Download as docx, pdf, or txt
You might also like
- Biophysical Profile PDFDocument1 pageBiophysical Profile PDFmp1757No ratings yet
- Scientific Principles of Strength TrainingDocument38 pagesScientific Principles of Strength Trainingarkko5585% (13)
- MSC Nursing QN PaperDocument9 pagesMSC Nursing QN Papersanthyakunjumon100% (1)
- Bag Technique Checklists CHN 1 (SL)Document3 pagesBag Technique Checklists CHN 1 (SL)Krisa AdornaNo ratings yet
- Modified Braden Q ScaleDocument1 pageModified Braden Q ScaleGrace Simarmata100% (1)
- Oisd GDN 166Document64 pagesOisd GDN 166sgh1355100% (5)
- APGAR Scoring Written ReportDocument2 pagesAPGAR Scoring Written ReportFaith MarfilNo ratings yet
- A. KMC Introduction, Components & BenefitsDocument25 pagesA. KMC Introduction, Components & BenefitssantojuliansyahNo ratings yet
- Bag TechniqueDocument1 pageBag TechniquejesperdomincilbayauaNo ratings yet
- Exercises To Facilitate Change of Baby's Position From Breech To CephalicDocument3 pagesExercises To Facilitate Change of Baby's Position From Breech To CephalicaziskarnNo ratings yet
- Procedure Checklist Chapter 21: Using RestraintsDocument1 pageProcedure Checklist Chapter 21: Using RestraintsjthsNo ratings yet
- Essential Newborn Care ProtocolDocument23 pagesEssential Newborn Care ProtocolKaren Viviene CincoNo ratings yet
- Perineal CareDocument4 pagesPerineal CareJny SherpaNo ratings yet
- Randomized Trial of Plastic Bags To Prevent TermDocument8 pagesRandomized Trial of Plastic Bags To Prevent TermkemalmiaNo ratings yet
- Topic - Breast Feeding Subject - Pediatrics Unit - Ii: Prepared by - Mr. Dinesh Khinchi H.O.D Pediatrics Kinsr KanpurDocument14 pagesTopic - Breast Feeding Subject - Pediatrics Unit - Ii: Prepared by - Mr. Dinesh Khinchi H.O.D Pediatrics Kinsr KanpurDinesh KhinchiNo ratings yet
- Post Op Bed Making ChecklistDocument6 pagesPost Op Bed Making ChecklistRoselyn Y. QuintoNo ratings yet
- Cpms College of Nursing Assignment ON Oral Medication: DATED: 18 MAY, 2021 Subject: Child Health NursingDocument4 pagesCpms College of Nursing Assignment ON Oral Medication: DATED: 18 MAY, 2021 Subject: Child Health NursingAmy LalringhluaniNo ratings yet
- Therapeutic Back Massage: College of NursingDocument1 pageTherapeutic Back Massage: College of NursingCarol Neng CalupitanNo ratings yet
- Immediate Care of The NewbornDocument8 pagesImmediate Care of The NewbornksjsellsNo ratings yet
- NCM 107 SL (Care of Mother, Child, Adolescent) Ballard ScoringDocument7 pagesNCM 107 SL (Care of Mother, Child, Adolescent) Ballard ScoringclrssNo ratings yet
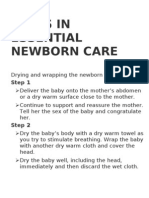
- Steps in Essential Newborn CareDocument12 pagesSteps in Essential Newborn CareCedy L. CieloNo ratings yet
- Vital SignDocument4 pagesVital SignGabriel JocsonNo ratings yet
- RD ManualDocument6 pagesRD Manualapple m.No ratings yet
- Anthropometric Measurements and Weighing ChecklistDocument4 pagesAnthropometric Measurements and Weighing ChecklistAnnica LozanoNo ratings yet
- WeaningDocument15 pagesWeaningArchana SahuNo ratings yet
- 01-Health Behavior QuestionnaireDocument3 pages01-Health Behavior QuestionnaireZhi Li50% (2)
- Assessment of The NewbornDocument57 pagesAssessment of The Newbornmuiz muhammadNo ratings yet
- Case Study-Infant With Fluid Imbalance08-10-KEYDocument3 pagesCase Study-Infant With Fluid Imbalance08-10-KEYreecoleNo ratings yet
- PhototherapyDocument3 pagesPhototherapyNicole PageNo ratings yet
- ApgarDocument13 pagesApgarAneesh MyneniNo ratings yet
- Bag TechniqueDocument5 pagesBag TechniqueGaganNo ratings yet
- NICU Aim and ObjectivesDocument1 pageNICU Aim and ObjectivesskylertNo ratings yet
- Incubator Care 1Document4 pagesIncubator Care 1Mayank KumarNo ratings yet
- Protracted LabourDocument20 pagesProtracted Labourkhadzx100% (2)
- Case StudyDocument5 pagesCase StudyJui Perano100% (2)
- Importance of Assessing NewbornDocument9 pagesImportance of Assessing NewbornMaria Alena Rose SalmeroNo ratings yet
- Partograph: Source: Basic Emergency Obstetric Care Dr. Jose Fabella Memorial Hospital, & Who By: Araceli F. SuratDocument33 pagesPartograph: Source: Basic Emergency Obstetric Care Dr. Jose Fabella Memorial Hospital, & Who By: Araceli F. SuratRaquel MonsalveNo ratings yet
- New Born ClassificationDocument47 pagesNew Born ClassificationEyob MizanNo ratings yet
- Essential Intrapartum and Newborn Care Practice Session ChecklistDocument28 pagesEssential Intrapartum and Newborn Care Practice Session ChecklistMonica Melchor DoriaNo ratings yet
- Presentation Abnormal PuerperiumDocument52 pagesPresentation Abnormal PuerperiumTesfaye AbebeNo ratings yet
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNo ratings yet
- Urinary Catheterization For PediatricsDocument6 pagesUrinary Catheterization For PediatricsMichael Montinola100% (1)
- Nursing Procedure Checklist: Administering An Ear IrrigationDocument1 pageNursing Procedure Checklist: Administering An Ear IrrigationOrl Trinidad0% (1)
- Changing Trends in Hospital CareDocument10 pagesChanging Trends in Hospital Carejay dewanagn100% (1)
- Nursing Care of A Neonate Part 1Document67 pagesNursing Care of A Neonate Part 1Rani G SNo ratings yet
- Umbilical Cord CareDocument11 pagesUmbilical Cord Carekristel ludangcoNo ratings yet
- NewbornDocument45 pagesNewbornkiran kumarNo ratings yet
- Topic #15 Health Promotion During Pregnancy-Self Care NeedsDocument4 pagesTopic #15 Health Promotion During Pregnancy-Self Care NeedsMadayag, Mary Faith U.No ratings yet
- Phototherapy On The Postnatal WardDocument5 pagesPhototherapy On The Postnatal WardYwagar Ywagar100% (1)
- PV ChecklistDocument2 pagesPV ChecklistNidhi Shivam AhlawatNo ratings yet
- WHO Labour Care GuideDocument34 pagesWHO Labour Care GuideAnkita Singh100% (1)
- Cardio Vascular Nursing Care PlanDocument10 pagesCardio Vascular Nursing Care PlanUday KumarNo ratings yet
- Infant Radiant WarmerDocument7 pagesInfant Radiant WarmerManish MandaviyaNo ratings yet
- Assignment On IncubatorDocument12 pagesAssignment On IncubatorNeetaNo ratings yet
- Unit 3 Dev Psy-InfancyDocument31 pagesUnit 3 Dev Psy-InfancySikander MalikNo ratings yet
- Oropharyngeal and Nasopharyngeal SuctioningDocument2 pagesOropharyngeal and Nasopharyngeal SuctioningAlana Caballero100% (1)
- How To Do Tepid Sponge Bath: InstructionsDocument2 pagesHow To Do Tepid Sponge Bath: Instructionssuandi isindaNo ratings yet
- Psychological Perspective of Abnormal LaborDocument25 pagesPsychological Perspective of Abnormal LaborPriscilla Sarah PayneNo ratings yet
- DehydrationDocument16 pagesDehydrationBenben LookitandI'mNo ratings yet
- Newborn ResuscitationDocument7 pagesNewborn ResuscitationYwagar YwagarNo ratings yet
- Immediate Care of The NewbornDocument11 pagesImmediate Care of The NewbornHannahKarizaNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Admintrationofmedications1 Copy 181202173921Document186 pagesAdmintrationofmedications1 Copy 181202173921Karl RobleNo ratings yet
- Echocardiogram: Echocardiogram, Also Known As Echocardiography, or Heart Ultrasound Is ADocument23 pagesEchocardiogram: Echocardiogram, Also Known As Echocardiography, or Heart Ultrasound Is AKarl RobleNo ratings yet
- Instructional Plan Career PathDocument6 pagesInstructional Plan Career PathKarl RobleNo ratings yet
- Guide Blood Component and Blood Product AdministrationDocument10 pagesGuide Blood Component and Blood Product AdministrationKarl RobleNo ratings yet
- Coagulation Reconstitution Reference Binder Part 1 Updated July 2021Document39 pagesCoagulation Reconstitution Reference Binder Part 1 Updated July 2021Karl RobleNo ratings yet
- Blood Transfusion TherapyDocument11 pagesBlood Transfusion TherapyKarl RobleNo ratings yet
- Emilio Aguinaldo Highway, By-Pass Road, San Vicente Ii, Silang, Cavite E-Mail: Contact Nos: (046) 482-9999, (02) 584-4053Document2 pagesEmilio Aguinaldo Highway, By-Pass Road, San Vicente Ii, Silang, Cavite E-Mail: Contact Nos: (046) 482-9999, (02) 584-4053Karl RobleNo ratings yet
- Elements of Informed Consent For Blood and Blood ProductsDocument2 pagesElements of Informed Consent For Blood and Blood ProductsKarl RobleNo ratings yet
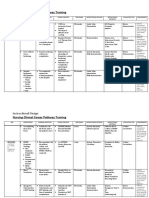
- Training Design COVID-19 Immunization Training I. RationaleDocument4 pagesTraining Design COVID-19 Immunization Training I. RationaleKarl RobleNo ratings yet
- Patient Rights & ResponsibilitiesDocument5 pagesPatient Rights & ResponsibilitiesKarl RobleNo ratings yet
- Pre-Employment Testing To Improve Nurse RetentionDocument50 pagesPre-Employment Testing To Improve Nurse RetentionKarl RobleNo ratings yet
- Breath Sounds: ConsiderationsDocument10 pagesBreath Sounds: ConsiderationsKarl RobleNo ratings yet
- Auscultation of Lung Sounds and MurmursDocument8 pagesAuscultation of Lung Sounds and MurmursKarl RobleNo ratings yet
- Dole/Bwc/Ohsd/Ip-5: ST ST STDocument2 pagesDole/Bwc/Ohsd/Ip-5: ST ST STKarl RobleNo ratings yet
- Phlebitis Infiltration and Localized Site InfectioDocument24 pagesPhlebitis Infiltration and Localized Site InfectioKarl RobleNo ratings yet
- Storage Handling ToolkitDocument65 pagesStorage Handling ToolkitKarl RobleNo ratings yet
- Philippine Health Insurance CorporationDocument2 pagesPhilippine Health Insurance CorporationKarl RobleNo ratings yet
- Algorithm For Prevention of Rabies After Animal Encounters in OregonDocument2 pagesAlgorithm For Prevention of Rabies After Animal Encounters in OregonKarl RobleNo ratings yet
- Evidence-Based Case Report: Kartiwa Hadi NuryantoDocument20 pagesEvidence-Based Case Report: Kartiwa Hadi NuryantohfathiardiNo ratings yet
- Philips Titration Protocol 2017Document12 pagesPhilips Titration Protocol 2017Sam WhiteNo ratings yet
- Liberty (Art. 21) : ProtectionDocument15 pagesLiberty (Art. 21) : ProtectionA2 Sir Fan PageNo ratings yet
- 11 Ways To Live A Happier LifeDocument5 pages11 Ways To Live A Happier LifeHannah Grace Tan GerminaNo ratings yet
- Consent Form - EmployerDocument1 pageConsent Form - EmployerShankarr Kshan100% (1)
- Care and Management of Turkey, Duck andDocument35 pagesCare and Management of Turkey, Duck andShealla Pis-oNo ratings yet
- Hygienia EnglishDocument40 pagesHygienia EnglishAsanga MalNo ratings yet
- Research Jan ClarenzDocument6 pagesResearch Jan ClarenzBiboy De ungriaNo ratings yet
- NURSING CARE PLAN - Impaired Urinary EliminationDocument2 pagesNURSING CARE PLAN - Impaired Urinary EliminationDaniel Andre S. SomorayNo ratings yet
- Safety Rules in The Science LaboratoryDocument4 pagesSafety Rules in The Science LaboratoryJaznMonNo ratings yet
- Job Description: Cardiff and Vale University Health Board Job DetailsDocument9 pagesJob Description: Cardiff and Vale University Health Board Job DetailsmustakNo ratings yet
- Construction Safety Program TemplateDocument15 pagesConstruction Safety Program TemplateSole Kicks PHNo ratings yet
- Child AbuseDocument3 pagesChild Abusemariazubair990No ratings yet
- A Day in The Life of A Social WORKER JENNY ROSE SINDONDocument13 pagesA Day in The Life of A Social WORKER JENNY ROSE SINDONma.cristina ginesNo ratings yet
- Design Guidelines HospitalDocument39 pagesDesign Guidelines HospitalKhaled FacebNo ratings yet
- Plugin-Introduction To CPT Medical Billing 101Document47 pagesPlugin-Introduction To CPT Medical Billing 101fiesty7971% (7)
- Iec 62443 3 2 2020Document12 pagesIec 62443 3 2 2020steveNo ratings yet
- Pe3 Module No. 2 Dance Related InjuriesDocument7 pagesPe3 Module No. 2 Dance Related InjuriesGabo AlfonsoNo ratings yet
- Wasynczuk CV May 2018Document6 pagesWasynczuk CV May 2018api-403363741No ratings yet
- Ismenore: You Should Also DoDocument2 pagesIsmenore: You Should Also DoNurul Ilmi UtamiNo ratings yet
- Assasment, Treatment CelulitisDocument7 pagesAssasment, Treatment CelulitisSulistiyawati CuplizNo ratings yet
- Rural Libraries, Village Knowledge Centre (VKC) and Concept of Rural Libraries and Knowledge Centre (RLKC) Bishnu Prasad Upadhaya, Ghanakanta Baruah College, Morigaon.Document3 pagesRural Libraries, Village Knowledge Centre (VKC) and Concept of Rural Libraries and Knowledge Centre (RLKC) Bishnu Prasad Upadhaya, Ghanakanta Baruah College, Morigaon.bishnupoudelNo ratings yet
- Determination of Ascorbic Acid: Analytical Chemistry IVDocument9 pagesDetermination of Ascorbic Acid: Analytical Chemistry IVashNo ratings yet
- User ManualDocument136 pagesUser ManualConstantin StratulescuNo ratings yet
- Depression: Based StatsDocument9 pagesDepression: Based StatsPinky EclarinalNo ratings yet
- McCann Food Additives and Hyperactive Behaviour PDFDocument8 pagesMcCann Food Additives and Hyperactive Behaviour PDFDiego Bermudez NaranjoNo ratings yet
- GastroparesisDocument31 pagesGastroparesisGaby ZuritaNo ratings yet