Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- (The Master Work Series) Otto F. Kernberg - Borderline Conditions and Pathological Narcissism-Jason Aronson, Inc. (2000)Document376 pages(The Master Work Series) Otto F. Kernberg - Borderline Conditions and Pathological Narcissism-Jason Aronson, Inc. (2000)Roxana Apostol100% (10)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Daily Calorie Log WorksheetDocument6 pagesDaily Calorie Log WorksheetBladeNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
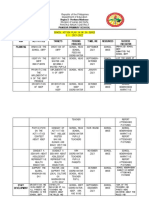
- Ok Sa Deped Action Plan 2021 2022Document3 pagesOk Sa Deped Action Plan 2021 2022Mamaanun PS100% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Uveitis WorkupDocument75 pagesUveitis WorkupGopal RaoNo ratings yet
- Primary Hypospadias Repair Techniques: A Review of The EvidenceDocument6 pagesPrimary Hypospadias Repair Techniques: A Review of The EvidencebenimhepfiNo ratings yet
- The GMS Hypospadias Score: Assessment of Inter-Observer Reliability and Correlation With Post - Operative ComplicationsDocument6 pagesThe GMS Hypospadias Score: Assessment of Inter-Observer Reliability and Correlation With Post - Operative ComplicationsbenimhepfiNo ratings yet
- A Standardized Classification of Hypospadias: Marek OrkiszewskiDocument5 pagesA Standardized Classification of Hypospadias: Marek OrkiszewskibenimhepfiNo ratings yet
- Site of Urethral Meatus (Before Chordee Correction)Document1 pageSite of Urethral Meatus (Before Chordee Correction)benimhepfiNo ratings yet
- ENT Meds ListDocument4 pagesENT Meds ListnickikNo ratings yet
- On-Call X-Rays Made Easy - NodrmDocument305 pagesOn-Call X-Rays Made Easy - NodrmSara Navarro50% (2)
- SDS Floor DeodorizerDocument6 pagesSDS Floor Deodorizersee wan lerNo ratings yet
- Alcoholism and Native AmericansDocument3 pagesAlcoholism and Native AmericansGary DeMonteNo ratings yet
- 7-29-21 Gov McMaster To Dir Leach Re Federal SNAP ExtensionDocument3 pages7-29-21 Gov McMaster To Dir Leach Re Federal SNAP ExtensionABC15 NewsNo ratings yet
- Paracetamol Use With Bexsero: in Children Aged Under 2 YearsDocument1 pageParacetamol Use With Bexsero: in Children Aged Under 2 YearswindiNo ratings yet
- Psychology SyllabusDocument62 pagesPsychology SyllabusshiningemporiumNo ratings yet
- 2022 - 015 - p5 Sa2 Exam Letter For Parents (Final - PG)Document7 pages2022 - 015 - p5 Sa2 Exam Letter For Parents (Final - PG)Sophie-Rae TeNo ratings yet
- A List of Psychological DisordersDocument12 pagesA List of Psychological DisordersGaurav LahotiNo ratings yet
- Carillo V PeopleDocument3 pagesCarillo V PeopleAnonymous AUdGvYNo ratings yet
- AL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteDocument2 pagesAL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteJazzmine C. RubricoNo ratings yet
- MSLSS Multidimensional Student Life Satisfaction ScaleDocument3 pagesMSLSS Multidimensional Student Life Satisfaction ScaleChris Gabriel Ucol100% (1)
- Cannondale 2012 IQ200 Cycling Computer FINALDocument4 pagesCannondale 2012 IQ200 Cycling Computer FINALAdrian Popescu0% (1)
- Angiotensin-Converting EnzymeDocument7 pagesAngiotensin-Converting EnzymenembutalNo ratings yet
- DR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDocument27 pagesDR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDhiraj PantNo ratings yet
- PortfolioDocument28 pagesPortfoliorizwan mughalNo ratings yet
- Risk Assessment Work InstructionDocument3 pagesRisk Assessment Work Instructionabdulrehman731No ratings yet
- Heart and Neck Vessels AssessmentDocument8 pagesHeart and Neck Vessels Assessmentfatimafaith1129No ratings yet
- What Do Fire & Hole Watchers Do?: Primary DutyDocument1 pageWhat Do Fire & Hole Watchers Do?: Primary DutySumit ShindeNo ratings yet
- V FIT ST STB09 1 InstDocument24 pagesV FIT ST STB09 1 InstSudeep Jacob JosephNo ratings yet
- TM 5-3800-205-23-3 Model 613CWDDocument344 pagesTM 5-3800-205-23-3 Model 613CWDAdvocateNo ratings yet
- There Should Be More Dancing by Rosalie Ham - Reading GuideDocument3 pagesThere Should Be More Dancing by Rosalie Ham - Reading GuideRandomHouseAU100% (1)
- Bone HealingDocument5 pagesBone HealingFadliArifNo ratings yet
- Anemia Makrositik (Defisiensi Cyanocobalamin) (English)Document34 pagesAnemia Makrositik (Defisiensi Cyanocobalamin) (English)sujidahNo ratings yet
- DCH EHAQ 4TH Action PlaneDocument11 pagesDCH EHAQ 4TH Action PlaneMiraf Mesfin100% (1)
- J Annemergmed 2017 01 018Document14 pagesJ Annemergmed 2017 01 018Jorge BarriosNo ratings yet