Professional Documents
Culture Documents
Supplementation With Folic Acid During Methotrexate Therapy For Rheumatoid Arthritis
Supplementation With Folic Acid During Methotrexate Therapy For Rheumatoid Arthritis
Uploaded by
Genshin SatuOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Supplementation With Folic Acid During Methotrexate Therapy For Rheumatoid Arthritis
Supplementation With Folic Acid During Methotrexate Therapy For Rheumatoid Arthritis
Uploaded by
Genshin SatuCopyright:
Available Formats
Supplementation with Folic Acid during Methotrexate
Therapy for Rheumatoid Arthritis
A Double-Blind, Placebo-controlled Trial
Sarah L. Morgan, MD, RD; Joseph E. Baggott, PhD; William H. Vaughn, BS; Janet S. Austin, MA;
Tonya A. Veitch, BS; Jeannette Y. Lee, PhD; William J. Koopman, MD;
Carlos L. Krumdieck, MD, PhD; and Graciela S. Alarcon, MD, MPH
• Objective: To determine the effect of two different 1 he folic acid antagonist methotrexate (N-10-methyl-ami-
weekly doses of folic acid on the toxicity and efficacy of nopterin) is useful in low doses (2.5 to 20 mg/wk) for
low-dose methotrexate therapy for rheumatoid arthritis. treating chronic inflammatory diseases (1-7). Many trials
• Design: Randomized, double-blind, placebo- have established the efficacy of methotrexate in rheuma-
controlled study. toid arthritis (7-13). Compared with other disease-modi-
• Patients: 79 persons between 19 and 78 years of fying drugs, methotrexate has the highest probability of
age who fulfilled the American Rheumatism Associa- drug continuation at 10 years. Dose response-related
tion's criteria for rheumatoid arthritis. toxic effects have been reported in 30% to 90% of pa-
• Intervention: Participants were randomly assigned tients given methotrexate (13). Toxic effects include gas-
to visually identical placebo or to 5 mg or 27.5 mg of trointestinal intolerance, hematologic abnormalities, alo-
folic acid each week. pecia, hepatotoxicity, and pulmonary toxicity (14-22).
• Measurements: Duration, intensity, and clinical se- Some side effects of methotrexate administration, such
verity of toxic events; efficacy (indices of joint tender- as gastrointestinal intolerance, mimic complicated folate
ness and swelling and grip strength); plasma and eryth- deficiency (23). Folate deficiency occurs frequently in pa-
rocyte folate levels; and other laboratory variables. tients with rheumatoid arthritis; further, folate stores are
• Results: Folic acid supplementation at either dose decreased in patients with rheumatoid arthritis who take
did not affect the efficacy of methotrexate therapy as methotrexate, suggesting that impaired folate status is
judged by joint indices and patient and physician as- related to toxicity (24-26).
sessments of disease. Patients given folic acid supple- Folic acid supplementation has been reported anecdot-
ments had lower toxicity scores than did participants ally to lessen toxicity in patients receiving methotrexate
given placebo (P < 0.001). Low blood folate levels and treatment (27, 28). In a 6-month, double-blind, placebo-
increased mean corpuscular volumes were associated controlled trial, 7 mg of folic acid weekly (1 mg/d or 2265
with substantial methotrexate toxicity, whereas daily nmol/d) decreased methotrexate toxicity without affecting
dietary intakes of more than 900 nmol (400 fig) of folic efficacy (29). This was confirmed by Stewart and col-
acid were associated with little methotrexate toxicity. leagues (30) in a retrospective chart review.
• Conclusions: Folic acid, an inexpensive vitamin, is Folinic acid (leucovorin, citrovorum factor) is a one-
safe in a broad range of doses and protects patients carbon-substituted, fully reduced folate that has also been
with rheumatoid arthritis who are taking methotrexate administered during methotrexate therapy (31-36). Low
from toxicity while preserving the efficacy of methotrex- doses of the vitamin (1 to 7 mg/wk) have decreased
ate. methotrexate toxicity (35, 36). Higher doses negate effi-
cacy and lessen toxicity (31, 32). Thus, the folinic acid
dose may critically affect the efficacy of methotrexate ther-
apy.
The influence of the folic acid dose on methotrexate
toxicity and efficacy remains controversial, and the effects
of different doses of folic acid are not known (37, 38).
Some investigators argue that if toxic effects occur, the
most rational approach is to reduce the dose of metho-
trexate rather than to provide folic acid supplements (37).
We designed a larger and longer study to evaluate differ-
ent doses of folic acid, assuming that toxicity could be
reduced without changing the efficacy of methotrexate.
Ann Intern Med. 1994;121:833-841. Methods
Participants
From the Birmingham Veteran's Administration Hospital and
the University of Alabama at Birmingham, Birmingham, Ala- Patients aged 19 to 78 years who fulfilled the American Col-
bama. For current author addresses, see end of text. lege of Rheumatology's revised criteria for rheumatoid arthritis
© 1994 American College of Physicians 833
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
consented to participate in the trial (39). Enrollment criteria daily living assessed and averaged at baseline and at 12 months
included rheumatoid arthritis diagnosed more than 6 months using the modified Health Assessment Questionnaire and scored
previously, onset after the age of 16 years, and at least three of on a scale of 1 (no difficulty) to 4 (unable to perform) (42); and
the following signs or symptoms: 3 or more swollen joints, 6 or 10) presence, duration, intensity, and severity of toxic effects at
more tender joints, at least 45 minutes of morning stiffness, and every follow-up visit and every 3 weeks by telephone interview
a Westergren erythrocyte sedimentation rate greater than or (done by SLM).
equal to 28 mm/h.
Referring rheumatologists and the principal investigator did Laboratory Assessments
the screening. Exclusion criteria included serious concomitant
medical illnesses, liver enzyme levels twice the upper limit of At the initial visit, complete blood cell count, Westergren
normal, leukocyte counts less than 3.5 X 109/L or platelet counts erythrocyte sedimentation rate, liver enzyme (aspartate amino
less than 150 X 109/L, and use of methotrexate within the past 6 transferase and alkaline phosphatase), rheumatoid factor by
months. Gold salts were stopped for at least 10 days before the nephelometry, and serum creatinine values were obtained. The
trial. This short washout period mirrors actual rheumatology complete blood cell count, creatinine, and liver function tests
practice. Patients remained under the care of their rheumatolo- were repeated at all visits. If laboratory values were obtained
gists, abstained from alcohol use, did not become pregnant, and more frequently than stipulated in the protocol, they were re-
received stable doses of aspirin and nonsteroidal anti-inflamma- corded and became part of the toxicity score.
tory drugs. If prednisone was taken at entry, the dose could not Blood for plasma and erythrocyte folate levels, using a meth-
exceed 10 mg/d. Hydroxychloroquine therapy was allowed during otrexate-resistant Lactobacillus casei microbiological assay, was
the study. drawn at all visits (43). At baseline, blood was drawn for a
vitamin panel (plasma and erythrocyte folate, vitamins B 12 , A, C,
and E, carotene, riboflavin, thiamin, pyridoxine) (44-51). If pa-
Study Design tients had abnormal values for any of the vitamins, other than
Figure 1 shows the trial design. To maintain the double-blind folate, the abnormality was treated with single vitamin supple-
status of the trial, the statistician carried out the randomization ments.
using a computer program in which the algorithm was transpar-
ent and a coded vial number represented the treatment assign- Radiographic Assessment
ment. Patients were assigned to treatment groups by a sequential Hand and wrist radiographs taken within 6 months of entering
treatment assignment process designed to balance the sample the trial were assessed by one of the rheumatologists (GSA)
with respect to baseline features, including age, sex, folate-con- without knowledge of study status. Joint erosions and space
taining vitamin use, rheumatoid factor status, and prednisone use narrowing were determined by the modified method of Sharp
(40). Patients agreed to discontinue therapy with folate-contain- (52). Results were expressed as the mean raw scores for joint
ing vitamins during the trial. Rheumatoid factor was considered erosion and joint space narrowing.
positive if the level was more than 30 IU/mL or if the titer was
more than 1:160. Patients received either visually identical pla- Toxicity: Frequency and Severity
cebo or 5 mg (low-dose folic acid group) or 27.5 mg folic acid
(high-dose folic acid group) each week, prepared by the Hospital Toxic effects and discontinuation of therapy with study medi-
Investigational Drug Service. Spectrophotometric analysis indi- cations due to toxicity were considered primary outcomes. We
cated that the mean ± SD folic acid content was 1 ±0.15 mg determined a toxicity score, modified from the one previously
(2.3 ± 0.3 jLtmol) and 5.5 ± 0.3 mg (12.5 ± 0.7 /Ltmol) per capsule used, for each patient at each visit or until methotrexate therapy
in the low-dose and high-dose folic acid groups, respectively. was discontinued (29) (Appendix).
Lederle Laboratories provided the methotrexate (Rheumatrex;
Pearl River, New York), which was started in a median oral dose Efficacy
of 16.5 jLtmol (7.5 mg) per week and increased in 5.5-/xmol (2.5
mg) increments at the rheumatologist's discretion. Methotrexate We determined patient response to treatment using a modifi-
was taken either in an undivided or a divided dose (that is, every cation of the criteria used in our previous folic acid supplemen-
12 hours for three doses). The methotrexate dosing regimens tation trial and by others (8, 29, 53). We defined marked im-
were identical among the study groups. Folic acid supplements provement in the joint swelling index and the joint tenderness
were given 5 days per week when methotrexate was not ingested. and pain index as a net decrease of 50% or more in value at any
Compliance with the regimen was reinforced using a digital re-
minder cap (Counter Cap; Senetics, Boulder, Colorado). All
participants and investigators were blinded to vitamin capsule
content until the study was complete.
Clinical Assessment
Patients were evaluated immediately before methotrexate ini-
tiation at a mean of 13, 26, 39, and 53 weeks (Figure 1). Each
patient was assessed by the same physician-nutritionist (SLM).
Two research assistants (JSA or WHV) did the joint evaluations.
In most cases, patients were examined by the same observer
throughout the study. The joint counts for tenderness and swell-
ing were not significantly different between the two observers
(P = 0.6 for tenderness; P = 0.9 for swelling). The following vari-
ables were evaluated at each visit: 1) number of the 58 diarth-
rodial joints with swelling; 2) number of the 60 joints with
tenderness on pressure or with pain on passive motion (or both);
3) joint swelling and tenderness indices, expressed as a sum, with
each joint graded for swelling as 0 (none), 1 (mild), 2 (moder-
ate), or 3 (severe); 4) mean grip strength (three measurements)
for both hands expressed in mm Hg; 5) duration of morning
stiffness expressed in hours; 6) patient's and physician's global
assessments of disease activity graded as 0 (asymptomatic), 1 Figure 1. Study design for the double-blind, placebo-controlled
(mild), 2 (moderate), 3 (severe), or 4 (very severe); 7) current trial. The randomization was done by the statistician using a
medications and doses; 8) a 1-day dietary recall using the Min- sequential treatment assignment program in which the algorithm
nesota Nutrition Data System software, Food Database version was transparent and a coded vial number was used as the treat-
6A, Nutrient Database version F21 (41); 9) eight activities of ment assignment.
834 1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
follow-up visit compared with visit 1. We defined moderate im- and analysis of variance to evaluate the effects of treatment,
provement as a 30% to 49% net decrease in the index, and no time, and their interaction.
change as the index value remaining within 30% of the original Non-normal distributions occurred in joint indices for pain and
value. We defined worsening as an increase in the index value of tenderness, physician and patient assessment of disease, grip
30% or more. strength, answers to the modified Health Assessment Question-
We examined the effects of folic acid supplementation on naire, and plasma and erythrocyte folate levels. We used the
changes in physician and patient global assessments, grip Wilcoxon rank-sum test to compare the three groups and Wil-
strength, morning stiffness, erythrocyte sedimentation rate, find- coxon rank-sum tests for pair-wise comparison, if appropriate.
ings of the modified Health Assessment Questionnaire, complete
blood cell counts, blood folate levels, and dietary folate and Comparison of Toxicity Scores
vitamin B 12 intake.
We used the Fisher exact test to compare the incidence of
Statistical Analysis toxic effects in the folic acid and placebo groups. Because the
Sample Size and Analysis primary outcome measure was the toxicity score, we included
data until the study was complete or the participant withdrew. To
In our previous study, the mean toxicity scores for patients evaluate the effects of time, treatment group, and their interac-
receiving low-dose folic acid and placebo recipients were 0.21 tion on the toxicity score, we used analysis of variance on the
and 1.06, respectively, for a difference of 0.85. The sample size rank of the toxicity scores. We did two-way analyses of variance
tested the null hypothesis for no difference between placebo and (or on the ranks for data that were non-normally distributed) to
low- and high-dose folic acid treatments, with respect to the evaluate the effects of time, treatment, and their interaction.
mean toxicity score. The alternative hypothesis was that the
difference in the score between at least one pair of treatments
(placebo compared with low-dose folic acid, placebo compared
with high-dose folic acid, or low-dose folic acid compared with Results
high-dose folic acid) was greater than or equal to the difference
observed previously. As described by Cohen (54) and imple- Patients
mented by Borenstein and Cohen (55), 25 patients per group was
a sufficient number to detect a difference in the mean toxicity W e enrolled 94 patients (age range, 19 to 78 years) into
score of 0.85 between any pair of treatments at a significance the trial. Subsequently, we withdrew 15 patients because
level of 0.05 and a power of 0.80. of noncompliance (numbers were equally distributed
An underlying assumption in sample size estimates was that among the study groups). O u r results are from 79 patients
the scores are normally distributed. To address the potential
non-normal character of the toxicity scores, we increased the who completed the trial: 25 in the low-dose folic acid
sample size estimates by 4% to maintain the significance level group, 26 in the high-dose folic acid group, and 28 in the
and power if nonparametric analyses were used. To allow for a placebo group. T h e demographic and selected clinical
20% attrition rate, the enrollment goal was 31 patients per features of the patients in the three study groups were
group.
similar (Table 1). N o patients were taking sulfasalazine
Patients vvere withdrawn if more than 3 weeks of methotrexate
treatment was missed for any reason or if noncompliance was before enrollment. W e found no statistical difference
documented. Patients who withdrew from the trial because of a m o n g the groups in previous use of gold salts (P = 0.92).
toxic effects did so after consulting their rheumatologists. Pa- Four patients in the placebo group (23%), 4 in the low-
tients contributed to data analyses until therapy with methotrex- dose folic acid group (14.3%), and 6 in the high-dose folic
ate was discontinued. For patients who withdrew before receiving
12 months of therapy, we computed toxicity and efficacy data acid group (23%) previously had therapy with methotrex-
based on data collected until drug therapy was discontinued. ate discontinued because of toxic effects (P = 0.76). Pa-
tients who previously discontinued methotrexate therapy
Comparison of Data among Groups because of toxic effects were randomly distributed in the
three groups. O t h e r initial variables such as hemoglobin
We tested the baseline values of all outcome measures for
normality using the Shepin-Wilk statistic. For normally distrib- level, hematocrit, leukocyte count, m e a n corpuscular vol-
uted data, we used chi-square analyses to compare proportions u m e , creatinine level, aspartate aminotransferase value,
Table 1. Demographic and Selected Clinical Characteristics of 79 Patients with Rheumatoid Arthritis*
Characteristics Study Group
Placebo Low-Dose Folic Acid High-Dose Folic Acid
(n = 28) (n = 25) (n = 26)
Mean age, y 52.2 ± 13.0 54.4 ± 14.0 53.2 ± 14.3
Sex, % women 82 76 65
Race, % white 85.7 68 73
Mean disease duration, y 8.5 ± 8.2 7.4 ± 10 11.6 ± 9.5
Previous use of folate-containing vitamins, % 32 28 19
IgM rheumatoid factor positivity (>30 IU/mL or 1:160 titer), % 71 80 85
Concurrent use of aspirin or nonsteroidal anti-inflammatory
drugs, % 86 80 88
Concurrent prednisone use, % 79 80 88
Concurrent hydroxychloroquine use, n 1 1 4
Patients previously receiving gold salts, n 16 17 17
Patients previously receiving methotrexate, n 4 6 4
Previous disease-modifying antirheumatic drug use, % 64 68 77
Mean joint erosion score 9.2 ± 9.5 15 ± 16.7 17.7 ± 17.8
Mean joint space narrowing 20.2 ± 20.1 29.1 ± 25.1 35.3 ± 31.1
* All comparisons between groups, P > 0.05. Means are expressed ± SD.
1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11 835
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
Methotrexate Dose: Folate and B 1 2 Intake
We found no statistical differences in mean cumulative
methotrexate dose among the three groups. The mean
cumulative methotrexate doses at 53 weeks in the pla-
cebo, low-dose folic acid, and high-dose folic acid groups
were 206 ± 88 mg, 217 ± 113 mg, and 284 ± 187 mg,
respectively (P = 0.24). The average weekly methotrexate
dose was 8.5 ± 1 . 5 mg, 9.4 ± 2.4 mg, and 9.6 ± 2.6 mg in
the placebo, low-dose folic acid, and high-dose folic acid
groups, respectively (P = 0.27).
The mean dietary folate and vitamin B 1 2 intakes among
the groups were never statistically different. Median di-
etary folate intakes were 204 /xg/d in the placebo group,
195 jmg/d in the low-dose folic acid group, and 230 ju,g/d in
the high-dose folic acid group (P = 0.37 for all compar-
isons). The median daily intakes in all study groups did
not substantially differ from the median values of 150 to
250 jmg/d reported in the Second National Health and
Nutrition Examination series (56).
Primary Outcome: Toxic Effects
Fifty-four patients (68%) experienced some form of
toxicity: 25 (89%) in the placebo group, 12 (48%) in the
low-dose folic acid group (P < 0.002 compared with pla-
cebo), and 17 (65%) in the high-dose folic acid group.
Figure 2 shows the median toxicity score for the three
groups (0.685, 0.016, and 0.031 in the placebo, low-dose
folic acid, and high-dose folic acid groups, respectively).
The toxicity score for the placebo group was greater than
Figure 2. Median toxicity scores in the three study groups. The
placebo group had a statistically higher toxicity score (P = 0.001)
those for the two folic acid-supplemented groups (P =
than the folic acid supplementation groups. The toxicity score 0.001 for both comparisons for low-dose folic acid and
was not significantly different between the low-dose folic acid and high-dose folic acid compared with placebo; P - 0.71 for
high-dose folic acid groups (P = 0.71). A = patients withdrawn low-dose folic acid compared with high-dose folic acid).
from the trial because of toxic effects; O = patients who com- The most frequently reported toxicities were nausea and
pleted the trial.
indigestion (31 patients), diarrhea (11 patients), stomatitis
(9 patients), and rash (9 patients). When the patients
receiving hydroxychloroquine were omitted from the anal-
alkaline phosphatase level, and erythrocyte sedimentation yses, the results were identical.
rate were also similar among the groups. The erosion and
Other Outcomes
joint space narrowing scores were similar at baseline
among the three groups (P = 0.16 for joint space narrow- Efficacy
ing and P = 0.17 for erosions; Table 1). As noted in Table 2, the percentages of patients who
Table 2. Joint Swelling and Tenderness at 6 and 12 Months in the Three Treatment Groups
Outcome 6 Months 12 Months
Placebo Low-Dose Folic High-Dose Folic Placebo Low-Dose Folic High-Dose Folic
(n = 23) Acid (" = 24) Acic (" = 23) (n = 19) Acid (" = 23) Acid (n = 18)
n?_
< /u
Marked improvement
Swelling 35 38 61 68 78 78
Tenderness 30 29 39 53 43 61
Moderate improvement
Swelling 26 29 26 16 13 5
Tenderness 35 8 18 16 13 16
No change
Swelling 35 33 9 11 5 17
Tenderness 26 55 39 21 35 17
Worsening
Swelling 4 0 4 5 4 0
Tenderness 9 8 4 10 9 6
* P > 0.5 (chi-square) for comparisons among groups at 6 months and 12 months.
836 1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
Table 3. Data for Efficacy and Other Outcomes at Baseline, 6 Months, and 12 Months*
Outcome Placebo Group Low-Dose Folic Acid Group High-Dose Folic Ac id Group
Baseline 6 Months 12 months Baseline 6 Months 12 months Baseline 6 Months 12 months
Joint indices for tendernesst 34 21 18 32 20 21 34 26 14
(2, 99) (0, 61) (4, 62) (6, 112) (2, 99) (0, 90) (2, 105) (0, 66) (2, 41)
Joint indices for swelling! 45 25 12 51 28 14 43 20 13
(6, 85) (3, 51) (0, 51) (14, 85) (2, 48) (2, 40) (18, 103) (4, 62) (1, 58)
Patient assessment of disease
activity! 3 2 2 3 2 2 3 2 2
(2,5) (1,4) (2,4) (2,5) (1,5) (1,5) (2,5) (1,4) (1,4)
Physician assessment of disease
activity! 4 3 2 4 3 2 4 3 2
(2,4) (2,4) (2,4) (2,5) (2,4) (2,3) (2,5) (2,5) (2,4)
Grip strength in right hand,
mm Hg"\ 56.5 66.7 61.7 40.5 45 48.3 35 53.3 46.7
(5, 100) (10, 205) (9.3, 167) (0, 173) (13, 127) (18.3, 133) (5, 132) (5, 180) (8.3, 118)
Grip strength in left hand,
mm Hgf 46.7 56.7 56.7 40 34.2 48.3 32.5 30 48.3
(4.3, 208) (10, 223) (10.7, 150) (5, 243) (5, 115) (10, 152) (1.3, 183) (6.7, 190) (10, 157)
Modified Health Assessment
Questionnaire 1.8 1.5 2 1.2 2 1.2
(1, 3.4) (1, 2.8) (1, 3.8) (1, 2.8) (1.1, 3.4) (1, 2.6)
* Median (minimum, maximum).
! P < 0.05 for time effects for the three treatment groups.
had marked improvement, moderate improvement, no im- volume of 100 fL or more at one or more follow-up visits
provement, or worsening were similar among the three compared with only one and none in the low-dose or
groups (P > 0.5). We observed marked improvement in high-dose folic acid groups, respectively (P = 0.02).
the pain and tenderness index after 12 months in 53%, Mean baseline plasma folate levels were 15, 10, and
43%, and 61% of patients receiving placebo, low doses of 13.5 nmol/mL (P > 0.1), and mean baseline erythrocyte
folic acid, and high doses of folic acid, respectively. We folate levels were 662, 591, and 624 nmol (P > 0.1) in the
found marked improvement in the swelling index in 68%, placebo, low-dose folic acid, and high-dose folic acid
78%, and 78% of patients receiving placebo, low doses of groups, respectively. After 1 year, mean plasma folate
folic acid, and high doses of folic acid, respectively. levels in the placebo group decreased to 4.8 nmol/mL
(P < 0.01) and mean plasma folate levels increased four
Patient Withdrawal and Dropout to five times from baseline values in the folic acid groups
(P < 0.001). In contrast, mean erythrocyte folate levels in
We withdrew 13 patients because of noncompliance.
the low-dose and high-dose folic acid groups were little
One patient was withdrawn for taking additional folate
changed (± 5%) from baseline values after 1 year,
supplements and one because diagnosis was reconsidered.
whereas levels in the placebo group decreased by approx-
Seven patients in the placebo group, 2 in the low-dose
imately 50% (349 nmol/mL; P < 0.001 for baseline values
folic acid group, and 2 in the high-dose folic acid group
compared with values at 1 year). Twelve (43%), 5 (20%),
discontinued methotrexate treatment because of toxic ef-
and 4 (15%) patients in the placebo, low-dose folic acid,
fects. More dropouts occurred in the placebo group
(25%) than in the folic acid groups (8%) (P = 0.08).
Other Indices
As noted in Table 3, patient and physician assessment,
joint indices for swelling and tenderness, and grip
strength improved with time. We found significant time
effects with respect to joint tenderness indices (P =
0.025), joint swelling indices (P = 0.027), physician assess-
ment of disease (P = 0.011), patient assessment of disease
(P= 0.008), right-hand grip strength (P = 0.032), and
left-hand grip strength (P = 0.047). We observed no sig-
nificant time-treatment interactions.
At the follow-up visits, changes in the median or mean
values for the following variables were not statistically
different among the groups: modified Health Assessment
Questionnaire, erythrocyte sedimentation rate, hemoglo-
bin level, hematocrit, leukocyte count, mean corpuscular
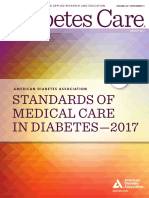
Figure 3. Toxicity score as a function of dietary folate intake in
volume, creatinine concentration, and aspartate amino- the placebo group. An exponential decay curve was fitted to the
transferase or alkaline phosphatase levels. However, six of data. To convert micrograms to nanomoles, divide micrograms by
the patients in the placebo group had a mean corpuscular 0.441 (the formula weight of folic acid is 441.4).
1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11 837
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
and high-dose folic acid groups, respectively, had eryth- on the data presented, baseline mean corpuscular volume,
rocyte folate levels less than 320 nmol/L (that is, <140 blood folate, and vitamin B, 2 values should be deter-
ng/mL) at one or more of the follow-up visits (P = 0.02). mined in patients in whom methotrexate will be initiated.
Figure 3 shows the toxicity score in the placebo group Because anemia is a late finding in nutritional deficien-
plotted as a function of mean daily dietary folate intake. cies, and patients may have dimorphic anemia (iron plus
Negligible toxic effects occurred as the dietary folate in- B 12 or folate deficiency), yielding a normal mean corpus-
take was increased to more than 900 nmol/d (400 jLtg/d). cular volume, we think vitamin levels are useful. There is
We used a multivariate general linear model to evaluate no contraindication to starting folic acid at a dose of 5 to
the effects of the following factors on the toxicity score: 7 mg/wk during methotrexate therapy initiation. Supple-
sex, race, disease duration, previous folate-containing vi- mentation with higher doses may be indicated if an in-
tamin use, rheumatoid factor status, concurrent nonste- creasing mean corpuscular volume is observed or if sus-
roidal anti-inflammatory drug use, concurrent prednisone pected methotrexate toxic effects occur. The dose may be
use, previous disease-modifying antirheumatic drug use, adjusted to levels as high as 27.5 mg/wk to control or
dietary folate intake, and supplemental folate intake (pla- reverse both of these clinical findings. Serial evaluation of
cebo; 5 mg/wk; and 27.5 mg/wk). Because the toxicity the mean corpuscular volume has been suggested as an
score and dietary folate intake measurements were not inexpensive means to monitor incipient toxicity (60).
normally distributed, we used their ranks in the analysis. However, other investigators have found that the mean
The analysis indicated that dietary folate intake and sup- corpuscular volume does not predict toxicity in patients
plemental folate intake were related to toxicity (P = 0.016 given folic acid (30). Our data suggest that a high mean
for dietary intake; P = 0.016 for supplemental folate in- corpuscular volume and a low blood folate level are often
take). Dietary folate was negatively correlated with toxic- associated with methotrexate toxicity.
ity score, indicating that higher dietary folate intake re- The mechanism or mechanisms by which folate pro-
duced toxicity. With regard to supplemental folate intake, duces the clinical effects on toxicity are not clear. Folinic
both the 5 mg and 27.5 mg/wk doses reduced toxicity acid, 5-formyl-tetrahydrofolic acid, also has been used to
compared with placebo, suggesting an ameliorative effect. reduce side effects of methotrexate (31-36). Perhaps folic
No interaction occurred between the dietary and supple- acid and folinic acid correct a state of folate deficiency, or
mental folate intakes (P = 0.39). perhaps folinic acid, by circumventing dihydrofolate re-
ductase inhibition, relieves toxicity. However, these two
mechanisms are not mutually exclusive.
Discussion
The vitamin form and ratio of folate to methotrexate
This controlled trial shows that folic acid supplementa- are important factors in determining whether efficacy will
tion of 11 327 nmol (5 mg) or 62 302 nmol (27.5 mg) per be lost with combination vitamin and antivitamin therapy.
week decreases methotrexate toxicity without compromis- Because folinic acid is a fully reduced and one-carbon-
ing efficacy. The toxicity of methotrexate in both folic acid substituted folate, it can bypass folate-metabolizing steps
groups was low and nearly identical. The data suggest that that reduce the pteridine moiety and add a one-carbon
dietary folate also helps protect against methotrexate tox- fragment. Table 4 shows the ratios of folate to metho-
icity. This finding suggests that the intake of one multiple- trexate and clinical outcomes in previous studies. Folinic
vitamin pill containing 900 nmol of folic acid (400 jLig/d) acid in relatively high doses negates the effectiveness of
may also modulate methotrexate toxicity in patients with methotrexate therapy for rheumatoid arthritis (31). Our
other micronutrient deficiencies (57). previous trial used a folic acid-to-methotrexate ratio of
We designed this trial using completers analysis. One 0.93 to 1, causing decreased toxicity but not decreased
year into the study, we considered modifying the trial efficacy (29). Similar results are now reported with a ratio
toward intention-to-treat analysis. However, we could not as high as 2.85 to 1. The participants who received 27.5
have obtained complete data on the participants who had mg/wk had a folate-to-methotrexate ratio that was much
already withdrawn in the first year. We wanted to com- higher than in the folinic acid studies by Joyce and col-
pare our study with other methotrexate clinical trials that leagues and Tishler and colleagues (31, 32), in which
used completers analyses and thus chose not to analyze efficacy was negated. A study by Duhra (61) using 35 mg
the data by intent to treat. The overall results of the study of folic acid per week during methotrexate therapy for
were not greatly influenced by the study design. By using psoriasis showed no loss of efficacy and supports a wide
intent-to-treat analysis, we might have observed a lesser margin of safety for folic acid. Although folinic acid can
degree of difference for efficacy, but we would have ob- lessen methotrexate toxicity, the dose level is more critical
served the same toxic effects and resulting discontinuation than that for folic acid.
of drug therapy. The optimal dosing schedule of folate supplements in
We also re-examined the data on the basis of the most relation to methotrexate is not known. The half-life for
recent recommendations from the American College of oral, intramuscular, and intravenous low-dose methotrex-
Rheumatology for monitoring hepatic conditions in pa- ate is about 4.5 to 13 hours (62-65). Table 4 shows the
tients with rheumatoid arthritis who are receiving meth- timing of the folate to methotrexate in previously pub-
otrexate, but this did not change the toxicity scores (58). lished reports. In the studies by Joyce and associates (31),
We previously showed that low baseline plasma and Tishler and coworkers (32), and Buckley and colleagues
erythrocyte folate levels can predict future toxicity (29). (34), folinic acid was given within the first half-life of the
Because large doses of folic acid can mask and exacerbate methotrexate dose. The ratio of folate to methotrexate
vitamin B 1 2 deficiency, adequate vitamin B 1 2 status should used by these three investigators was 2.3, 0.95, and 0.5,
be assured before folic acid supplementation (59). Based respectively, with the lowest ratio causing no flare in
838 1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
Table 4. Ratios of Folic Acid to Methotrexate and Folinic Acid to Methotrexate and Effects on Clinical Efficacy*
Reference Weekly Folate-to- Effect on Efficacy in Timing of Folate Relative to
Methotrexate Ratio Rheumatoid Arthritis Methotrexate Dose
Folinic acidf
31 2.3 : 1 Flare in disease activity Oral folinic acid 2 hours after weekly oral
methotrexate dose
32 0.95 : 1 Flare in disease activity 15 mg oral folinic acid for 3 consecutive days,
starting 4 to 6 hours after intravenous meth-
otrexate dose
33 0.5:1 No adverse effect on disease activity Folinic acid orally for 2 days, beginning 4 days
before next intramuscular methotrexate dose
34 0.5 : 1 No adverse effect on disease activity Oral folinic acid 4 hours after oral methotrex-
ate dose
35 0.09 : 1 No change in efficacy—one patient in Oral folinic acid 24 hours after oral metho-
folinic acid arm for lack of efficacy trexate dose
36 0.05 : 1 No change in efficacy Oral folinic acid given simultaneously with oral
methotrexate dose
Folic acid
29 0.93 : 1 No change in efficacy Not specified
30 1: 1 No change in efficacy Not specified
This trial 0.53 : 1 and 2.85 : 1 No change in efficacy Folic acid administered on 2 days when oral
methotrexate not taken
* Folic acid = Pteroylglutamic acid; folinic acid = 5-Formyl-tetrahydro-pteroylglutamic acid.
t Only one half of the folinic acid dose is biologically active because of the presence of stereoisomers.
disease activity. In contrast, when the two highest ratios severity factor is 1 (alopecia, malaise or fatigue, nausea,
were administered, a flare in disease activity occurred, pruritus, anorexia, or general gastrointestinal intolerance
which suggests that the ratio of folate to methotrexate, [pyrosis, cramps, and so on]), 2 (vomiting, diarrhea, sto-
not the dosing interval, was more important in determin- matitis, rash, headache, elevated liver enzyme levels, pe-
ing whether efficacy is altered. ripheral nodulosis), 3 (elevated serum creatinine level), or
The cost of folinic acid compared with that of folic acid 4 (cytopenias, documented infections, or pulmonary tox-
therapy is also relevant (36). At our center, the price of a icity, systemic nodulosis, profound lethargy). Any abnor-
dose of folinic acid is 43 times greater than the price of mality in liver functions or complete blood cell count,
an equivalent dose of folic acid; these figures are probably documented infection, or pulmonary toxicity was given an
similar to costs nationwide. Thus, safety and cost would intensity score of 3 (severe). Abnormal liver function tests
support folic acid as the better supplement. A controlled were defined as an aspartate aminotransferase or an al-
trial of folic acid and folinic acid would answer these kaline phosphatase level greater than two times baseline;
questions most clearly. cytopenias were defined as a leukocyte count less than 3.5
The proposal to enrich flour with folic acid to prevent X 109/L or a platelet count less than 150 X 109/L; and
neural tube defects has led to concern about the possi- serum creatinine concentration was considered elevated if
bility of negating the efficacy of methotrexate therapy in more than 133 /xmol/L (1.5 mg/dL). Pulmonary toxicity
autoimmune diseases (66, 67). Neither our data nor the was defined as evidence of new interstitial pulmonary
data of others support this concern (61). Enrichment of infiltrates from baseline chest radiograph and evidence of
flour to provide folic acid intakes of 900 to 2265 nmol restrictive changes in pulmonary function tests, including
(400 jLtg to 1 mg/d) would not affect efficacy of low-dose vital capacity less than 80% of predicted value, normal
methotrexate therapy for rheumatic disease. expiratory flow rates, normal maximal voluntary ventila-
The enzyme or enzymes that must be inhibited to allow tion, and carbon monoxide diffusion capacity less than
for the efficacy of methotrexate therapy is not known. We 70% of normal. Infection was defined as a documented
have postulated that inhibition of aminoimidazole carbox- viral, bacterial, or fungal infection that compromised the
amide ribotide transformylase is necessary for the efficacy patient greatly and required hospitalization or administra-
of methotrexate therapy (68). tion of systemic antimicrobial agents, or both.
Widely varying dose levels of folic acid decrease the
Acknowledgments: The authors thank their patient volunteers and their
toxicity of methotrexate without affecting its efficacy. The referring rheumatologists (faculty and fellows) for participating in the
flexibility in the dosing range, coupled with its low cost, study and the staffs of the General Clinical Research Center, the Kirklin
make folic acid the preferred vitamin form to treat pa- Clinic, and the University of Alabama at Birmingham Clinical Vitaminol-
ogy Lab for assisting in the investigation.
tients with rheumatoid arthritis who are taking methotrex-
ate. Grant Support: In part by the National Institutes of Health Department of
Research Resources Clinical Research Center grant RR-32-31S1; United
States Public Health Service grants 5P01-CA-28103-10, 5P60-AR-20614,
Appendix and AR-03555; and Veteran's Administration Merit Review Award AR-
03555.
Toxicity score = duration of toxic events [weeks] X (in- Requests for Reprints: Sarah L. Morgan, MD, RD, 212 Webb, Department
tensity) X (clinical severity factor) + weeks in the proto- of Nutrition Sciences, U.A.B. Station, Birmingham, AL 35294-3360.
col, where intensity is 1 (mild), 2 (moderate), or 3 (se- Current Author Addresses: Dr. Morgan: 212 Webb, Department of Nutri-
vere), as gauged by patient report; and the clinical tion Sciences, U.A.B. Station, Birmingham, AL 35294-3360.
1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11 839
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
Dr. Baggott: 340 Webb, Department of Nutrition Sciences, U.A.B. Station, 21. Hargreaves MR, Mowat AG, Benson MK. Acute pneumonitis associ-
Birmingham, AL 35294-3360. ated with low dose methotrexate treatment for rheumatoid arthritis:
Mr. Vaughan: 437 Webb, Department of Nutrition Sciences, U.A.B. Sta- report of five cases and review of published reports. Thorax. 1992;47:
tion, Birmingham, AL 35294-3360. 628-33.
Ms. Austin: CH 19 420, U.A.B. Station, Birmingham, AL 35294-2041. 22. Walker AM, Funch D, Dreyer NA, Tolman KG, Kremer JM, Alarcon
Ms. Veitch: 210 Webb, Department of Nutrition Sciences, U.A.B. Station, GS, et al. Determinants of serious liver disease among patients receiv-
Birmingham, AL 35294-3360. ing low-dose methotrexate for rheumatoid arthritis. Arthritis Rheum.
Dr. Lee: WTI 153, Cancer Center Biostatistics Unit, Division of Hema- 1993;36:329-35.
tology/Oncology, Department of Medicine, U.A.B. Station, Birmingham, 23. Jackson RC. Biological effects of folic acid antagonists with antineo-
AL 35294-3300. plastic activity. Pharmacol Ther. 1984;25:61-82.
Dr. Koopman: 429A THT, Division of Clinical Immunology and Rheuma- 24. Omer A, Mowat AG. Nature of anemia in rheumatoid arthritis. IX.
tology, Department of Medicine, U.A.B. Station, Birmingham, AL 35294- Folate metabolism in patients with rheumatoid arthritis. Ann Rheum
0006. Dis. 1968;27:414-24.
Dr. Krumdieck: 326 Webb, Department of Nutrition Sciences, U.A.B. 25. Morgan SL, Baggott JE, Altz-Smith M. Folate status of rheumatoid
Station, Birmingham, AL 35294-3360. arthritis patients receiving long term, low-dose methotrexate therapy.
Dr. Alarcon: 301 MEB, Division of Clinical Immunology and Rheumatol- Arthritis Rheum. 1987;30:1348-56.
ogy, Department of Medicine, U.A.B. Station, Birmingham, AL 35294- 26. Hine RJ, Alarcon GS, Koopman WJ, Morgan SL, Baggott JE, Clegg
3296. DO, et al. Serum folate (FA) levels of rheumatoid arthritis (RA)
patients treated with methotrexate (MTX) or other disease-modifying
antirheumatic drugs (DMARDs) [Abstract]. Arthritis Rheum. 1990;33:
References S60.
1. Hanno R, Gruber GG, Owen LG, Callen JP. Methotrexate in psoriasis. 27. Wilke WS, Krall PL. Resistant rheumatoid arthritis. What to do when
A brief review of indications, usage, and complications of methotrex- conservative therapy doesn't work. Postgrad Med. 1984;75:69-77.
ate therapy. J Am Acad Dermatol. 1980;2:171-4. 28. Mackenzie AH. Hepatotoxicity of prolonged methotrexate therapy for
2. Mullarkey MF, Blumenstein BA, Andrade WP, Bailey GA, Olason I, rheumatoid arthritis. Cleve Clin Q. 1985;52:129-35.
Wetzel CE. Methotrexate in the treatment of corticosteroid-dependent 29. Morgan SL, Baggott JE, Vaughn WH, Young PK, Austin JV, Krum-
asthma. A double-blind crossover study. N Engl J Med. 1988;318: dieck CL, et al. The effect of folic acid supplementation on the toxicity
603-7. of low-dose methotrexate in patients with rheumatoid arthritis. Arthri-
3. Metzger AL, Bohan A, Goldberg LS, Bluestone R, Pearson CM. Poly- tis Rheum. 1990;33:9-18.
myositis and dermatomyositis: combined methotrexate and corticoste- 30. Stewart KA, Mackenzie AH, Clough JD, Wilke WS. Folate supplemen-
roid therapy. Ann Intern Med. 1974;81:182-9. tation in methotrexate-treated rheumatoid arthritis patients. Semin
4. Owen ET, Cohen ML. Methotrexate in Reiter's disease. Ann Rheum Arthritis Rheum. 1991;20:332-8.
Dis. 1979;38:48-50. 31. Joyce DA, Will RK, Hoffman DM, Laing B, Blackbourn SJ. Exacer-
5. Hoffman GS, Leavitt RY, Kerr GS, Fauci AS. The treatment of bation of rheumatoid arthritis in patients treated with methotrexate
Wegener's granulomatosis with glucocorticoids and methotrexate. Ar- after administration of folinic acid. Ann Rheum Dis. 1991;50:913-4.
thritis Rheum. 1992;35:1322-9. 32. Tishler M, Caspi D, Fishel B, Yaron M. The effects of leucovorin
6. Kozarek RA, Patterson DJ, Gelfand MD, Botoman VA, Ball TJ, Wil- (folinic acid) on methotrexate therapy in rheumatoid arthritis patients.
ske KR. Methotrexate induces clinical and histological remission in Arthritis Rheum. 1988;31:906-8.
patients with refractory inflammatory bowel disease. Ann Intern Med. 33. Hanrahan PS, Russell AS. Concurrent use of folinic acid and meth-
1989;110:353-6. otrexate in rheumatoid arthritis. J Rheumatol. 1988;15:1078-80.
7. Williams HJ, Willkens RF, Samuelson CO Jr, Alarcon GS, Guttadau- 34. Buckley LM, Vacek PM, Cooper SM. Administration of folinic acid
ria M, Yarbobo C, et al. Comparison of low-dose oral pulse metho- after low dose methotrexate in patients with rheumatoid arthritis.
trexate and placebo in the treatment of rheumatoid arthritis. A con- J Rheumatol. 1990;17:1158-61.
trolled clinical trial. Arthritis Rheum. 1985;28:721-30. 35. Shiroky JB, Neville C, Esdaile JM, Choquette D, Zummer M, Hazel-
8. Weinblatt ME, Coblyn JS, Fox DA, Fraser PA, Holdsworth DE, Glass tine M, et al. Low-dose methotrexate with leucovorin (folinic acid) in
DN, et al. Efficacy of low-dose methotrexate in rheumatoid arthritis. the management of rheumatoid arthritis. Results of a randomized,
N Engl J Med. 1985;312:818-22. double-blind, placebo-controlled trial. Arthritis Rheum. 1993;36:795-
9. Andersen PA, West SG, O'Dell JR, Via CS, Claypool RG, Kotzin BL. 803.
Weekly pulse methotrexate in rheumatoid arthritis. Clinical and im- 36. Weinblatt ME, Maier AL, Coblyn JS. Low dose leucovorin does not
munologic effects in a randomized, double-blind study. Ann Intern interfere with the efficacy of methotrexate in rheumatoid arthritis: An
Med. 1985;103:489-96. 8 week randomized placebo controlled trial. J Rheumatol. 1993;20:
10. Thompson RN, Watts C, Edelman J, Esdaile J, Russell AS. A con- 950-2.
trolled two-centre trial of parenteral methotrexate therapy for refrac- 37. Stenger AA, Houtman PM, Bruyn GA. Does folate supplementation
tory rheumatoid arthritis. J Rheumatol. 1984;11:760-3. make sense in patients with rheumatoid arthritis treated with metho-
11. Weinblatt ME, Weissman BN, Holdsworth DE, Fraser PA, Maier AL, trexate? Ann Rheum Dis. 1992;51:1019-20.
Falchuk KR, et al. Long-term prospective study of methotrexate in the 38. Morgan SL, Baggott JE, Koopman WJ, Krumdieck CL, Alarcon GS.
treatment of rheumatoid arthritis. 84-month update. Arthritis Rheum. Folate supplementation and methotrexate [Letter]. Ann Rheum Dis.
1992;35:129-37. 1993;52:315-6.
12. Kremer JM, Phelps CT. Long-term prospective study of the use of 39. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper
methotrexate in the treatment of rheumatoid arthritis. Update after a NS, et al. The American Rheumatism Association 1987 revised criteria
mean of 90 months. Arthritis Rheum. 1991;35:138-45. for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;
13. Furst DE, Koehnke R, Burmeister LF, Kohler J, Cargill I. Increasing 31:315-24.
methotrexate effect with increasing dose in the treatment of resistant 40. Pocock SJ, Simon R. Sequential treatment assignment with balancing
rheumatoid arthritis. J Rheumatol. 1989;16:313-20. of prognostic factors in the controlled clinical trial. Biometrics. 1975;
14. Alarcon GS, Tracy IC, Blackburn WD Jr. Methotrexate in rheumatoid 31:103-15.
arthritis. Toxic effects as the major factor in limiting long-term treat- 41. Schakel SF, Sievert YA, Buzzard IM. Sources of data for developing
ment. Arthritis Rheum. 1989;32:671-6. and maintaining a nutrient database. J Am Diet Assoc. 1988;88:1268-
15. Gispen JG, Alarcon GS, Johnson J J, Acton RT, Barger BO, Koopman 71.
WJ. Toxicity to methotrexate in rheumatoid arthritis. J Rheumatol. 42. Pincus T, Summey JA, Soraci SA Jr, Wallston KA, Kummon NP.
1987;14:74-9. Assessment of patient satisfaction in activities of daily living using a
16. Wolfe F, Cathey MA. The effect of age on methotrexate efficacy and modified Stanford Health Assessment Questionnaire. Arthritis Rheum.
toxicity. J Rheumatol. 1991;18:973-7. 1983;26:1346-53.
17. Furst DE, Erikson N, Clute L, Koehnke R, Burmeister LF, Kohler JA. 43. Tamura T. Microbiological assay of folates. In: Picciano MF, Stokstad
Adverse experience with methotrexate during 176 weeks of a longterm EL, Gregory JF, eds. Folic Acid Metabolism in Health and Disease.
prospective trial in patients with rheumatoid arthritis. J Rheumatol. New York: Wiley-Liss; 1990:121-37.
1990;17:1628-35. 44. Home DW, Patterson D. Lactobacillus casei microbiological assay of
18. Antonelli MA, Moreland LW, Brick JE. Herpes Zoster in patients with folic acid derivatives in 96-well microtiter plates. Clin Chem. 1988;34:
rheumatoid arthritis treated with weekly, low-dose methotrexate. Am J 2357-9.
Med. 1991;90:295-8. 45. Stacewicz-Sapuntzakis M, Bowen PE, Kikendall JW, Burgess M. Si-
19. MacKinnon SK, Starkebaum G, Willkens RF. Pancytopenia associated multaneous determination of serum retinol and various carotenoids:
with low dose pulse methotrexate in the treatment of rheumatoid their distribution in middle-aged men and women. Journal of Micro-
arthritis. Semin Arthritis Rheum. 1985;15:119-26. nutrient Analysis. 1987;3:27-45.
20. Cannon GW, Ward JR, Clegg DO, Samuelson CO Jr, Abbott TM. 46. Lau KS, Gottlieb C, Wasserman LR, Herbert V. Measurement of
Acute lung disease associated with low-dose pulse methotrexate ther- serum vitamin B 1 2 level using radioisotope dilution and coated char-
apy in patients with rheumatoid arthritis. Arthritis Rheum. 1983;26: coal. Blood. 1965;26:202-14.
1269-74. 47. Omaye ST, Schaus EE, Kutnink MA, Hawkes WC. Measurement of
840 1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
vitamin C in blood components by high-performance liquid chroma- Williams HJ, et al. Methotrexate for rheumatoid arthritis. Suggested
tography. Implication in assessing vitamin C status. Ann N Y Acad guidelines for monitoring liver toxicity. American College of Rheuma-
Sci. 1987;498:398-401. tology. Arthritis Rheum. 1994;3:316-28.
48. Bayoumi RA, Rosalki SB. Evaluation of methods of coenzyme activa- 59. Butterworth CE Jr, Tamura T. Folic acid safety and toxicity: a brief
tion of erythrocyte enzymes for detection of deficiency of vitamins Bl, review. Am J Clin Nutr. 1989;50:353-8.
B2, and B6. Clin Chem. 1976;22:327-35. 60. Weinblatt ME, Fraser P. Elevated mean corpuscular volume as a
49. Waring PP, Fisher D, McDonnell J, McGown EL, Sauberlich HE. A predictor of hematologic toxicity due to methotrexate therapy. Arthri-
continuous-flow (AutoAnalyzer II) procedure for measuring erythro- tis Rheum. 1989;32:1592-6.
cyte transketolase activity. Clin Chem. 1982;28:2206-13. 61. Duhra P. Treatment of gastrointestinal symptoms associated with
50. Skala JH, Gretz D, Waring PP. An automated continuous-flow pro- methotrexate therapy for psoriasis. J Am Acad Dermatol. 1993;28:
cedure for simultaneous measurement of erythrocyte alanine and as- 466-9.
partate aminotransferase activities. Nutrition Research. 1987;7:731-41. 62. Furst DE. Clinical pharmacology of very low dose methotrexate for
51. Baker H, Frank O. Vitamin A and carotenes. In: Clinical Vitaminol- use in rheumatoid arthritis. J Rheumatol. 1985;12:11-4.
ogy. New York: Interscience Publishers; 1968.
63. Sinnett MJ, Groff GD, Raddatz DA, Franck WA, Bertino JS Jr.
52. Sharp JT, Young DY, Bluhm GB, Brook A, Brower AC, Corbett M, et
Methotrexate pharmacokinetics in patients with rheumatoid arthritis.
al. How many joints in the hands and wrists should be included in a
J Rheumatol. 1989;16:745-8.
score of radiologic abnormalities used to assess rheumatoid arthritis?
64. Edelman J, Biggs DF, Jamali F, Russell AS. Low-dose methotrexate
Arthritis Rheum. 1985;28:1326-35.
kinetics in arthritis. Clin Pharmacol Ther. 1984;35:382-6.
53. Weinblatt ME, Kaplan H, Germain BF, Merriman RC, Solomon SD,
Wall B, et al. Low-dose methotrexate compared with auranofln in 65. Laffourgue P, Monjanel-Mouterde S, Durand A, Catalin J, Acquavia
adult rheumatoid arthritis. A thirty-six-week, double-blind trial. Arthri- PC. Is there an interaction between low doses of corticosteroids and
tis Rheum. 1990;33:330-8. methotrexate in patients with rheumatoid arthritis? A pharmacokinetic
54. Cohen J. Statistical Power Analysis for the Behavioral Sciences. New study in 33 patients. J Rheumatol. 1993;20:263-7
York: Academic Press; 1977. 66. Centers for Disease Control and Prevention. Recommendation for the
55. Borenstein M, Cohen J. Statistical Power Analysis: A Computer Pro- use of folic acid to reduce the number of cases of spina bifida and
gram. Hilldale, New Jersey: Lawerence Erlbaum Associates; 1988. other neural tube defects. MMWR Morb Mortal Wkly Rep. 1992;41:1-7.
56. Subar AF, Block G, James LD. Folate intake and food sources in the 67. Nightingale SL. Proposals for folic acid fortification and labeling of
US population. Am J Clin Nutr. 1989;50:508-16. certain foods to reduce risk of neural tube defects. JAMA. 1993;270:
57. Morgan SL, Hine RJ, Vaughn WH, Brown A. Dietary intake and 2283.
circulating vitamin levels of rheumatoid arthritis patients treated with 68. Baggott JE, Morgan SL, Ha TS, Alarcon GS, Koopman WJ, Krum-
methotrexate. Arthritis Care Res. 1993;6:4-10. dieck CL. Antifolates in rheumatoid arthritis: a hypothetical mecha-
58. Kremer JM, Alarcon GS, Lightfoot RW Jr, Willkens RF, Furst DE, nism of action. Clin Exp Rheumatol. 1993;ll:S101-5.
1 December 1994 • Annals of Internal Medicine • Volume 121 • Number 11 841
Downloaded From: http://annals.org/ by a Tulane University User on 05/13/2015
You might also like
- Dying To Be Thin ReviewDocument5 pagesDying To Be Thin Reviewapi-242071284No ratings yet
- MAF Method SummaryDocument8 pagesMAF Method SummaryJavier Fernández CondeNo ratings yet
- Practical Homoepathy D S Vohra.01577 2case StuediesDocument4 pagesPractical Homoepathy D S Vohra.01577 2case StuediessumarumNo ratings yet
- Hilot Philippine Traditional MassageDocument3 pagesHilot Philippine Traditional MassageXiaoYing100% (12)
- MTX in D 2007Document13 pagesMTX in D 2007Ari KurniawanNo ratings yet
- Drug Interactions With Azithromycin and The Macrolides: An OverviewDocument10 pagesDrug Interactions With Azithromycin and The Macrolides: An OverviewAranel BomNo ratings yet
- Methotrexate in Rheumatoid Arthritis Efficacy and Safety 2329 6887 2 127Document4 pagesMethotrexate in Rheumatoid Arthritis Efficacy and Safety 2329 6887 2 127Saifuddin HaswareNo ratings yet
- Understanding The Mechanisms of Action of MethotrexateDocument6 pagesUnderstanding The Mechanisms of Action of MethotrexateMuhamad Rizqy MaulanaNo ratings yet
- Multinational Evidence-Based Recommendations ForDocument40 pagesMultinational Evidence-Based Recommendations FordawniejuneNo ratings yet
- Clinical Pharmacokinetics of Methotrexate: D.O. Shen and DL AzarnoffDocument2 pagesClinical Pharmacokinetics of Methotrexate: D.O. Shen and DL AzarnoffAdkhiatul MuslihatinNo ratings yet
- Eectiveness Tolerability and Safety of Tofacitinib inDocument14 pagesEectiveness Tolerability and Safety of Tofacitinib indanny gomezNo ratings yet
- Psoriasis Treatments GuidelinesDocument33 pagesPsoriasis Treatments GuidelinesWay FastNo ratings yet
- Effect FolicDocument9 pagesEffect FolicAmalia NandiaNo ratings yet
- Reviews: Methotrexate and Its Mechanisms of Action in Inflammatory ArthritisDocument10 pagesReviews: Methotrexate and Its Mechanisms of Action in Inflammatory ArthritisanitaNo ratings yet
- Cerminara Et Al 2017 A Single Center Retrospective Analysis of A Protocol For High Dose Methotrexate and LeucovorinDocument9 pagesCerminara Et Al 2017 A Single Center Retrospective Analysis of A Protocol For High Dose Methotrexate and Leucovorinanton.neonatusNo ratings yet
- Feature: Extracorporeal Treatment For Methotrexate PoisoningDocument21 pagesFeature: Extracorporeal Treatment For Methotrexate PoisoningPaola ZuluagaNo ratings yet
- Journal of Oncological Sciences: Rashida Muhammad UmarDocument5 pagesJournal of Oncological Sciences: Rashida Muhammad UmarFiore PanceNo ratings yet
- Pharmacological Interactions of VasoconstrictorsDocument8 pagesPharmacological Interactions of VasoconstrictorsValeska Farina EspinosaNo ratings yet
- Methotrexte PIDocument27 pagesMethotrexte PIMichael FreudigerNo ratings yet
- Clinically Relevant Drug-Drug Interactions in Oncology: Howard L. McleodDocument6 pagesClinically Relevant Drug-Drug Interactions in Oncology: Howard L. McleodCindyGaniNo ratings yet
- Efektivititas Pemberian Obat Methotrexate Dibandingkan Obat LeflunamidDocument5 pagesEfektivititas Pemberian Obat Methotrexate Dibandingkan Obat Leflunamidhilman lesmanaNo ratings yet
- 2016 Medical Ozone Increases Methotrexate Clinical Response and Improves Cellular Redox Balance in Patients With Rheumatoid ArthritisDocument6 pages2016 Medical Ozone Increases Methotrexate Clinical Response and Improves Cellular Redox Balance in Patients With Rheumatoid ArthritisAcupuntura de EquinosNo ratings yet
- Friedman 2018Document7 pagesFriedman 2018Genshin SatuNo ratings yet
- Polymorphism in Gene For ABCC2 Transporter PredictDocument12 pagesPolymorphism in Gene For ABCC2 Transporter PredictGregorius HocevarNo ratings yet
- JurnalDocument5 pagesJurnalkadekNo ratings yet
- 1 s2.0 S1297319X18301817 MainDocument7 pages1 s2.0 S1297319X18301817 MainDanianto WicaksonoNo ratings yet
- Methotrexate - StatPearls - NCBI BookshelfDocument1 pageMethotrexate - StatPearls - NCBI Bookshelfanoy judeNo ratings yet
- C1C13 and C14-Methotrexate - Methotrexate Sodium (CPhA Monograph)Document13 pagesC1C13 and C14-Methotrexate - Methotrexate Sodium (CPhA Monograph)Mina AzmyNo ratings yet
- BPH Smith English-6-15Document10 pagesBPH Smith English-6-15novi camiumNo ratings yet
- Drug-Drug, Drug-Dietary Supplement, and Drug-Citrus Fruit and Other Food Interactions: What Have We Learned?Document11 pagesDrug-Drug, Drug-Dietary Supplement, and Drug-Citrus Fruit and Other Food Interactions: What Have We Learned?Brian JonesNo ratings yet
- ArticuloDocument10 pagesArticuloYoselyn Jhoana Limache MarinNo ratings yet
- RA1Document4 pagesRA1Intan Winta PratiwiNo ratings yet
- Methotrexate 27Document27 pagesMethotrexate 27Asia KanwalNo ratings yet
- Drug Anim, AlDocument5 pagesDrug Anim, AlakondisNo ratings yet
- Salapolivalente 02 Net3 JldapenaDocument42 pagesSalapolivalente 02 Net3 JldapenaBenjamínGalvanNo ratings yet
- Enantiomers Evaluation CetirizineDocument4 pagesEnantiomers Evaluation Cetirizinebebel555No ratings yet
- Will Pharmacogenetics Allow Better Prediction of MTX Toxicity and Efficacy in Patients With Rheumatoid ArthritisDocument7 pagesWill Pharmacogenetics Allow Better Prediction of MTX Toxicity and Efficacy in Patients With Rheumatoid Arthritisdoc0814No ratings yet
- Lajevardi Et Al-2015-International Journal of DermatologyDocument7 pagesLajevardi Et Al-2015-International Journal of DermatologyRizka Leonita FahmyNo ratings yet
- Current Status of 5 of Lower Urinary Tract Symptoms and BPH: - Reductase Inhibitors in The ManagementDocument8 pagesCurrent Status of 5 of Lower Urinary Tract Symptoms and BPH: - Reductase Inhibitors in The ManagementApriani BahoriNo ratings yet
- Therapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsDocument7 pagesTherapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsSerley WulandariNo ratings yet
- Tropisetron 26Document6 pagesTropisetron 26Tori SepriwanNo ratings yet
- Effect of Different Durations of Ketoconazole Dosing On The Single-Dose Pharmacokinetics of MidazDocument10 pagesEffect of Different Durations of Ketoconazole Dosing On The Single-Dose Pharmacokinetics of MidazLuciana OliveiraNo ratings yet
- Jurnal CimetidineDocument7 pagesJurnal CimetidineAidahNo ratings yet
- FOCUS STUDY For FebuxostatDocument7 pagesFOCUS STUDY For FebuxostatshaheenNo ratings yet
- Methotrexate Alopecia AreataDocument10 pagesMethotrexate Alopecia AreataThorn MailNo ratings yet
- Ncologist: R I FDADocument7 pagesNcologist: R I FDAapi-26302710No ratings yet
- Wang 2018Document42 pagesWang 2018Erni SalehNo ratings yet
- Glucocorticoid (Dexamethasone) - Induced Metabolome Changes in Healthy Males Suggest Prediction of Response and Side EffectsDocument12 pagesGlucocorticoid (Dexamethasone) - Induced Metabolome Changes in Healthy Males Suggest Prediction of Response and Side EffectsGritoNo ratings yet
- Clinical Pharmacokinetics of FluoxetineDocument14 pagesClinical Pharmacokinetics of FluoxetinePalwasha MalikNo ratings yet
- Therapeutic Drug Monitoring of Levetiracetam and Lamotrigine: Is There A Need?Document8 pagesTherapeutic Drug Monitoring of Levetiracetam and Lamotrigine: Is There A Need?Klinik BayuNo ratings yet
- Short-Course Nitrofurantoin For The Treatment of Acute Uncomplicated Cystitis in WomenDocument6 pagesShort-Course Nitrofurantoin For The Treatment of Acute Uncomplicated Cystitis in WomenHanifah RifdaNo ratings yet
- Pharmacogenetics and The Concept of Individualized Medicine: BS ShastryDocument6 pagesPharmacogenetics and The Concept of Individualized Medicine: BS Shastrykunalprabhu148No ratings yet
- Jurnal Anti EmetikDocument5 pagesJurnal Anti EmetikkarinagiovanniNo ratings yet
- Pharmacogenomics: Learning ObjectivesDocument16 pagesPharmacogenomics: Learning ObjectivesJamilNo ratings yet
- Perspectives: Methotrexate-How Does It Really Work?Document4 pagesPerspectives: Methotrexate-How Does It Really Work?Genshin SatuNo ratings yet
- 1 RP130001 PDFDocument8 pages1 RP130001 PDFDiga AlbrianNo ratings yet
- 2020 - Emerging Challenges To The Safe and Effective Use of Methadone For Cancer-Related Pain in Paediatric and Adult Patient PopulationsDocument16 pages2020 - Emerging Challenges To The Safe and Effective Use of Methadone For Cancer-Related Pain in Paediatric and Adult Patient PopulationsPoliana carmonaNo ratings yet
- Drug Interactions Lecture Pre-ReadingDocument12 pagesDrug Interactions Lecture Pre-ReadingGregNo ratings yet
- European J Cancer Care - 2018 - Riu Viladoms - Drug Interactions With Oral Antineoplastic Drugs The Role of The PharmacistDocument5 pagesEuropean J Cancer Care - 2018 - Riu Viladoms - Drug Interactions With Oral Antineoplastic Drugs The Role of The PharmacistCatalina Del CantoNo ratings yet
- Keratolytics and Emollients and Their Role PDFDocument18 pagesKeratolytics and Emollients and Their Role PDFRez QNo ratings yet
- Jashore University of Science and TechnologyDocument16 pagesJashore University of Science and TechnologyBlood DonationNo ratings yet
- A Phase 2 Study of Two Doses of Bortezomib in Relapsed or Refractory MyelomaDocument8 pagesA Phase 2 Study of Two Doses of Bortezomib in Relapsed or Refractory MyelomaJLNo ratings yet
- Important Drug Nutrient InteractionsDocument7 pagesImportant Drug Nutrient InteractionsEleonora ComucciNo ratings yet
- Combination of Massage Therapy With Ultramagnetic Therapy: Does It Affect Shoulder Pain Rehabilitation?Document10 pagesCombination of Massage Therapy With Ultramagnetic Therapy: Does It Affect Shoulder Pain Rehabilitation?Alejandro Cordoba aparicioNo ratings yet
- IschemicHeartDisease LectureDocument64 pagesIschemicHeartDisease LectureFerdinand RobertNo ratings yet
- Zero Degrees of Empathy A New Theory of Human Cruelty WikiDocument5 pagesZero Degrees of Empathy A New Theory of Human Cruelty WikisyedhoqueNo ratings yet
- MINISTRY of HEALTH TRINIDAD & TOBAGO Manual of Procedures Related To The Inspection of Antibiotics and NarcoticsDocument10 pagesMINISTRY of HEALTH TRINIDAD & TOBAGO Manual of Procedures Related To The Inspection of Antibiotics and NarcoticsneilsengtaNo ratings yet
- Changing Face of Homoeopathic Pharmacy: Lecture by Dr. P. N. VarmaDocument44 pagesChanging Face of Homoeopathic Pharmacy: Lecture by Dr. P. N. VarmawasiuddinNo ratings yet
- Creep Feeding GoatDocument4 pagesCreep Feeding GoatqfarmsNo ratings yet
- InsidetrackDocument11 pagesInsidetrackprashant.acharyahnrNo ratings yet
- Secondary GlaucomaDocument22 pagesSecondary GlaucomaYeshiwas AbejeNo ratings yet
- Pelvic Floor DysfunctionDocument92 pagesPelvic Floor DysfunctionWindy Puspa KusumahNo ratings yet
- CystitisDocument24 pagesCystitisTaufik Ramadhan BiyaNo ratings yet
- PROCTOSIGMOIDOSDocument5 pagesPROCTOSIGMOIDOSJopet Llanita0% (1)
- Books: Chest Physiotherapy in The Intensive Care UnitDocument1 pageBooks: Chest Physiotherapy in The Intensive Care UnitHAMMYER ALROKHAMINo ratings yet
- Documentation and Reporting: Fundamentals of Nursing (NUPC 104)Document14 pagesDocumentation and Reporting: Fundamentals of Nursing (NUPC 104)Mayki GarciaNo ratings yet
- Kako Napisati I Publikovati Naucni RadDocument14 pagesKako Napisati I Publikovati Naucni RadJovan Z. PopovićNo ratings yet
- Gastrointestinal Series A. Upper GI SeriesDocument4 pagesGastrointestinal Series A. Upper GI SeriesShanna Marie Melodia100% (1)
- Fourth Semester FinalDocument14 pagesFourth Semester Finalmara5140No ratings yet
- Artifcial Liver Support in Patients With Liver Failure: A Modifed DELPHI Consensus of International ExpertsDocument16 pagesArtifcial Liver Support in Patients With Liver Failure: A Modifed DELPHI Consensus of International Expertsmedico89No ratings yet
- Kasus+gout+dan+hiperuricemiaDocument3 pagesKasus+gout+dan+hiperuricemiareffadaNo ratings yet
- Orbital Decompression, Optic N Decompression and EndoDCRDocument97 pagesOrbital Decompression, Optic N Decompression and EndoDCRAlok RathiNo ratings yet
- Common Gastrointestinal Problems and Emergencies in Neonates and ChildrenDocument24 pagesCommon Gastrointestinal Problems and Emergencies in Neonates and ChildrenPatrick KosgeiNo ratings yet
- Letters To The Editor: Dr. Donald FoubisterDocument2 pagesLetters To The Editor: Dr. Donald FoubisterSohail LatifNo ratings yet
- Ultrasound in Anesthesia, Critical Care, and Pain.19Document2 pagesUltrasound in Anesthesia, Critical Care, and Pain.19Syamsi KubangunNo ratings yet
- The Role of Nurse Practitioners in Care Coordination and TransitionDocument10 pagesThe Role of Nurse Practitioners in Care Coordination and Transitionapi-312364579No ratings yet
- Ada 2017Document142 pagesAda 2017Ana Maria Ramos Rojas100% (1)
- Acute GastritisDocument14 pagesAcute GastritisMenchie Vivas-AlotNo ratings yet
- NPO Means "Nothing by Mouth," From The LatinDocument4 pagesNPO Means "Nothing by Mouth," From The Latin14 zarwa hassanNo ratings yet