Download as docx, pdf, or txt
You might also like
- ElectivesDocument5 pagesElectivesসোমনাথ মহাপাত্র100% (1)
- RisperdalDocument2 pagesRisperdalAdrianne Bazo100% (1)
- Hypothyroidism (Drug Study)Document2 pagesHypothyroidism (Drug Study)Krisianne Mae Lorenzo FranciscoNo ratings yet
- Pregabalin LYricaDocument2 pagesPregabalin LYricaKristine Young100% (3)
- Insert - PreciControl Anti-SARS-CoV-2 S.ms - 09289313190.v1.enDocument2 pagesInsert - PreciControl Anti-SARS-CoV-2 S.ms - 09289313190.v1.enLilik IndrawatiNo ratings yet
- 1960Document49 pages1960Chris Gultiano100% (1)
- Settings, Methods, and Tools of Social WorkDocument8 pagesSettings, Methods, and Tools of Social WorkAvishanks Dluffyace Guyao100% (3)
- PrednisoloneDocument2 pagesPrednisoloneKatie McPeekNo ratings yet
- Drug StudyDocument4 pagesDrug StudyKristine Young100% (1)
- Prescribed Medication: Information Leaflet PriorDocument4 pagesPrescribed Medication: Information Leaflet PriorHavier EsparagueraNo ratings yet
- Drug Study (Omeprazole)Document2 pagesDrug Study (Omeprazole)Baji ۦۦNo ratings yet
- PrednisoneDocument1 pagePrednisoneCassieNo ratings yet
- Drug StudyDocument9 pagesDrug StudyKAROL MARIAE LUZ ERESNo ratings yet
- Tapazole (Methimazole)Document2 pagesTapazole (Methimazole)CassieNo ratings yet
- Drug Study (Tramadol)Document1 pageDrug Study (Tramadol)Baji ۦۦNo ratings yet
- Evangelista Drug-StudyDocument15 pagesEvangelista Drug-Studydinglasanerica57No ratings yet
- She Drug StudyDocument23 pagesShe Drug StudyShella DechavezNo ratings yet
- Potential Complications:: Ruston Et Al., 2013)Document11 pagesPotential Complications:: Ruston Et Al., 2013)brianNo ratings yet
- Drugs 2Document6 pagesDrugs 2Elyse Ann ReyesNo ratings yet
- RosuvastatinDocument1 pageRosuvastatinJoshua KellyNo ratings yet
- Make A Drug Study On The Medications Given To JaneDocument2 pagesMake A Drug Study On The Medications Given To JaneYoko Mae YanoNo ratings yet
- Drug StudyDocument2 pagesDrug StudymaxynezolayvarNo ratings yet
- Lisinopril Drug StudyDocument2 pagesLisinopril Drug StudyKristinelou Marie Reyna100% (1)
- HI Drug Study - v.3Document13 pagesHI Drug Study - v.3Mary Claire AbenidoNo ratings yet
- Drug Study: Contraindicated in Patients With Systemic Fungal Infection, Who Are Taking Mifepristone and HypersensitivityDocument3 pagesDrug Study: Contraindicated in Patients With Systemic Fungal Infection, Who Are Taking Mifepristone and HypersensitivityJoy SaavedraNo ratings yet
- Drug-Study-Form (Valencia)Document4 pagesDrug-Study-Form (Valencia)Kei ValenciaNo ratings yet
- DRUG STUDY 2023 WARD POTASSIUM CHLORIDE AutosavedDocument2 pagesDRUG STUDY 2023 WARD POTASSIUM CHLORIDE AutosavedMary Grace AgataNo ratings yet
- Drug Study EntecavirDocument4 pagesDrug Study EntecavirClarimae AwingNo ratings yet
- Drug Study - LosartanDocument2 pagesDrug Study - LosartanCath Bril50% (2)
- CDU Care Plan. UTIDocument7 pagesCDU Care Plan. UTImutiso mutieNo ratings yet
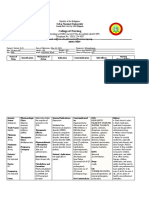
- College of Nursing: The Health Sciences CenterDocument3 pagesCollege of Nursing: The Health Sciences CenterAna Luisa Conejos ConeseNo ratings yet
- Drug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeDocument8 pagesDrug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeAngel Gaddi LarenaNo ratings yet
- Tamoxifen NolvadexDocument1 pageTamoxifen NolvadexAdrianne Bazo100% (1)
- Drug Study ParacetamolDocument2 pagesDrug Study ParacetamolDannah BulliandayNo ratings yet
- NURS 1566 Clinical Form 3: Clinical Medications WorksheetsDocument2 pagesNURS 1566 Clinical Form 3: Clinical Medications Worksheetsm_r0se_k0hNo ratings yet
- Generic:: Drug Study #1Document1 pageGeneric:: Drug Study #1Patricia Jean FaeldoneaNo ratings yet
- V. Atypical AntidepressantsDocument2 pagesV. Atypical AntidepressantsChristine Pialan SalimbagatNo ratings yet
- Predacot PrednisoneDocument1 pagePredacot PrednisoneAdrianne BazoNo ratings yet
- Predacot PrednisoneDocument1 pagePredacot PrednisoneAdrianne BazoNo ratings yet
- Volvulus GROUP 4Document7 pagesVolvulus GROUP 41S VILLEGAS GabrielNo ratings yet
- Drug Study - Magnesium SulfateDocument6 pagesDrug Study - Magnesium SulfatePrincess Alane MorenoNo ratings yet
- Drug StudyDocument13 pagesDrug Studyapi-3757116100% (4)
- NCM107 Lab Drug Study Manalo BSN 2BDocument4 pagesNCM107 Lab Drug Study Manalo BSN 2BBethrice MelegritoNo ratings yet
- Drug Study - Aling MaritesDocument1 pageDrug Study - Aling MaritesAbbyNo ratings yet
- Drug StudyDocument5 pagesDrug StudyMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Methylprednisolone (Solu Medrol)Document3 pagesMethylprednisolone (Solu Medrol)Adrianne Bazo100% (1)
- NewcardiooooDocument32 pagesNewcardiooooCharlene RojasNo ratings yet
- NCP Impaired Swallowing Ward 2023Document5 pagesNCP Impaired Swallowing Ward 2023Mary Grace AgataNo ratings yet
- Strumazol Strong Iodine SolutionDocument5 pagesStrumazol Strong Iodine SolutionAisha MarieNo ratings yet
- Reactive - Arthritis - TextDocument2 pagesReactive - Arthritis - TextSathvika BNo ratings yet
- CortisoneDocument2 pagesCortisoneJulioNo ratings yet
- LocalDocument5 pagesLocalybqbjpvtmrNo ratings yet
- College of Nursing: Cebu Normal UniversityDocument11 pagesCollege of Nursing: Cebu Normal Universityvivi's eyebrowsNo ratings yet
- DS 7Document1 pageDS 7Aichal HmjNo ratings yet
- Solu-Cortef (Hydrocortisone)Document3 pagesSolu-Cortef (Hydrocortisone)E100% (2)
- PrimidoneDocument6 pagesPrimidoneKim SunooNo ratings yet
- Rheumatoid Arthritis Drug StudyDocument2 pagesRheumatoid Arthritis Drug StudyChristaNo ratings yet
- Magnesium SulfateDocument6 pagesMagnesium SulfatePrincess Alane MorenoNo ratings yet
- Why Drugs and Vaccines Don't Work: The Science behind Natural Healing, and the Fraud behind Mainstream HealthcareFrom EverandWhy Drugs and Vaccines Don't Work: The Science behind Natural Healing, and the Fraud behind Mainstream HealthcareNo ratings yet
- Chronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsFrom EverandChronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsNo ratings yet
- Why Use Natural Healing: A Comparison of the Science and Efficacy of Natural Healing with That of PharmaceuticalsFrom EverandWhy Use Natural Healing: A Comparison of the Science and Efficacy of Natural Healing with That of PharmaceuticalsNo ratings yet
- Activity 1 RIZAL LAW A DEBATEDocument1 pageActivity 1 RIZAL LAW A DEBATEKimberly Claire DegalaNo ratings yet
- Activity 2. GANITO KAMI NOON PAANO KAYO NGAYONDocument4 pagesActivity 2. GANITO KAMI NOON PAANO KAYO NGAYONKimberly Claire DegalaNo ratings yet
- Assignment # 1Document2 pagesAssignment # 1Kimberly Claire DegalaNo ratings yet
- DEGALA-ACTIVITY Unit II THEORIES OF GENDERDocument3 pagesDEGALA-ACTIVITY Unit II THEORIES OF GENDERKimberly Claire DegalaNo ratings yet
- AssignmentDocument14 pagesAssignmentKimberly Claire DegalaNo ratings yet
- ParticipationDocument3 pagesParticipationSAA LOANSNo ratings yet
- Research Final Draft (Part2)Document28 pagesResearch Final Draft (Part2)Mae Colmenares100% (10)
- PHRM 821 Veterinary Pharmacy and Compounding Lab WorksheetDocument6 pagesPHRM 821 Veterinary Pharmacy and Compounding Lab Worksheetapi-381827675No ratings yet
- Original Article: Laparoscopic Inguinal Lymphadenectomy: A New Minimally Invasive Technique To Treat Vulva CarcinomaDocument6 pagesOriginal Article: Laparoscopic Inguinal Lymphadenectomy: A New Minimally Invasive Technique To Treat Vulva CarcinomaVlad GrigoreNo ratings yet
- A Comparative Study of Prison Systems in African Countries (O.A.Stephens, 2018)Document374 pagesA Comparative Study of Prison Systems in African Countries (O.A.Stephens, 2018)Razi MahriNo ratings yet
- Google LensDocument1 pageGoogle Lenstamo.chilingarashviliNo ratings yet
- Prosthodontics Book ListDocument3 pagesProsthodontics Book ListDentist Here100% (1)
- (Ariane) RESUME AND APPLICATION LETTERDocument4 pages(Ariane) RESUME AND APPLICATION LETTERmichelle ann sabilonaNo ratings yet
- Ls4 Elem Las21 To-Las50-MergedDocument31 pagesLs4 Elem Las21 To-Las50-MergedJaypee Aturo100% (2)
- The Management of Traumatic Brain Injury in Children: Opportunities For ActionDocument90 pagesThe Management of Traumatic Brain Injury in Children: Opportunities For ActionDR DAN PEZZULONo ratings yet
- Senate Hearing, 113TH Congress - The Bakken: Examining Efforts To Address Law Enforcement, Infrastructure and Economic Development NeedsDocument122 pagesSenate Hearing, 113TH Congress - The Bakken: Examining Efforts To Address Law Enforcement, Infrastructure and Economic Development NeedsScribd Government DocsNo ratings yet
- Pharmacy RTW 1 - OutlineDocument9 pagesPharmacy RTW 1 - OutlineKAREEM WAHEEDNo ratings yet
- Cristobal, Rocelyn P. MS Lec Post Task Triage FinalDocument10 pagesCristobal, Rocelyn P. MS Lec Post Task Triage FinalRocelyn CristobalNo ratings yet
- Infectious Diseases of The Gastrointestinal Tract: General InformationDocument9 pagesInfectious Diseases of The Gastrointestinal Tract: General InformationRichelle PadinNo ratings yet
- Hypertension and Congestive Heart FailureDocument4 pagesHypertension and Congestive Heart FailureDawn ReyaNo ratings yet
- Tax Case Compilation Ia To D 1Document19 pagesTax Case Compilation Ia To D 1Markonitchee Semper Fidelis100% (1)
- Safety Data Sheet ALUMON 5825 (QA) : 1. Identification of The Substance/Preparation and The CompanyDocument7 pagesSafety Data Sheet ALUMON 5825 (QA) : 1. Identification of The Substance/Preparation and The CompanyUtilities2No ratings yet
- Mobilna Protetika-PriručnikDocument150 pagesMobilna Protetika-PriručnikAleksandar Vukosav100% (1)
- Biochemistry by R.JDocument256 pagesBiochemistry by R.JDebajyoti DasNo ratings yet
- Anxiolytic DrugsDocument8 pagesAnxiolytic DrugsTony DawaNo ratings yet
- Fieldpro Smart Feeder: Om-264 234D ProcessesDocument52 pagesFieldpro Smart Feeder: Om-264 234D ProcessesReino Carlito Cordero GiroyNo ratings yet
- MI SlidesDocument65 pagesMI SlidesJobelyn TunayNo ratings yet
- EGR Carb Cleaner-English (UK & ROI)Document8 pagesEGR Carb Cleaner-English (UK & ROI)Youtube For EducationNo ratings yet
- Anemia of Chronic Disease in The ElderlyDocument7 pagesAnemia of Chronic Disease in The ElderlyAkbarNo ratings yet
- Carter Procession Closure MapDocument1 pageCarter Procession Closure Mapcookiespiffey21No ratings yet
- HR PoliciesDocument4 pagesHR PoliciesGanapati KattigeNo ratings yet