Download as pdf or txt
You might also like
- Lab Policies Sysmex XN 450 XN 550 Lab 1532Document25 pagesLab Policies Sysmex XN 450 XN 550 Lab 1532Nguyen Tien Trinh100% (5)
- SLEEP HYGIENE INDEX DrWendieRobbins PDFDocument1 pageSLEEP HYGIENE INDEX DrWendieRobbins PDFrinaldy andriansyahNo ratings yet
- Blood Transfusion LectureDocument8 pagesBlood Transfusion LectureCamille Cirineo Arensol100% (2)
- Lesson 36 Administering Blood ProductsDocument3 pagesLesson 36 Administering Blood ProductsDarren RossNo ratings yet
- Investigation of FMH by Flow CytometryDocument15 pagesInvestigation of FMH by Flow CytometryMohammed Khair BashirNo ratings yet
- Advanced Diagnostic Immunohematology and Blood BankDocument6 pagesAdvanced Diagnostic Immunohematology and Blood BankYaseen MohamnadNo ratings yet
- Blood and Blood Products Therapy PolicyDocument3 pagesBlood and Blood Products Therapy PolicymarataningutukuNo ratings yet
- Laboratory Unit 2Document6 pagesLaboratory Unit 2Mushy_ayaNo ratings yet
- Blood TransfusionDocument9 pagesBlood Transfusionlayla alyamiNo ratings yet
- WF Lab Clin TM RbcsDocument3 pagesWF Lab Clin TM RbcsVidini Kusuma AjiNo ratings yet
- Blood Transfusion PolicyDocument6 pagesBlood Transfusion PolicyTanisha SinghNo ratings yet
- Training and Competency Assessment in Blood Transfusion TherapyDocument7 pagesTraining and Competency Assessment in Blood Transfusion Therapyjake_caballo23No ratings yet
- Blood Transfusion: A Clinician's ReferenceDocument32 pagesBlood Transfusion: A Clinician's Referenceلوريس أبو الفتوحNo ratings yet
- Blood TransfusionDocument57 pagesBlood Transfusionggrrk7100% (2)
- ABO Reagent RBCDocument6 pagesABO Reagent RBCtahirnawazawanNo ratings yet
- Blood TransfusionDocument6 pagesBlood TransfusionRoxanne Quiñones GelacioNo ratings yet
- Package Insert Reagent Red Blood Cells A1 Cells B CellsDocument6 pagesPackage Insert Reagent Red Blood Cells A1 Cells B CellsAbdulwahab Mohamud AbdiNo ratings yet
- Blood Transfusion SLPDocument10 pagesBlood Transfusion SLPLovesehun OhNo ratings yet
- Massive TransfusionDocument3 pagesMassive Transfusionthd3rNo ratings yet
- Blood TransfusionDocument22 pagesBlood Transfusiondeepak_143No ratings yet
- Blood Transfusion On Dialysis Guidelines Aug 2017 PDFDocument5 pagesBlood Transfusion On Dialysis Guidelines Aug 2017 PDFYolanda IrawatiNo ratings yet
- Blood Transfusion PracticeDocument18 pagesBlood Transfusion Practicedave king BelayNo ratings yet
- Blood TransfusionDocument10 pagesBlood TransfusionMitch SierrasNo ratings yet
- Administering A Blood TransfusionDocument7 pagesAdministering A Blood TransfusionAndrea Bayaga WaganNo ratings yet
- Blood Transfusion Whole Blood: Right Blood Component Right Time Right ReasonDocument13 pagesBlood Transfusion Whole Blood: Right Blood Component Right Time Right ReasonalysalorenoNo ratings yet
- A-1200 Methods Intro enDocument9 pagesA-1200 Methods Intro enMARICENo ratings yet
- Blood Transfusion InstructionsDocument17 pagesBlood Transfusion InstructionsMuthuraj KasinathanNo ratings yet
- Blood Administration: NRS 108 Essec County CollegeDocument22 pagesBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniNo ratings yet
- Manual Cell Count and Differential For Body Fluid and CSFDocument14 pagesManual Cell Count and Differential For Body Fluid and CSFendale gebregzabherNo ratings yet
- Returning Blood Components and Blood Products Into InventoryDocument6 pagesReturning Blood Components and Blood Products Into InventoryAnonymous jaOTeMMI2No ratings yet
- Blood ProductsDocument41 pagesBlood ProductsrijjorajooNo ratings yet
- ERBA ELite 3 ControlsDocument1 pageERBA ELite 3 ControlsGlobalindo Center MedicalNo ratings yet
- SOP For ABO GroupingDocument5 pagesSOP For ABO GroupingDUKENo ratings yet
- ISBT Science Series - 2008 - Armstrong - Benefits and Risks of TransfusionDocument15 pagesISBT Science Series - 2008 - Armstrong - Benefits and Risks of TransfusionFatima AddaNo ratings yet
- Reception Flow Chart: Sample ReceiptDocument10 pagesReception Flow Chart: Sample ReceiptDcas RianneNo ratings yet
- Guidelines For Gamma Irradiation of Blood Components: A ZSBT NDocument8 pagesGuidelines For Gamma Irradiation of Blood Components: A ZSBT NDiego Martin RabasedasNo ratings yet
- Blood Transfusion Therapy DefinitionDocument27 pagesBlood Transfusion Therapy DefinitionEvangelin MelvinNo ratings yet
- Blood Transfusion WordDocument8 pagesBlood Transfusion WordKaren Angela Panganiban100% (1)
- University of Santo Tomas Immunohematology and Transfusion MedicineDocument7 pagesUniversity of Santo Tomas Immunohematology and Transfusion MedicineWynlor Abarca100% (1)
- Blood Transfusion WordDocument6 pagesBlood Transfusion WordRachel Julianne MoralesNo ratings yet
- RT.011 Antiglobulin Crossmatch (Saline-LISS-PEG)Document12 pagesRT.011 Antiglobulin Crossmatch (Saline-LISS-PEG)Osama BakheetNo ratings yet
- Blood TransfusionDocument2 pagesBlood TransfusionChristian Anthony L. GamoloNo ratings yet
- Hepc e Met Hep C RibaDocument22 pagesHepc e Met Hep C Ribaعائش العموديNo ratings yet
- BD - Bulk Erythrocyte Lysing With Ammonium Chloride For Flow Cytometry ImmunophenotypingDocument3 pagesBD - Bulk Erythrocyte Lysing With Ammonium Chloride For Flow Cytometry ImmunophenotypingBcells AutoimmunityNo ratings yet
- Cavite State University: Don Severino Delas Alas CampusDocument7 pagesCavite State University: Don Severino Delas Alas CampusCharmaine Dela CruzNo ratings yet
- Blood TransfusionDocument5 pagesBlood TransfusionCla67% (3)
- Exchange TransfusionDocument11 pagesExchange TransfusionThangam jayaraniNo ratings yet
- Blood TransfusionDocument7 pagesBlood TransfusionJustin GallemitNo ratings yet
- Compatibility TestingDocument36 pagesCompatibility TestingCharmaine Corpuz Granil100% (1)
- PMLS 2 Unit 8Document4 pagesPMLS 2 Unit 8Elyon Jirehel AlvarezNo ratings yet
- Neonatal Exchange TransfusionDocument33 pagesNeonatal Exchange TransfusionedrinsneNo ratings yet
- Blood TransfusionDocument5 pagesBlood Transfusionrupali gahalianNo ratings yet
- Blood Transfusion PocedureDocument9 pagesBlood Transfusion PocedureRaman Samrao100% (1)
- Policies and Procedures of Laboratory Services in Each AreaDocument10 pagesPolicies and Procedures of Laboratory Services in Each AreaDarren CarinoNo ratings yet
- Maternal 2 - Blood TransfusionDocument5 pagesMaternal 2 - Blood TransfusionJuliana Anne RamosNo ratings yet
- Blood Transfusion Procedure Checklist 2Document3 pagesBlood Transfusion Procedure Checklist 2Rainier CervantesNo ratings yet
- Insert - PreciControl ClinChem Multi 1.05117020001.v7.enDocument2 pagesInsert - PreciControl ClinChem Multi 1.05117020001.v7.enVegha Nedya100% (1)
- ASTM 71830-97 - Standard Practice For Selection of Blood For in Vitro Evaluation of Blood PumpsDocument2 pagesASTM 71830-97 - Standard Practice For Selection of Blood For in Vitro Evaluation of Blood PumpsJoãoNo ratings yet
- Practical Transfusion Medicine for the Small Animal PractitionerFrom EverandPractical Transfusion Medicine for the Small Animal PractitionerNo ratings yet
- Mollison's Blood Transfusion in Clinical MedicineFrom EverandMollison's Blood Transfusion in Clinical MedicineRating: 4.5 out of 5 stars4.5/5 (1)
- Admintrationofmedications1 Copy 181202173921Document186 pagesAdmintrationofmedications1 Copy 181202173921Karl RobleNo ratings yet
- Emilio Aguinaldo Highway, By-Pass Road, San Vicente Ii, Silang, Cavite E-Mail: Contact Nos: (046) 482-9999, (02) 584-4053Document2 pagesEmilio Aguinaldo Highway, By-Pass Road, San Vicente Ii, Silang, Cavite E-Mail: Contact Nos: (046) 482-9999, (02) 584-4053Karl RobleNo ratings yet
- Instructional Plan Career PathDocument6 pagesInstructional Plan Career PathKarl RobleNo ratings yet
- Coagulation Reconstitution Reference Binder Part 1 Updated July 2021Document39 pagesCoagulation Reconstitution Reference Binder Part 1 Updated July 2021Karl RobleNo ratings yet
- Elements of Informed Consent For Blood and Blood ProductsDocument2 pagesElements of Informed Consent For Blood and Blood ProductsKarl RobleNo ratings yet
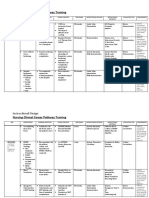
- Training Design COVID-19 Immunization Training I. RationaleDocument4 pagesTraining Design COVID-19 Immunization Training I. RationaleKarl RobleNo ratings yet
- Blood Transfusion TherapyDocument11 pagesBlood Transfusion TherapyKarl RobleNo ratings yet
- Echocardiogram: Echocardiogram, Also Known As Echocardiography, or Heart Ultrasound Is ADocument23 pagesEchocardiogram: Echocardiogram, Also Known As Echocardiography, or Heart Ultrasound Is AKarl RobleNo ratings yet
- Pre-Employment Testing To Improve Nurse RetentionDocument50 pagesPre-Employment Testing To Improve Nurse RetentionKarl RobleNo ratings yet
- Auscultation of Lung Sounds and MurmursDocument8 pagesAuscultation of Lung Sounds and MurmursKarl RobleNo ratings yet
- Patient Rights & ResponsibilitiesDocument5 pagesPatient Rights & ResponsibilitiesKarl RobleNo ratings yet
- Apgar Score: How The Test Is PerformedDocument27 pagesApgar Score: How The Test Is PerformedKarl RobleNo ratings yet
- Breath Sounds: ConsiderationsDocument10 pagesBreath Sounds: ConsiderationsKarl RobleNo ratings yet
- Dole/Bwc/Ohsd/Ip-5: ST ST STDocument2 pagesDole/Bwc/Ohsd/Ip-5: ST ST STKarl RobleNo ratings yet
- Phlebitis Infiltration and Localized Site InfectioDocument24 pagesPhlebitis Infiltration and Localized Site InfectioKarl RobleNo ratings yet
- Storage Handling ToolkitDocument65 pagesStorage Handling ToolkitKarl RobleNo ratings yet
- Philippine Health Insurance CorporationDocument2 pagesPhilippine Health Insurance CorporationKarl RobleNo ratings yet
- Algorithm For Prevention of Rabies After Animal Encounters in OregonDocument2 pagesAlgorithm For Prevention of Rabies After Animal Encounters in OregonKarl RobleNo ratings yet
- Stages of SleepDocument1 pageStages of Sleepapi-461452779No ratings yet
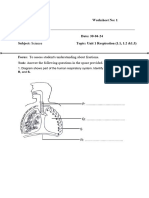
- 01 Respiratory SystemDocument15 pages01 Respiratory Systemnaseer alfahdNo ratings yet
- Sleep Studies: in The Sleep Laboratory and in The Home: Patient EducationDocument2 pagesSleep Studies: in The Sleep Laboratory and in The Home: Patient EducationALINo ratings yet
- Z020201t-A First Aid..Document24 pagesZ020201t-A First Aid..NkNo ratings yet
- Semi Detailed Lesson Plan Using 5esDocument2 pagesSemi Detailed Lesson Plan Using 5esrondariopearldawnNo ratings yet
- Chapter - 2 NCERT SolutionsDocument7 pagesChapter - 2 NCERT SolutionsPugalmeena PugalmeenaNo ratings yet
- Medical Surgical Nursing Lab Oxygenation To Suctioning of Tracheostomy QuestionsDocument6 pagesMedical Surgical Nursing Lab Oxygenation To Suctioning of Tracheostomy Questionsclaire dimaano (colosus)No ratings yet
- GR 10 Life Sciences IEB 3 in 1 Extracts PDFDocument16 pagesGR 10 Life Sciences IEB 3 in 1 Extracts PDFteeNo ratings yet
- What Is The Definition of InsomniaDocument24 pagesWhat Is The Definition of InsomniaHaniv Prasetya AdhiNo ratings yet
- Dwnload Full Cardiovascular and Pulmonary Physical Therapy Evidence To Practice 5th Edition Frownfelter Test Bank PDFDocument36 pagesDwnload Full Cardiovascular and Pulmonary Physical Therapy Evidence To Practice 5th Edition Frownfelter Test Bank PDFphysetergrannam.devtjz100% (20)
- Home Vent GuideDocument27 pagesHome Vent GuideIsmael Pérez RuizNo ratings yet
- Chapter 23 Respiratory System - Study GuideDocument5 pagesChapter 23 Respiratory System - Study GuideGretchenNo ratings yet
- Breathing and Exchange of GasesDocument10 pagesBreathing and Exchange of GasesAnonymous 9uu04elNo ratings yet
- Respiratory System: Gas ExchangeDocument35 pagesRespiratory System: Gas ExchangeQuenie Balanay AgaNo ratings yet
- Anatomy and PhysiologyDocument6 pagesAnatomy and PhysiologyPau-pau BasiNo ratings yet
- Grade 7 WorksheetDocument5 pagesGrade 7 Worksheetsunitak115No ratings yet
- Biology 8 Frog Dissection GuideDocument10 pagesBiology 8 Frog Dissection GuideRyan SantosNo ratings yet
- Animal TissueDocument32 pagesAnimal TissueIan Kerby Sollano100% (1)
- Presentation Without MusicDocument17 pagesPresentation Without Musicapi-237180804No ratings yet
- Hematopoietic SystemDocument47 pagesHematopoietic SystemAbbi Yanto ArtNo ratings yet
- Part B-13-Night Shift SleepDocument4 pagesPart B-13-Night Shift Sleepfernanda1rondelliNo ratings yet
- 1st MINI TESTDocument8 pages1st MINI TESTTín TháiNo ratings yet
- Chapter 1: Introduction To Anatomy and Physiology NotesDocument6 pagesChapter 1: Introduction To Anatomy and Physiology Notesapi-305436791No ratings yet
- Squid Lab DissectionDocument41 pagesSquid Lab DissectionMarie Claire AquilinaNo ratings yet
- 1 The Effects of Sleep DeprivationDocument15 pages1 The Effects of Sleep DeprivationShenel OrtegaNo ratings yet
- Silverman Anderson IndexDocument2 pagesSilverman Anderson IndexMark Jaco AngNo ratings yet
- Mindmap Digestive AnatomyDocument2 pagesMindmap Digestive Anatomyapi-535582646No ratings yet
- Thermoregulation: Biology Bilingual Education 2013Document32 pagesThermoregulation: Biology Bilingual Education 2013rahmaNo ratings yet
- Neuro Study GuideDocument11 pagesNeuro Study GuideEllen Hennings100% (1)