecordDocument1 pageMedical Administration RecorddemereNo ratings yet
- Essential Drug List: (Accessed 24 April 2007)Document47 pagesEssential Drug List: (Accessed 24 April 2007)Ryan Noel Perez de TagleNo ratings yet
- Anti Psychotic DrugsDocument2 pagesAnti Psychotic DrugscalfornianursingacadNo ratings yet
- GA Dengan Intubasi EndotrachealDocument21 pagesGA Dengan Intubasi EndotrachealMuhammad Nur AlamsyahNo ratings yet
- Mental Illness: Antianxiety Agents. Drugs Used To Treat Anxiety Disorders and Symptoms. These IncludeDocument14 pagesMental Illness: Antianxiety Agents. Drugs Used To Treat Anxiety Disorders and Symptoms. These IncludeLeeNo ratings yet
- Kendriya Vidyalaya Kirandul: Investigatory Project of BiologyDocument10 pagesKendriya Vidyalaya Kirandul: Investigatory Project of BiologyAachal GayreNo ratings yet
- Part 3 PNLE MAY 2022 PSYCH MEDS BOOSTERDocument11 pagesPart 3 PNLE MAY 2022 PSYCH MEDS BOOSTERJustine CagatanNo ratings yet
- The Main Causes of Drug AddictionDocument19 pagesThe Main Causes of Drug Addictiongaree maNo ratings yet
- PSB 3441 CH 1 HallucinogensDocument2 pagesPSB 3441 CH 1 HallucinogensAnonymous lm3GIU45No ratings yet
- Presenter: DR Abdul Muhaimin Bin Mat Sulaiman Supervisor: DR SolehinDocument46 pagesPresenter: DR Abdul Muhaimin Bin Mat Sulaiman Supervisor: DR Solehinmatmin07No ratings yet
- Pharmacology 1 - Case Study 1Document2 pagesPharmacology 1 - Case Study 1BaldogNo ratings yet
- Exam 2 UpdatedDocument6 pagesExam 2 Updatedapi-676549138No ratings yet
- LAMOTRIGINEDocument2 pagesLAMOTRIGINEJOHNNo ratings yet
- Yellow List: List of Narcotic Drugs Under International ControlDocument25 pagesYellow List: List of Narcotic Drugs Under International ControlAMSNo ratings yet
- Table 4-16 - Use of Mood Stabilizing Medications For BipolarDocument1 pageTable 4-16 - Use of Mood Stabilizing Medications For BipolarDragutin PetrićNo ratings yet
- WDR23 Exsum Fin SPDocument70 pagesWDR23 Exsum Fin SPVerónica SilveriNo ratings yet
- Receptor Profile of Selected Anti-Psychotic Drugs: Lovely Liana Clapis Sittie Rahani CanacanDocument42 pagesReceptor Profile of Selected Anti-Psychotic Drugs: Lovely Liana Clapis Sittie Rahani CanacanKevin ChanNo ratings yet
- BromazepamDocument6 pagesBromazepamMariusNeicuNo ratings yet
- Module 4Document13 pagesModule 4Cathlyne Mejia NatnatNo ratings yet
- Edited: DR - Dairion Gatot M.Ked SP - PD-KHOMDocument57 pagesEdited: DR - Dairion Gatot M.Ked SP - PD-KHOMayuhati siregarNo ratings yet
- The Effects and Toxicity of Cathinones From The Users' Perspectives - A Qualitative StudyDocument7 pagesThe Effects and Toxicity of Cathinones From The Users' Perspectives - A Qualitative StudyTymon BlaksellNo ratings yet