Download as pdf or txt
You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Community Health Nursing + Copar 4 - Mbol Batch 2021 Sep 14 RigonDocument61 pagesCommunity Health Nursing + Copar 4 - Mbol Batch 2021 Sep 14 RigonSean Lloyd RigonNo ratings yet
- National Essential Drug List (Malaysia) PDFDocument11 pagesNational Essential Drug List (Malaysia) PDFKah Jun100% (1)
- Louis Pasteur: by Jamie MignotDocument33 pagesLouis Pasteur: by Jamie MignotGiovanni BuzulanNo ratings yet
- Sinovac Vaccine ExplainerDocument6 pagesSinovac Vaccine ExplainerAnilNo ratings yet
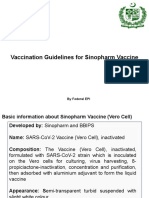
- V.3 21195 Sinopharm Vaccine Explainer 24Document6 pagesV.3 21195 Sinopharm Vaccine Explainer 24Mohammad Hisham BhawpalNo ratings yet
- COVID-19 Vaccine AstraZeneca ExplainerDocument6 pagesCOVID-19 Vaccine AstraZeneca ExplainerBakNo ratings yet
- 14h30 26-Mar 21078 JanssenDocument6 pages14h30 26-Mar 21078 JanssenSavu BogdanNo ratings yet
- E Evaluation Report CoronaVacDocument41 pagesE Evaluation Report CoronaVacEdward CNo ratings yet
- Pfizer Vaccine Explainer Version 2Document6 pagesPfizer Vaccine Explainer Version 2Samanta SlanaNo ratings yet
- Covid-19 Vaccine Chadox1-S (Recombinant)Document7 pagesCovid-19 Vaccine Chadox1-S (Recombinant)JMF750No ratings yet
- The Sinovac VaccineDocument4 pagesThe Sinovac VaccineMontasir BalambagNo ratings yet
- COVID-19 MRNA Vaccine MRNA-1273 ModernaDocument4 pagesCOVID-19 MRNA Vaccine MRNA-1273 ModernawalkrogNo ratings yet
- Fact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2Document3 pagesFact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2marie-eve guyNo ratings yet
- Covid 19 VaccineDocument13 pagesCovid 19 Vaccine9480463463No ratings yet
- Sinopharm Training Guide - 29 1 2021Document24 pagesSinopharm Training Guide - 29 1 2021shahbaz aliNo ratings yet
- COVID-19 Vaccine Comparison: Issue BriefDocument4 pagesCOVID-19 Vaccine Comparison: Issue BriefJimmy FebrianNo ratings yet
- เอกสารกำกับยา ภาษาอังกฤษ SinovacDocument12 pagesเอกสารกำกับยา ภาษาอังกฤษ SinovacAtawit SomsiriNo ratings yet
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryJohn Alex SelorioNo ratings yet
- COVID-19 AstraZeneca Vaccine AdminDocument13 pagesCOVID-19 AstraZeneca Vaccine AdminKyaw MinNo ratings yet
- Moderna Vaccine Screening Questions 2020-12-29Document2 pagesModerna Vaccine Screening Questions 2020-12-29TLNo ratings yet
- Vaccines in Respiratory Infection 111Document36 pagesVaccines in Respiratory Infection 111K R DivyaNo ratings yet
- Red Biotechnology 3 PPT 2021Document44 pagesRed Biotechnology 3 PPT 2021Vanessa SantiagoNo ratings yet
- Immunization ScheduleDocument2 pagesImmunization ScheduleTracy100% (1)
- Qdenga Epar Product Information enDocument47 pagesQdenga Epar Product Information enNovrina Wahidah RestiNo ratings yet
- Contraindications and Precautionary Conditions For VaccinatiDocument25 pagesContraindications and Precautionary Conditions For VaccinatikrishnasreeNo ratings yet
- Janssen Prep and Admin SummaryDocument3 pagesJanssen Prep and Admin SummaryAnania ClementNo ratings yet
- WHO EURO 2021 2480 42236 58306 EngDocument3 pagesWHO EURO 2021 2480 42236 58306 EngRizka NoviandariNo ratings yet
- COVAXIN Product InfoDocument7 pagesCOVAXIN Product InfoJoseph Raymund BautistaNo ratings yet
- 13 Summary of Product Characteristics Labelling Package LeafletDocument20 pages13 Summary of Product Characteristics Labelling Package LeafletEnrique Carranza100% (1)
- Varicella Post-ProphylaxisDocument2 pagesVaricella Post-ProphylaxisAngelaTrinidadNo ratings yet
- Incovacc FactsheetDocument1 pageIncovacc FactsheetmerkiserzoNo ratings yet
- Who Should Be Vaccinated First?Document4 pagesWho Should Be Vaccinated First?Claire FernandezNo ratings yet
- U1dr2c1072660000411c SPC enDocument16 pagesU1dr2c1072660000411c SPC enCheung Yuk YamNo ratings yet
- Covid-19 Vaccine Faq: What Is An mRNA Vaccine and How Does It Work?Document7 pagesCovid-19 Vaccine Faq: What Is An mRNA Vaccine and How Does It Work?Kipas AnginNo ratings yet
- FAQ - COVID-19 VaccineDocument5 pagesFAQ - COVID-19 Vaccinejianhe sunNo ratings yet
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration Summarywilltippin4747No ratings yet
- Interim Recommendations For Use of The Inactivated Covid-19 Vaccine, Coronavac, Developed by SinovacDocument9 pagesInterim Recommendations For Use of The Inactivated Covid-19 Vaccine, Coronavac, Developed by SinovacNathaly BarretoNo ratings yet
- Vaxzevria Previously Covid 19 Vaccine Astrazeneca Epar Medicine Overview - enDocument5 pagesVaxzevria Previously Covid 19 Vaccine Astrazeneca Epar Medicine Overview - enRestu Annisa PutriNo ratings yet
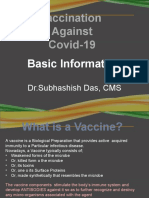
- Vaccination Against Covid-19: Basic InformationDocument46 pagesVaccination Against Covid-19: Basic InformationSubhashish DasNo ratings yet
- (Updated) J&J - 15july2021Document14 pages(Updated) J&J - 15july2021christelm_1No ratings yet
- Kiss Covid VaccinationsDocument4 pagesKiss Covid VaccinationsMohamed Ali KalathingalNo ratings yet
- Coronavirus (COVID-19) Vaccination For Seafarers and Shipping Companies: A Practical GuideDocument8 pagesCoronavirus (COVID-19) Vaccination For Seafarers and Shipping Companies: A Practical GuideCharlesNo ratings yet
- COVAXINDocument3 pagesCOVAXINRakshit VermaNo ratings yet
- Faqs For Healthcare Workers and Front Line Workers GeneralDocument12 pagesFaqs For Healthcare Workers and Front Line Workers GeneraltejaNo ratings yet
- Janssen Covid-19 Vaccine Journal Club ZwachteDocument4 pagesJanssen Covid-19 Vaccine Journal Club Zwachteapi-552486649No ratings yet
- Nuvaxovid Epar Product Information enDocument31 pagesNuvaxovid Epar Product Information enKiss TiborNo ratings yet
- Guidelines For Sputnik V Vaccine - 6101Document5 pagesGuidelines For Sputnik V Vaccine - 6101Usman JamilNo ratings yet
- 46 Saniya Ruqsar PPT On VaccineDocument11 pages46 Saniya Ruqsar PPT On VaccinemaherNo ratings yet
- Cervarix 2018Document26 pagesCervarix 2018Jacob PaglinawanNo ratings yet
- Pfizer Vaccine Explainer Version 2Document9 pagesPfizer Vaccine Explainer Version 2nqosa neidscqNo ratings yet
- Annex I Summary of Product CharacteristicsDocument33 pagesAnnex I Summary of Product CharacteristicsVimala BohoNo ratings yet
- Covid Vaccine EfficacyDocument3 pagesCovid Vaccine EfficacyNathaniel LaranjoNo ratings yet
- The Oxford/Astrazeneca Covid-19 Vaccine: What You Need To KnowDocument24 pagesThe Oxford/Astrazeneca Covid-19 Vaccine: What You Need To KnowmeiNo ratings yet
- FAQ Convidecia 17082021Document5 pagesFAQ Convidecia 17082021FarhanaNo ratings yet
- Covid-19 Vaccine and CancerDocument12 pagesCovid-19 Vaccine and CancerJelyn DiwaNo ratings yet
- ImmunizationDocument40 pagesImmunizationJasmin PastoresNo ratings yet
- Vaccine PHCDocument7 pagesVaccine PHCmntzrzyd6No ratings yet
- Varilrix Serbuk Injeksi 2000 PFU, Dosis - Vaksin Varisela - Zoster - DKI9676701044A1 - 2018 - 3Document8 pagesVarilrix Serbuk Injeksi 2000 PFU, Dosis - Vaksin Varisela - Zoster - DKI9676701044A1 - 2018 - 3rianaNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years and Older)Document5 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years and Older)Hannah Caburian RemoNo ratings yet
- ACC Qdenga SMPCDocument18 pagesACC Qdenga SMPCAngsamerahNo ratings yet
- Kepi Vaccines (2) - Gi - 1Document30 pagesKepi Vaccines (2) - Gi - 1okwadha simionNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- The Wayland News November 2013Document16 pagesThe Wayland News November 2013Julian HornNo ratings yet
- Immunization RecordDocument4 pagesImmunization RecordVin BitzNo ratings yet
- VPH 83.43 Rev.1 Chap5Document69 pagesVPH 83.43 Rev.1 Chap5jubatus.libroNo ratings yet
- Past Quiz QuestionsDocument4 pagesPast Quiz QuestionsAbubakar AbdhooNo ratings yet
- E Vaccination System Using AiDocument17 pagesE Vaccination System Using AiBRO.V͙A͙M͙S͙I͙ Ƥeͥ†eͣrͫ꧂No ratings yet
- Preventive MedicineDocument5 pagesPreventive Medicinescribdnotes123No ratings yet
- p.5 Science Questions Tekart LearningDocument43 pagesp.5 Science Questions Tekart Learninglazorus LEVITICUSNo ratings yet
- Histeria Por Vacunación Mass Psychogenic Illness After Vaccination 2003Document6 pagesHisteria Por Vacunación Mass Psychogenic Illness After Vaccination 2003Oscar Alejandro Cardenas QuinteroNo ratings yet
- Annual Report Adjusted 2010Document166 pagesAnnual Report Adjusted 2010Ralph ZazulaNo ratings yet
- WHO/BS/06.2050 - Final English Only: Expert Committee On Biological StandardizationDocument66 pagesWHO/BS/06.2050 - Final English Only: Expert Committee On Biological StandardizationSleeping KnightNo ratings yet
- AviPro News Issue1Document4 pagesAviPro News Issue1Bryan NicollNo ratings yet
- TRS - 978 - Annex - 5 Yellow Fever PDFDocument74 pagesTRS - 978 - Annex - 5 Yellow Fever PDFPradeep KumarNo ratings yet
- Protein TherapeuticsDocument14 pagesProtein TherapeuticsSumanth Kumar ReddyNo ratings yet
- Clil Lesson Method ScenariosDocument100 pagesClil Lesson Method ScenariosMariely AcevedoNo ratings yet
- Letter From Doctors To APSDocument2 pagesLetter From Doctors To APSJustin HinkleyNo ratings yet
- Primary Health Care HandoutsDocument34 pagesPrimary Health Care HandoutspauchanmnlNo ratings yet
- Blackbird AIDocument12 pagesBlackbird AILatoya SchumerNo ratings yet
- Confirmation Notice2Document4 pagesConfirmation Notice2Sasha GaishunNo ratings yet
- Group 3 - Position PaperDocument8 pagesGroup 3 - Position PaperNicole OlegarioNo ratings yet
- Population ExplosionDocument52 pagesPopulation ExplosionusmansherdinNo ratings yet
- Interventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsDocument10 pagesInterventions To Increase Pediatric Vaccine Uptake An Overview of Recent FindingsMariaNo ratings yet
- AmeworkDocument11 pagesAmeworkGeorgia De OcampoNo ratings yet
- Golden Points PDFDocument29 pagesGolden Points PDFBijay Kumar MahatoNo ratings yet
- PHICS HCW Immunization Recommendation UpdateDocument49 pagesPHICS HCW Immunization Recommendation UpdatearingkinkingNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary Detailssyed sharifNo ratings yet
- Communicable DiseasesDocument10 pagesCommunicable Diseasesapi-276039341No ratings yet
- Expanded Program For Immunization LECTURE NOTESDocument4 pagesExpanded Program For Immunization LECTURE NOTESSarahLabadan67% (3)