Download as pdf or txt
You might also like
- Current Surgical Diagnosis and TreatmentDocument1 pageCurrent Surgical Diagnosis and TreatmentM HussainNo ratings yet
- Snap IV InstructionsDocument2 pagesSnap IV Instructionsverouka100% (1)
- Bingo Powerpoint v3 Answers AZCOM RadiologyDocument76 pagesBingo Powerpoint v3 Answers AZCOM Radiologyk5c4s89No ratings yet
- ShoulderDocument4 pagesShoulderRadwa MostafaNo ratings yet
- LumbarDocument9 pagesLumbarMario Rico GonzálezNo ratings yet
- Effect of Cupping Massage and Modified Spinal Decompression Therapy With Exercise Therapy in Neck Radiculopathy SyndromeDocument9 pagesEffect of Cupping Massage and Modified Spinal Decompression Therapy With Exercise Therapy in Neck Radiculopathy SyndromeKhadiga AhmadNo ratings yet
- Manipulación 1Document8 pagesManipulación 1MeryNo ratings yet
- Mulligan Sustained Natural Apophyseal Glides Versus Thoracic Manipulation On Mechanical Neck Pain: A Randomized Controlled StudyDocument12 pagesMulligan Sustained Natural Apophyseal Glides Versus Thoracic Manipulation On Mechanical Neck Pain: A Randomized Controlled StudyAbdul Latiful KhabirNo ratings yet
- Taise Angeli Boff, Fernanda Pasinato, Ângela Jornada Ben, Judith E. Bosmans, Maurits Van Tulder, Rodrigo Luiz CarregaroDocument10 pagesTaise Angeli Boff, Fernanda Pasinato, Ângela Jornada Ben, Judith E. Bosmans, Maurits Van Tulder, Rodrigo Luiz CarregaroNaomiNo ratings yet
- Effect of SNAGS Mulligan Technique On Chronic Cervical Radiculopathy: A Randomized Clinical TrialDocument7 pagesEffect of SNAGS Mulligan Technique On Chronic Cervical Radiculopathy: A Randomized Clinical TrialsdvsdvrNo ratings yet
- 2007 Efficacy of A C1-2 Self SNAG in The Management of Cervicogenic HeadacheDocument8 pages2007 Efficacy of A C1-2 Self SNAG in The Management of Cervicogenic HeadacherdkelsallNo ratings yet
- Effects of Heavy Slow Resistance Training Combined With Corticosteroid Injections or Tendon Needling in Patients With Lateral Elbow TendinopathyDocument10 pagesEffects of Heavy Slow Resistance Training Combined With Corticosteroid Injections or Tendon Needling in Patients With Lateral Elbow TendinopathyaaNo ratings yet
- To Compare The Effects of Maitland MobilizationDocument4 pagesTo Compare The Effects of Maitland MobilizationravichandragoudaNo ratings yet
- Intra-Articular Injection, Subacromial Injection, and Hydrodilatation For Primary Frozen Shoulder: A Randomized Clinical TrialDocument8 pagesIntra-Articular Injection, Subacromial Injection, and Hydrodilatation For Primary Frozen Shoulder: A Randomized Clinical TrialAbhishek JirelNo ratings yet
- Physical Therapy Intervention For Cervicogenic Headache: An Overview of Systematic ReviewsDocument9 pagesPhysical Therapy Intervention For Cervicogenic Headache: An Overview of Systematic ReviewsJoílton OliveiraNo ratings yet
- Shih 2017Document9 pagesShih 2017jayadevanNo ratings yet
- Effectiveness of Adding Rehab of Cervical Related Sensorimotor Control To Manual Therapy and Exercise For Neck PainDocument10 pagesEffectiveness of Adding Rehab of Cervical Related Sensorimotor Control To Manual Therapy and Exercise For Neck Painbcvaughn019No ratings yet
- Multidisciplinary Manual Therapy Management of Cervicogenic Headache: A Case ReportDocument9 pagesMultidisciplinary Manual Therapy Management of Cervicogenic Headache: A Case ReportChirag MunjalNo ratings yet
- Cervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachial Pain: A Randomized Waiting List Controlled Clinical TrialDocument12 pagesCervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachial Pain: A Randomized Waiting List Controlled Clinical TrialFabiana FernandesNo ratings yet
- Contextual Factors Enriched Standard Carei(1)Document12 pagesContextual Factors Enriched Standard Carei(1)Lorena PrimiciaNo ratings yet
- Evidence Based Physiotherapy Management of A Cervical Radiculopathy PatientDocument9 pagesEvidence Based Physiotherapy Management of A Cervical Radiculopathy PatientDr Abdallah BahaaNo ratings yet
- J Jbspin 2021 105198Document8 pagesJ Jbspin 2021 105198gck85fj8pnNo ratings yet
- Neural MobilizationDocument10 pagesNeural MobilizationDonasi YukNo ratings yet
- Ijpr 2019 104 PDFDocument6 pagesIjpr 2019 104 PDFDr. Akshay Pal PTNo ratings yet
- Clinical Effects of Proprioceptive Thumb ExerciseDocument9 pagesClinical Effects of Proprioceptive Thumb Exercisejc596ncf2hNo ratings yet
- Computer Game Assisted Task Specific Exercises Treatment Motor Cognitive FunctionDocument8 pagesComputer Game Assisted Task Specific Exercises Treatment Motor Cognitive FunctionGustavo Casabona MartinsNo ratings yet
- SR 20730194344Document5 pagesSR 20730194344mahdie.amoshahi.1No ratings yet
- Clinical Neurology and Neurosurgery: SciencedirectDocument5 pagesClinical Neurology and Neurosurgery: SciencedirectareteusNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- Agulhamento Seco No Alívio Da Dor Lombalgia Dry Needling BOXEDocument7 pagesAgulhamento Seco No Alívio Da Dor Lombalgia Dry Needling BOXEtaki47685No ratings yet
- This Item Is The Archived Peer-Reviewed Author-Version ofDocument12 pagesThis Item Is The Archived Peer-Reviewed Author-Version ofK scuddsNo ratings yet
- Synapse MirrorTherapyarticle PerezetalDocument7 pagesSynapse MirrorTherapyarticle PerezetalGirijashankar KhuntiaNo ratings yet
- Role of Physiotherapy in The Mobilization of PatieDocument9 pagesRole of Physiotherapy in The Mobilization of PatieroblesguzmanmelisaNo ratings yet
- The Effects of Mulligan Mobilisation Wit PDFDocument5 pagesThe Effects of Mulligan Mobilisation Wit PDFHevin GokulNo ratings yet
- The Effects of Mulligan Mobilisation With Movement and Taping Techniques On Pain, Grip Strength, and Function in Patients With Lateral EpicondylitisDocument5 pagesThe Effects of Mulligan Mobilisation With Movement and Taping Techniques On Pain, Grip Strength, and Function in Patients With Lateral EpicondylitisMawaddah SalehaNo ratings yet
- Hemiplegic Shoulder Pain by Kumat Et AlDocument4 pagesHemiplegic Shoulder Pain by Kumat Et AlAnindira RustandiNo ratings yet
- The Efficacy of Graded Motor Imagery in Post-Traumatic Stiffness of Elbow A Randomized Controlled TrialDocument10 pagesThe Efficacy of Graded Motor Imagery in Post-Traumatic Stiffness of Elbow A Randomized Controlled Trialseroxat2005No ratings yet
- 2055 2386 5 14 PDFDocument8 pages2055 2386 5 14 PDFrima rizky nourliaNo ratings yet
- Effectiveness of Focused Shockwave Therapy Versus Radial Shockwave Therapy For Noncalcific Rotator Cuff Tendinopathies: A Randomized Clinical TrialDocument9 pagesEffectiveness of Focused Shockwave Therapy Versus Radial Shockwave Therapy For Noncalcific Rotator Cuff Tendinopathies: A Randomized Clinical TrialAlessandroNo ratings yet
- Lumbopelvic Stabilization Exercises and Mckenzie Method in Low Back Pain Due To Disc Protrusion: A Blind Randomized Clinical TrialDocument12 pagesLumbopelvic Stabilization Exercises and Mckenzie Method in Low Back Pain Due To Disc Protrusion: A Blind Randomized Clinical TrialZahra SativaniNo ratings yet
- Manual Therapy: Susan A. Reid, Robin Callister, Suzanne J. Snodgrass, Michael G. Katekar, Darren A. RivettDocument9 pagesManual Therapy: Susan A. Reid, Robin Callister, Suzanne J. Snodgrass, Michael G. Katekar, Darren A. Rivettubiktrash1492No ratings yet
- Meta-Analysis - Hypnosis For PainDocument17 pagesMeta-Analysis - Hypnosis For PainmalwinatmdNo ratings yet
- Development and Implementation of The Physiotherapy-Led Exercise Interventions For The Treatment of Rotator Cuff DisordersDocument15 pagesDevelopment and Implementation of The Physiotherapy-Led Exercise Interventions For The Treatment of Rotator Cuff Disorderselmathy1998No ratings yet
- NiceDocument7 pagesNiceRisky Ilona SaputraNo ratings yet
- Clinical StudyDocument9 pagesClinical StudyJavierAntonioMéndezNo ratings yet
- Jurnal Imggris Corset For LBPDocument4 pagesJurnal Imggris Corset For LBPnanik setiyowatiNo ratings yet
- Effect Observation of Electro Acupunctute AnesthesiaDocument7 pagesEffect Observation of Electro Acupunctute Anesthesiaadink mochammadNo ratings yet
- Utilization of Concurrent Dorsal Root Ganglion Stimulation and Dorsal Column Spinal Cord Stimulation in Complex Regional Pain SyndromeDocument5 pagesUtilization of Concurrent Dorsal Root Ganglion Stimulation and Dorsal Column Spinal Cord Stimulation in Complex Regional Pain Syndromemarcus moraisNo ratings yet
- Jurnal 1Document7 pagesJurnal 1Dian NellisaNo ratings yet
- Effect of Mulligan Concept Lumbar SNAG On Chronic Nonspecific Low Back PainDocument10 pagesEffect of Mulligan Concept Lumbar SNAG On Chronic Nonspecific Low Back PainFebryanti Fisio2019No ratings yet
- ptrs009 03 03 PDFDocument6 pagesptrs009 03 03 PDFGusti Ayu KrisnayantiNo ratings yet
- 10 1016@j Jocn 2019 07 009Document6 pages10 1016@j Jocn 2019 07 009ravencrowneurNo ratings yet
- 10 1016@j Physio 2019 11 002Document27 pages10 1016@j Physio 2019 11 002Milton Ricardo de Medeiros FernandesNo ratings yet
- A Review of Current Treatment Options For CoccygodyniaDocument8 pagesA Review of Current Treatment Options For CoccygodyniaClara ViMiNo ratings yet
- Musculoskeletal Science and PracticeDocument11 pagesMusculoskeletal Science and PracticeAnii warikarNo ratings yet
- The Effect of Muscle Energy Technique On HeadacheDocument10 pagesThe Effect of Muscle Energy Technique On HeadacheDavid FehertyNo ratings yet
- SH 2Document14 pagesSH 2ع الNo ratings yet
- Selective Dorsal Rhizotomy For The Treatment of Severe Spastic Cerebral Palsy - Efficacy and Therapeutic Durability in GMFCS Grade IV and V ChildrenDocument11 pagesSelective Dorsal Rhizotomy For The Treatment of Severe Spastic Cerebral Palsy - Efficacy and Therapeutic Durability in GMFCS Grade IV and V ChildrenAlvaro Perez HenriquezNo ratings yet
- 2017 - Article - 65 2 PDFDocument11 pages2017 - Article - 65 2 PDFPaulina Sobarzo VegaNo ratings yet
- BurstDr Visceral PainDocument11 pagesBurstDr Visceral Painnavid.amirabadiNo ratings yet
- Manual of Vibration Exercise and Vibration TherapyFrom EverandManual of Vibration Exercise and Vibration TherapyJörn RittwegerNo ratings yet
- Strengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesFrom EverandStrengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesNo ratings yet
- ATMS Minimum Education Standards MyotherapyDocument7 pagesATMS Minimum Education Standards MyotherapyBal Mukund JhaNo ratings yet
- Peters 2012Document7 pagesPeters 2012Bal Mukund JhaNo ratings yet
- KP COVID ReportDocument2 pagesKP COVID ReportBal Mukund JhaNo ratings yet
- SGG Glass NoteDocument6 pagesSGG Glass NoteBal Mukund JhaNo ratings yet
- Home Exercise ProgramDocument21 pagesHome Exercise ProgramBal Mukund JhaNo ratings yet
- Class 6 Formulae MathsDocument11 pagesClass 6 Formulae MathsBal Mukund JhaNo ratings yet
- From Frail To Function To Fun: Section On Geriatrics American Physical Therapy AssociationDocument37 pagesFrom Frail To Function To Fun: Section On Geriatrics American Physical Therapy AssociationBal Mukund JhaNo ratings yet
- Autism and EpilepsyDocument5 pagesAutism and Epilepsyclarajimena25No ratings yet
- Influencing Factors On Hypertension Medication Adherence at Kampala International University Teaching Hospital in Ishaka, UgandaDocument17 pagesInfluencing Factors On Hypertension Medication Adherence at Kampala International University Teaching Hospital in Ishaka, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- RESEARCH PROPOSAL - 3 Nov 2013 PDFDocument27 pagesRESEARCH PROPOSAL - 3 Nov 2013 PDFWestley AbluyenNo ratings yet
- KKD3103 - Chapter 14 - Week 10 - SVDocument38 pagesKKD3103 - Chapter 14 - Week 10 - SVSYIFAA ATHIRAH BINTI SABRINo ratings yet
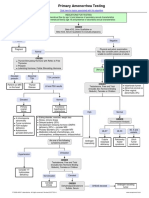
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Updates On The Treatment of Pterygium: Serbian Journal of Experimental and Clinical Research September 2016Document7 pagesUpdates On The Treatment of Pterygium: Serbian Journal of Experimental and Clinical Research September 2016Arfadin YusufNo ratings yet
- Alex Hardin Resume 2015Document3 pagesAlex Hardin Resume 2015api-306883462No ratings yet
- Authorization To Walk HomeDocument50 pagesAuthorization To Walk HomeAidan FranciscoNo ratings yet
- 2006D September AMC MCQ Recall QuestionsDocument13 pages2006D September AMC MCQ Recall QuestionsTehreem KhanNo ratings yet
- PSC Advert - 23.02.2021Document48 pagesPSC Advert - 23.02.2021Muchiri Nahashon100% (1)
- Inspiratory Muscle TrainingDocument15 pagesInspiratory Muscle Trainingulfapanjaitan100% (2)
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanJarda DacuagNo ratings yet
- COPD - Jindal Chest ClinicDocument31 pagesCOPD - Jindal Chest ClinicJindal Chest ClinicNo ratings yet
- Social & Preventive Pharmacy (Thakur Publication) - 1Document218 pagesSocial & Preventive Pharmacy (Thakur Publication) - 1Manav Patel100% (1)
- What Living As A Resident Can Teach Long-Term Care Staff: The Power of Empathy To Transform Care (Excerpt)Document14 pagesWhat Living As A Resident Can Teach Long-Term Care Staff: The Power of Empathy To Transform Care (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.No ratings yet
- Study Closely The Concept Map On Sudden Pregnancy ComplicationsDocument13 pagesStudy Closely The Concept Map On Sudden Pregnancy ComplicationsJek Dela CruzNo ratings yet
- Progressive Mobility in The Critically Ill PDFDocument15 pagesProgressive Mobility in The Critically Ill PDFydtrgnNo ratings yet
- Are Current Clinical Studies On Artificial Intelligence-Based Medical DevicesDocument13 pagesAre Current Clinical Studies On Artificial Intelligence-Based Medical Devicesmgw backupdataNo ratings yet
- Viral HepatitisDocument26 pagesViral HepatitisNasriah MacadatoNo ratings yet
- Links para Baixar Livros VeterináriosDocument14 pagesLinks para Baixar Livros VeterináriosBrunaFernandes33% (9)
- Cerebrovascular Accident - CaseDocument18 pagesCerebrovascular Accident - CaseHazel AsperaNo ratings yet
- We Need Minimally Disruptive Medicine: AnalysisDocument3 pagesWe Need Minimally Disruptive Medicine: Analysisapi-252646029No ratings yet
- Nurse To Nurse Bedside Shift Report LB 5th WeekDocument12 pagesNurse To Nurse Bedside Shift Report LB 5th Weekapi-527286440No ratings yet
- Dissociative DisordersDocument24 pagesDissociative DisordersSimón Ortiz LondoñoNo ratings yet
- IGNOU Block 4 Unit 3 Non-Communicable Diseases 2Document13 pagesIGNOU Block 4 Unit 3 Non-Communicable Diseases 2erice.researchNo ratings yet
- Rickettsial DiseasesDocument44 pagesRickettsial DiseasesPrince AlexNo ratings yet