Download as docx, pdf, or txt
You might also like
- Communicable Disease Nursing: Mrs. Dionesia Mondejar NavalesDocument64 pagesCommunicable Disease Nursing: Mrs. Dionesia Mondejar NavalesChevelle Valenciano-Gaan0% (1)
- Neuro CH 14 Study GuideDocument9 pagesNeuro CH 14 Study GuideMichael J MillerNo ratings yet
- Manual of Modern Hydronics Section 1 4Document58 pagesManual of Modern Hydronics Section 1 4Tin Aung KyiNo ratings yet
- Tetanus Dr osobleDocument24 pagesTetanus Dr osobleaxlaamabdisamed20No ratings yet
- Tetanus DR Moses KazevuDocument13 pagesTetanus DR Moses KazevuMoses Jr KazevuNo ratings yet
- Tetanus KuliahDocument26 pagesTetanus Kuliahdemi190794No ratings yet
- Kejang TetanusDocument26 pagesKejang Tetanusriska silviaNo ratings yet
- Tetanus: DR - Vemuri ChaitanyaDocument49 pagesTetanus: DR - Vemuri ChaitanyaalifNo ratings yet
- Surgery Lecture On: Dr. Ehsanur RezaDocument23 pagesSurgery Lecture On: Dr. Ehsanur Rezaiga sukmaNo ratings yet
- TetanusDocument21 pagesTetanusDebjit SahaNo ratings yet
- Tetanus SaleemDocument17 pagesTetanus SaleemMueez BalochNo ratings yet
- Tetanus ADocument3 pagesTetanus ASadaqat KhanNo ratings yet
- TetanusDocument3 pagesTetanusRoma Nova Pascual CabarrubiasNo ratings yet
- FRACTUREDocument11 pagesFRACTUREOgbe HannahNo ratings yet
- Tetanu S: By: Reno WaisyahDocument18 pagesTetanu S: By: Reno WaisyahReno WaisyahNo ratings yet
- Pleno 3.1.3Document44 pagesPleno 3.1.3Debby Mulya RahmyNo ratings yet
- TetanusDocument27 pagesTetanusMohammed FareedNo ratings yet
- Tetanus: Dr. Rohmania SetiariniDocument32 pagesTetanus: Dr. Rohmania SetiariniAnnisa RahmaniNo ratings yet
- Tetanus: W Hat Is Tetanus?Document20 pagesTetanus: W Hat Is Tetanus?Stefanie BlueNo ratings yet
- PemicuDocument34 pagesPemicuCindy SugandaNo ratings yet
- Tetanus and Antibiotic Prophylaxis, Wound and Minor Soft Tissue TumorsDocument81 pagesTetanus and Antibiotic Prophylaxis, Wound and Minor Soft Tissue TumorsNárēsh Yadav GäddēNo ratings yet
- Clostridium Tetani: Tejpratap S.P. Tiwari, MD Pedro L. Moro, MD, MPH and Anna M. Acosta, MDDocument14 pagesClostridium Tetani: Tejpratap S.P. Tiwari, MD Pedro L. Moro, MD, MPH and Anna M. Acosta, MDClaudia FreyonaNo ratings yet
- GYLLE Meningitis Otitis Media Pertussis Pneumonia Rotavirus 1Document37 pagesGYLLE Meningitis Otitis Media Pertussis Pneumonia Rotavirus 1Marie Ashley CasiaNo ratings yet
- Tetanus 9 eDocument10 pagesTetanus 9 ea.hooker114No ratings yet
- Tetanus Disease by SlidesgoDocument31 pagesTetanus Disease by Slidesgoputri diva prinanda100% (1)
- TetanusDocument23 pagesTetanusNadya Noor Mulya Putri100% (1)
- Keys, Spinal Cord Diseases - 024456Document13 pagesKeys, Spinal Cord Diseases - 024456PrasadNo ratings yet
- Nursing Informatics: Bachelor of Science in NursingDocument6 pagesNursing Informatics: Bachelor of Science in NursingMichelle MallareNo ratings yet
- Case Study - Seizure2Document12 pagesCase Study - Seizure2Jenny-Ann Baliday100% (1)
- DjfhgoiefkDocument32 pagesDjfhgoiefkhoseajeremiaNo ratings yet
- 1 Orofacial PainDocument28 pages1 Orofacial Painaizen.obito.mNo ratings yet
- Tetanus - AnatomyDocument7 pagesTetanus - AnatomyJoro27No ratings yet
- Tetanus: Rika Arista Dewi S1-3ADocument14 pagesTetanus: Rika Arista Dewi S1-3ArikaaristadNo ratings yet
- Tetanus: Mrs.G.Manibharathi, MSC (N), Associate ProfessorDocument26 pagesTetanus: Mrs.G.Manibharathi, MSC (N), Associate ProfessormanibharathiNo ratings yet
- Seizure Disorder Types: Partial - Local Onset May or May Not Impair Consciousness SimpleDocument4 pagesSeizure Disorder Types: Partial - Local Onset May or May Not Impair Consciousness Simpleampogison08No ratings yet
- TetanusDocument12 pagesTetanusYulisa FitrianiNo ratings yet
- Kepaniteraan Klinik Rsms - FK Upn "Veteran" Jakarta: Penguji: Dr. Hernawan, SP.SDocument32 pagesKepaniteraan Klinik Rsms - FK Upn "Veteran" Jakarta: Penguji: Dr. Hernawan, SP.SOktaviano Satria PNo ratings yet
- Team 2 Case Study EpilepsyDocument15 pagesTeam 2 Case Study EpilepsytmgursalNo ratings yet
- Illustrator File Edit Select Effect View Window HelpDocument8 pagesIllustrator File Edit Select Effect View Window HelpHaizel BieberNo ratings yet
- TetanusDocument48 pagesTetanusJanuar RezkyNo ratings yet
- Trigger Point Homp. TehranDocument46 pagesTrigger Point Homp. TehranKasra Chehrazy100% (1)
- Neuro Disorders Study OutlineDocument9 pagesNeuro Disorders Study OutlineHeather Russell100% (1)
- Neurology Notes - NHY - 11 - 2023Document27 pagesNeurology Notes - NHY - 11 - 2023ezinne obinna-umaNo ratings yet
- Seizure Disorder, Spinal Injury Neural TumorDocument52 pagesSeizure Disorder, Spinal Injury Neural TumornipoNo ratings yet
- Epilepsyppt 180618175748Document38 pagesEpilepsyppt 180618175748Vasu LohraNo ratings yet
- TetanusDocument12 pagesTetanusKidistNo ratings yet
- Group 2 TetanusDocument43 pagesGroup 2 TetanusDaymon, Ma. TeresaNo ratings yet
- Kepaniteraan Klinik RSD Mardi Waluyo Blitar - FK Unisma: Pembimbing: Dr. Utchu Tedja Mulya SP.BDocument35 pagesKepaniteraan Klinik RSD Mardi Waluyo Blitar - FK Unisma: Pembimbing: Dr. Utchu Tedja Mulya SP.BDada DoniNo ratings yet
- 1 Diagnosis and Management of Orofacial Pain - Ali AlhussainiDocument9 pages1 Diagnosis and Management of Orofacial Pain - Ali Alhussainiammar slimanNo ratings yet
- 8 Clostridial InfectionsDocument39 pages8 Clostridial InfectionsHariharanNo ratings yet
- PainDocument18 pagesPaingouri debNo ratings yet
- Nursing Assessment 1Document6 pagesNursing Assessment 1Kedir AliyiNo ratings yet
- Pain 1 PDFDocument37 pagesPain 1 PDFSamwel EmadNo ratings yet
- TetanusDocument35 pagesTetanusWaNda GrNo ratings yet
- Neuro HXDocument7 pagesNeuro HXM NNo ratings yet
- Weebly Questions Week TenDocument3 pagesWeebly Questions Week Tenapi-459697337No ratings yet
- Seizure Disorders: Assessment and Diagnostic FindingsDocument3 pagesSeizure Disorders: Assessment and Diagnostic FindingsBlessed GarcianoNo ratings yet
- Q1.Flaccid Paresis: Diagnostical VariantsDocument47 pagesQ1.Flaccid Paresis: Diagnostical VariantsNelson OduorNo ratings yet
- Tetanus: Zaidi Abd Hamid Pensyarah Pembantu PerubatanDocument31 pagesTetanus: Zaidi Abd Hamid Pensyarah Pembantu PerubatanSyasya NanaNo ratings yet
- Spinal Stenosis And Pinched Nerve A Simple Guide to These conditionsFrom EverandSpinal Stenosis And Pinched Nerve A Simple Guide to These conditionsRating: 5 out of 5 stars5/5 (1)
- Intercostal Neuralgia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntercostal Neuralgia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Law of The Lord Is Perfect: Tes The Soul Ny Mo Ti Law The of Lord Fect, The Per Is of The Ing Vert Con TheDocument1 pageThe Law of The Lord Is Perfect: Tes The Soul Ny Mo Ti Law The of Lord Fect, The Per Is of The Ing Vert Con TheFG ArciagaNo ratings yet
- The Extremities and Spines: General ObjectivesDocument32 pagesThe Extremities and Spines: General ObjectivesFG ArciagaNo ratings yet
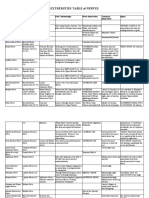
- Extremities Table of NervesDocument3 pagesExtremities Table of NervesFG ArciagaNo ratings yet
- Highest Blood Pressure Was 140/90 MMHGDocument5 pagesHighest Blood Pressure Was 140/90 MMHGFG ArciagaNo ratings yet
- Arciaga, FG - Ophtha Case Discussion 120622Document2 pagesArciaga, FG - Ophtha Case Discussion 120622FG ArciagaNo ratings yet
- Pedia Notes PDFDocument32 pagesPedia Notes PDFFG ArciagaNo ratings yet
- Arciaga, FG-ParaSGD 063021Document4 pagesArciaga, FG-ParaSGD 063021FG ArciagaNo ratings yet
- Coronavirus GuidancecoinfectionsDocument2 pagesCoronavirus GuidancecoinfectionsFG ArciagaNo ratings yet
- Arciaga, FG - SGDPara 051221Document4 pagesArciaga, FG - SGDPara 051221FG ArciagaNo ratings yet
- Arciaga, FG - PediaFC 051521Document10 pagesArciaga, FG - PediaFC 051521FG ArciagaNo ratings yet
- Light Millennium Man - LM 12-04 F SesamoDocument24 pagesLight Millennium Man - LM 12-04 F SesamoFranky AlbarranNo ratings yet
- Automatic Fire Control System in Railways 1Document44 pagesAutomatic Fire Control System in Railways 1RAJ50% (2)
- Cwf-60-30air CompressorDocument2 pagesCwf-60-30air CompressorHuy Lễ NguyễnNo ratings yet
- Launching Code, Algeria's First Coding School: Press ReleaseDocument3 pagesLaunching Code, Algeria's First Coding School: Press ReleaseClaire PershanNo ratings yet
- Tugas Individu 3Document3 pagesTugas Individu 3Penghancur DuniaNo ratings yet
- Marketing Plan Presentation RubricsDocument2 pagesMarketing Plan Presentation RubricsisabeloroseangelNo ratings yet
- Extract, Transform, Load: Inmon BillDocument11 pagesExtract, Transform, Load: Inmon BillLuntian Amour JustoNo ratings yet
- 4TH Summative Test Q2Document22 pages4TH Summative Test Q2Joehan DimaanoNo ratings yet
- Type of Contract (Tick The Appropriate Box) TA Title PurposeDocument7 pagesType of Contract (Tick The Appropriate Box) TA Title PurposeTesfaye BelayeNo ratings yet
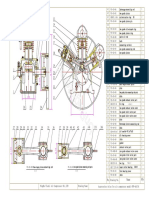
- ZA6VSD RysDocument1 pageZA6VSD RysDanielNo ratings yet
- Elements of Aeroelastic Design: Xie ChangchuanDocument21 pagesElements of Aeroelastic Design: Xie ChangchuanAbaziz Mousa OutlawZzNo ratings yet
- Label Non 3T v1Document9 pagesLabel Non 3T v1Febry Hisbullah NurmanNo ratings yet
- PDF DPWH Cost Estimation Manual For Low Rise Buildings DLDocument260 pagesPDF DPWH Cost Estimation Manual For Low Rise Buildings DLMichael Angelo Ballon100% (1)
- ISO 11820 - 1996 (En), Acoustics - Measurements On Silencers in Situ PDFDocument1 pageISO 11820 - 1996 (En), Acoustics - Measurements On Silencers in Situ PDFpighonNo ratings yet
- Autonomic Downlink Inter-Cell Interference Coordination in LTE Self-Organizing NetworksDocument5 pagesAutonomic Downlink Inter-Cell Interference Coordination in LTE Self-Organizing NetworksTarek Al AshhabNo ratings yet
- Diamond Kipah For JDocument3 pagesDiamond Kipah For JM MilliganNo ratings yet
- User Manual: Promia 50 Application - Material HandlingDocument110 pagesUser Manual: Promia 50 Application - Material Handlingred_shobo_85100% (2)
- AsDocument602 pagesAsnareshNo ratings yet
- China in A Changing Global Environment enDocument97 pagesChina in A Changing Global Environment enEskindirGirmaNo ratings yet
- Measures of Central Tendency and Dispersion (Week-07)Document44 pagesMeasures of Central Tendency and Dispersion (Week-07)Sarmad Altaf Hafiz Altaf HussainNo ratings yet
- Cse4001 Cloud-Computing TH 1.0 2 Cse4001Document2 pagesCse4001 Cloud-Computing TH 1.0 2 Cse4001sai22.ssbNo ratings yet
- How To Connect A Laptop To A ProjectorDocument87 pagesHow To Connect A Laptop To A ProjectorPurificacion, AnabeaNo ratings yet
- EA Publications With "Old" References Old References Documents Status Name of The DocumentDocument1 pageEA Publications With "Old" References Old References Documents Status Name of The DocumentAna Safranec VasicNo ratings yet
- Tutorial Letter 203/2/2017: General Chemistry 1BDocument18 pagesTutorial Letter 203/2/2017: General Chemistry 1BLeigh MakanNo ratings yet
- Lab 2 - Protection RelaysDocument10 pagesLab 2 - Protection RelaysLeo GeeNo ratings yet
- Serverless Architectures: Mike RobertsDocument51 pagesServerless Architectures: Mike RobertsfsmondiolatiroNo ratings yet
- UGC NET Paper 1Document17 pagesUGC NET Paper 1radhaNo ratings yet
- Travel Management - User ManualDocument24 pagesTravel Management - User ManualAlok Samataray100% (2)
- Listado de Gruas: Item Marca Modelo Serial MotorDocument2 pagesListado de Gruas: Item Marca Modelo Serial MotorOliver SemecoNo ratings yet