Download as pdf or txt
You might also like
- TKHMTC New Application FormDocument5 pagesTKHMTC New Application FormMbogi Toka100% (1)
- Pemeriksaan Kesihatan BiDocument3 pagesPemeriksaan Kesihatan BiWilson LimNo ratings yet
- Medical FormDocument3 pagesMedical FormkarashfordNo ratings yet
- Nursing Care Plan Formet (BEBO)Document15 pagesNursing Care Plan Formet (BEBO)Sumit chandNo ratings yet
- Occupational Health QuestionnaireDocument4 pagesOccupational Health QuestionnaireomnetaNo ratings yet
- Mediserve QLD Nurse Reg (Print)Document11 pagesMediserve QLD Nurse Reg (Print)Alex PiecesNo ratings yet
- 2021 Health QuestionnaireDocument3 pages2021 Health Questionnairemilksheikh2004No ratings yet
- Admission Letter JAN-SEPDocument9 pagesAdmission Letter JAN-SEPngethenjoro18No ratings yet
- Occupational Health (Health Screening Questionnaire)Document6 pagesOccupational Health (Health Screening Questionnaire)earl-e-birdNo ratings yet
- Medical BiodataDocument2 pagesMedical Biodataojowi.philpNo ratings yet
- 3.medical FormDocument5 pages3.medical Formamistudio30No ratings yet
- General Circular For MD October, 2022Document18 pagesGeneral Circular For MD October, 2022akhilNo ratings yet
- UoI Diploma Joining Instruction 2020 21Document4 pagesUoI Diploma Joining Instruction 2020 21Haason TzNo ratings yet
- Applications For Nursing PositionsDocument6 pagesApplications For Nursing PositionsNanaamma lipsyNo ratings yet
- Application For Admission For Academic Year 2019/2020 1. Proposed StudyDocument6 pagesApplication For Admission For Academic Year 2019/2020 1. Proposed StudyHumphrey ChisongelaNo ratings yet
- Faride Antonio OsmaneDocument4 pagesFaride Antonio OsmaneSamuel CarlitoNo ratings yet
- UoI Certificate Joining Instruction 2020 21Document4 pagesUoI Certificate Joining Instruction 2020 21Haason TzNo ratings yet
- Admissions Medical ApplicationDocument2 pagesAdmissions Medical ApplicationkesnaNo ratings yet
- Kaen University (Host Institution)Document4 pagesKaen University (Host Institution)Troy FengNo ratings yet
- Medical FormsDocument2 pagesMedical Formsgtws8fpnyzNo ratings yet
- Ayelign, Project WorkDocument27 pagesAyelign, Project WorkFiraafis LemmaNo ratings yet
- Registration Forms FoundationDocument3 pagesRegistration Forms FoundationArif ZaulkifleeNo ratings yet
- SLMC Regitration 2020Document3 pagesSLMC Regitration 2020vihari.shashiNo ratings yet
- Application Form IiiDocument6 pagesApplication Form IiibajomumbaseNo ratings yet
- Radiology Fellowships - Austin HealthDocument4 pagesRadiology Fellowships - Austin Healthsage masonNo ratings yet
- Updated Citizens Charter of FO XII 2023 7th EditionDocument137 pagesUpdated Citizens Charter of FO XII 2023 7th EditiondigakristinejoyNo ratings yet
- Medical ReportDocument5 pagesMedical ReportXYZNo ratings yet
- Teku Fomu ChetiDocument7 pagesTeku Fomu ChetiTone Radio-TzNo ratings yet
- 2011-2012 - Medical - DirectoryDocument112 pages2011-2012 - Medical - DirectoryЈелена КошевићNo ratings yet
- Aia Form 1 PDFDocument3 pagesAia Form 1 PDFVicky PascuaNo ratings yet
- Joaquim Jo BarbosaDocument4 pagesJoaquim Jo BarbosaMiguel Da PlacaNo ratings yet
- Care1st Medi Cal San DiegoDocument124 pagesCare1st Medi Cal San DiegotxgenicNo ratings yet
- Application Form For VolunteersDocument5 pagesApplication Form For Volunteersngan_ta2001No ratings yet
- School Personal Accident - Proposal FormDocument2 pagesSchool Personal Accident - Proposal FormDe KingmakerNo ratings yet
- Kibabii University Office of The Registrar (Academic Affairs) Entrance Medical Examination ImportantDocument4 pagesKibabii University Office of The Registrar (Academic Affairs) Entrance Medical Examination ImportantbrianlishinduNo ratings yet
- Faqs For The Agpt Program Entry in 2020: Current As at March 2019Document18 pagesFaqs For The Agpt Program Entry in 2020: Current As at March 2019kevin wangNo ratings yet
- Joining InstructionsDocument7 pagesJoining InstructionsDIGI TECHSNo ratings yet
- Application FormDocument8 pagesApplication FormMafruha AfrinNo ratings yet
- Request For Registration and License FormDocument3 pagesRequest For Registration and License FormTully MbogautwaNo ratings yet
- Health FormsDocument5 pagesHealth FormsRodolfo ArominNo ratings yet
- Application Form For Volunteers - Doc 1Document5 pagesApplication Form For Volunteers - Doc 1ngan_ta2001No ratings yet
- H14 09855 22 Medical FormDocument2 pagesH14 09855 22 Medical Formsalachjoseph24No ratings yet
- Schedule of Events-1Document3 pagesSchedule of Events-1Sri RhishiNo ratings yet
- Boitumelo Muyaya CVDocument5 pagesBoitumelo Muyaya CVbabesamarachi23No ratings yet
- 2012 Adult Medical FormDocument6 pages2012 Adult Medical FormRich WalterNo ratings yet
- DHA Medical FormDocument3 pagesDHA Medical FormSatish KapoorNo ratings yet
- Health Assessment FormDocument3 pagesHealth Assessment FormLau RenNo ratings yet
- Parental Consent Medical FormDocument2 pagesParental Consent Medical FormRonnie Valladores Jr.100% (1)
- Admissions Medical ApplicationDocument2 pagesAdmissions Medical ApplicationDajueNo ratings yet
- Tue Application FormDocument4 pagesTue Application FormHengky AntonNo ratings yet
- Application Form DPE 2022Document3 pagesApplication Form DPE 2022temogobosigo1No ratings yet
- MOTL Youth Medical FormDocument6 pagesMOTL Youth Medical FormRich WalterNo ratings yet
- Medical Certificate of AppDocument2 pagesMedical Certificate of AppRaju RajNo ratings yet
- Sri Lanka Medical Council: Coloured Photograph Photo Size 3.5 X 4. 5 CMDocument3 pagesSri Lanka Medical Council: Coloured Photograph Photo Size 3.5 X 4. 5 CMmani50No ratings yet
- MOrth Application Form May 2021Document3 pagesMOrth Application Form May 2021MINA GERGISNo ratings yet
- GAPP Application For A CaregiverDocument7 pagesGAPP Application For A Caregiverluwen357No ratings yet
- Unresolved Resources For ManoplasDocument2 pagesUnresolved Resources For Manoplasriderj601No ratings yet
- Breach of Duty of Care in Medical Negligence: Scope and LimitationDocument55 pagesBreach of Duty of Care in Medical Negligence: Scope and LimitationNaina Mathew100% (1)
- M Endo M Perio M Pros Exam Application FormDocument4 pagesM Endo M Perio M Pros Exam Application Formrugeaelzwea2No ratings yet
- The Health Workforce in Ethiopia: Addressing the Remaining ChallengesFrom EverandThe Health Workforce in Ethiopia: Addressing the Remaining ChallengesNo ratings yet
- Pistachio CultivarsDocument69 pagesPistachio CultivarsNzar HamaNo ratings yet
- The Opportunities of Lithium in Thermal Energy Storage: A State-Of-The-Art ReviewDocument24 pagesThe Opportunities of Lithium in Thermal Energy Storage: A State-Of-The-Art ReviewFrancisco DazaNo ratings yet
- 1 How Children Are Affected by Gender IssuesDocument5 pages1 How Children Are Affected by Gender IssuesElvis MontanodiaztanhuecopolvorizaNo ratings yet
- Allsec Compliance - Recent Labour Law Updates PDFDocument28 pagesAllsec Compliance - Recent Labour Law Updates PDFSureshNo ratings yet
- Management of Elective LaryngectomyDocument6 pagesManagement of Elective LaryngectomyKj BrionesNo ratings yet
- 2117 Barrons 1100 Words You Need To Know MCQ Test PDF Week 10 Day 4Document3 pages2117 Barrons 1100 Words You Need To Know MCQ Test PDF Week 10 Day 4Mohammed Al-misreNo ratings yet
- CAT Taurus 60Document2 pagesCAT Taurus 60Eyo EtimNo ratings yet
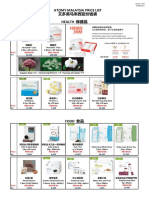
- Atomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Document6 pagesAtomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Lee Ling PengNo ratings yet
- Innes 1957Document2 pagesInnes 1957Magesh kumarNo ratings yet
- Description of HospitalDocument1 pageDescription of HospitalDanica Joy V. JacobaNo ratings yet
- Electrical Inspections ChecklistDocument6 pagesElectrical Inspections Checklistasyraf azaharyNo ratings yet
- Cefuroxime Drug StudyDocument2 pagesCefuroxime Drug StudyDanica Kate Galleon100% (1)
- (Download PDF) Calculus Early Transcendentals 3rd Edition Rogawski Solutions Manual Full ChapterDocument264 pages(Download PDF) Calculus Early Transcendentals 3rd Edition Rogawski Solutions Manual Full Chapterjadidbrmawi100% (5)
- KFTD Bengkulu 19 Februari 2021Document70 pagesKFTD Bengkulu 19 Februari 2021AINANo ratings yet
- Network Marketing Opportunity - Vestige Marketing Plan URTSAM - +919711572735Document16 pagesNetwork Marketing Opportunity - Vestige Marketing Plan URTSAM - +919711572735Samir K Mishra100% (1)
- Novavax VaccineDocument1 pageNovavax Vaccinealina JCNo ratings yet
- Lifting Operations Onboard ShipDocument3 pagesLifting Operations Onboard ShipGiorgi KandelakiNo ratings yet
- Public Area Cleaning - HousekeepingDocument14 pagesPublic Area Cleaning - HousekeepingPeter Adiputra0% (1)
- 816 2328 1 SM PDFDocument4 pages816 2328 1 SM PDFRahki BhatiNo ratings yet
- Outline PDF 06052024Document14 pagesOutline PDF 06052024Ryu SenaNo ratings yet
- Threat and Error ManagementDocument11 pagesThreat and Error ManagementmasonNo ratings yet
- TP2 24 AprilDocument12 pagesTP2 24 AprilAnaSlavovaNo ratings yet
- UNI T Catalogo 2022 1Document194 pagesUNI T Catalogo 2022 1Raúl Quintero MorenoNo ratings yet
- S1.01. Dental ErgonomicsDocument72 pagesS1.01. Dental ErgonomicsYasser Al WasifiNo ratings yet
- Employees Fps 1971Document22 pagesEmployees Fps 1971VasanthianbazhaganNo ratings yet
- Common Factors in PsychotherapyDocument11 pagesCommon Factors in Psychotherapydrc.psyNo ratings yet
- Name: - Section: - Date: - ScoreDocument4 pagesName: - Section: - Date: - ScoreBRENDEL SACARISNo ratings yet
- Highlights:: 2013 Falcon 2000LXS S/N 267/ N325APDocument6 pagesHighlights:: 2013 Falcon 2000LXS S/N 267/ N325APTesteArquivosNo ratings yet
- Adaptation CardsDocument17 pagesAdaptation CardsNubar MammadovaNo ratings yet
- Career Planning and DevelopmentDocument12 pagesCareer Planning and DevelopmentbushraNo ratings yet