Download as pdf or txt
You might also like
- Guideline Managing Critically IllDocument8 pagesGuideline Managing Critically Illmisfatrianoor10No ratings yet
- Covid-19 For MRCP ExamsDocument6 pagesCovid-19 For MRCP ExamsZara VaraNo ratings yet
- Jama Poston 2020 Gs 200003Document3 pagesJama Poston 2020 Gs 200003Alex Fernando Páez VallejoNo ratings yet
- Lecture Anwar Ventilation Managment COVIDDocument28 pagesLecture Anwar Ventilation Managment COVIDمحمدرزازالتبعيNo ratings yet
- Medical Management-Critically IllDocument4 pagesMedical Management-Critically IllMiki MykesNo ratings yet
- Center For Physiotherapy and Rehabilitation Science Jamia Millia IslamiaDocument16 pagesCenter For Physiotherapy and Rehabilitation Science Jamia Millia IslamiaummiNo ratings yet
- CCJM 87a ccc040 FullDocument3 pagesCCJM 87a ccc040 FullRianNo ratings yet
- Noninvasive Ventilation in Acute Respiratory Failure in AdultsDocument12 pagesNoninvasive Ventilation in Acute Respiratory Failure in AdultsferrevNo ratings yet
- Critical Care Management of Covid-19 Algorithm-EngDocument1 pageCritical Care Management of Covid-19 Algorithm-EngMr CROWNo ratings yet
- Novel Coronavirus Update A Physician Perspective: Presented by Dr. Mohammad Amzarul M.D. (Medicine)Document35 pagesNovel Coronavirus Update A Physician Perspective: Presented by Dr. Mohammad Amzarul M.D. (Medicine)dramzarulNo ratings yet
- CDC AerosolDocument5 pagesCDC Aerosolwiwik sNo ratings yet
- Respiratory (Medicalstudyzone - Com)Document72 pagesRespiratory (Medicalstudyzone - Com)shahroozabbas66No ratings yet
- Intubation Guidelines SummaryDocument2 pagesIntubation Guidelines SummaryriccardoNo ratings yet
- COVID19Document79 pagesCOVID19Mohamad El SharNo ratings yet
- Prone Position Guidelines-2Document14 pagesProne Position Guidelines-2SAMINo ratings yet
- Management of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Document7 pagesManagement of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Abhishek GoelNo ratings yet
- Clinical Management of COVID-19 Patients - v1Document18 pagesClinical Management of COVID-19 Patients - v1rohitNo ratings yet
- ARDSDocument29 pagesARDSSwee ShiuanNo ratings yet
- CCJM 87a ccc033 FullDocument4 pagesCCJM 87a ccc033 FullKamar Operasi Hermina BogorNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICFirdaus FamilyNo ratings yet
- BTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Document21 pagesBTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Madalina TalpauNo ratings yet
- Aha Ventilación Modulo 3Document11 pagesAha Ventilación Modulo 3Juan Carlos GomezNo ratings yet
- Managing COVID-19 ARDS: Berlin DefinitionDocument3 pagesManaging COVID-19 ARDS: Berlin DefinitionastutikNo ratings yet
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocument39 pagesPresentasi Dr. Basuki Rachmad, Sp. An. KICinstalasi kamar bedah RSMINo ratings yet
- Thorax 2016BTS/ICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults Davidson Ii1 Ii35Document36 pagesThorax 2016BTS/ICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults Davidson Ii1 Ii35danelvNo ratings yet
- Management Guidelines For COVID 19 in Resource Limited Settings - MOH - NUG July 2021Document11 pagesManagement Guidelines For COVID 19 in Resource Limited Settings - MOH - NUG July 2021MYo OoNo ratings yet
- Non-Invasive Positive Pressure Ventilation (Nippv)Document4 pagesNon-Invasive Positive Pressure Ventilation (Nippv)docsandyy78No ratings yet
- COVID Management - Zone RAG Categories v6Document1 pageCOVID Management - Zone RAG Categories v6AgnesnesssongNo ratings yet
- Covid 19 Aerosol Generating Medical ProceduresDocument1 pageCovid 19 Aerosol Generating Medical ProceduresAbidi HichemNo ratings yet
- Module 9 Mechanical Ventilation PDFDocument46 pagesModule 9 Mechanical Ventilation PDFChabboo SutabrataNo ratings yet
- COVID-19 Management of Critical Care Cases PDFDocument6 pagesCOVID-19 Management of Critical Care Cases PDFLubna AliNo ratings yet
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocument38 pagesNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sNo ratings yet
- CPR Covid-19Document29 pagesCPR Covid-19Triana TingNo ratings yet
- Edited COVID19 HANDOUT Requina SindiongDocument5 pagesEdited COVID19 HANDOUT Requina SindiongJannen CasasNo ratings yet
- Terapi Oxygen Pada Pasien Covd-19Document24 pagesTerapi Oxygen Pada Pasien Covd-19normamNo ratings yet
- Ecleris Considerations NIV 05.05.20Document4 pagesEcleris Considerations NIV 05.05.20tanu wijayaNo ratings yet
- Covid19 - Pathophysiology and ManagementDocument51 pagesCovid19 - Pathophysiology and ManagementMyraflor CaroNo ratings yet
- Muhimbili COVID SummaryDocument7 pagesMuhimbili COVID SummaryMeNo ratings yet
- AnaConda Device in Critical CareDocument14 pagesAnaConda Device in Critical CaredistopicmagNo ratings yet
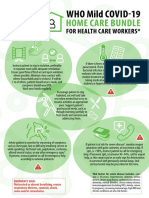
- WHO COVID-19-Home-Care-BundleDocument2 pagesWHO COVID-19-Home-Care-BundleOCSAF - P2LT PUNSALAN MCNo ratings yet
- DR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineDocument22 pagesDR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineP Vinod KumarNo ratings yet
- Fresh H1N1 Guidelines 1 - 1-18Document15 pagesFresh H1N1 Guidelines 1 - 1-18Shahid IqbalNo ratings yet
- Covid19 Infection Prevention and ControlDocument70 pagesCovid19 Infection Prevention and ControlAdeuga ADEKUOYENo ratings yet
- NCM 118 Lec Prelim 2Document13 pagesNCM 118 Lec Prelim 2SammNo ratings yet
- Niv Versus HFNCDocument30 pagesNiv Versus HFNCDukeNo ratings yet
- 02a - PPE - Summary and Rationale For RecommendationsDocument2 pages02a - PPE - Summary and Rationale For RecommendationsMohammedNo ratings yet
- Federal Democratic Republic of Ethiopia Ministry of HealthDocument43 pagesFederal Democratic Republic of Ethiopia Ministry of HealthdagemNo ratings yet
- Guidelines Gagal NafasDocument35 pagesGuidelines Gagal NafasRhevyNo ratings yet
- Mechanical Ventilition COVID GuidelinesDocument7 pagesMechanical Ventilition COVID Guidelinesheba abuhelwaNo ratings yet
- FAQs On COVID-19 From AIIMS e-ICUsDocument3 pagesFAQs On COVID-19 From AIIMS e-ICUsrakeshambasanaNo ratings yet
- In Managing Early Using: New Normal Respiratory Distress HFNTDocument51 pagesIn Managing Early Using: New Normal Respiratory Distress HFNTRaditya DidotNo ratings yet
- Clinical Management and TreatmentDocument3 pagesClinical Management and TreatmentAnni BarbaNo ratings yet
- High Flow Nasal Canula: Management of COVID-19 Patients: Department of Nursing Education and ResearchDocument12 pagesHigh Flow Nasal Canula: Management of COVID-19 Patients: Department of Nursing Education and ResearchIfan SetiadiNo ratings yet
- Airway ManagementDocument8 pagesAirway ManagementBaebee LouNo ratings yet
- Week 9-Respiratory EmergenciesDocument26 pagesWeek 9-Respiratory EmergenciesshrwqalhashmyhNo ratings yet
- Copd ManagementDocument7 pagesCopd ManagementPrincess OdigieNo ratings yet
- Whats New in GINA 2021 FinalDocument47 pagesWhats New in GINA 2021 FinalHeriestian eriesNo ratings yet
- Emergency Medicine SummaryDocument4 pagesEmergency Medicine SummaryokibreazyNo ratings yet
- Resp TestDocument7 pagesResp TestKong KongNo ratings yet