
Obstetric History and Physical Examination (Ina Irabon)
Obstetric History and Physical Examination (Ina Irabon)
You might also like
- TEST BANK For Pediatric Nursing - A Case-Based Approach, 2nd Edition by (Tagher, 2024), Verified Chapters 1 - 34, Complete Newest VersionDocument55 pagesTEST BANK For Pediatric Nursing - A Case-Based Approach, 2nd Edition by (Tagher, 2024), Verified Chapters 1 - 34, Complete Newest Versionkevinkariuki227No ratings yet
- Kerr, Michael E - One Family's Story-A Primer On Bowen TheoryDocument23 pagesKerr, Michael E - One Family's Story-A Primer On Bowen Theoryhabermaniac75% (4)
- Textbook Ebook Foundations of Maternal Newborn and Womens Health Nursing Seventh Edition Sharon Smith Murray All Chapter PDFDocument43 pagesTextbook Ebook Foundations of Maternal Newborn and Womens Health Nursing Seventh Edition Sharon Smith Murray All Chapter PDFrichard.barr601100% (6)
- GuidelineDocument7 pagesGuidelinebelvacute0% (2)
- POGS PB Dystocia Sept 2022Document6 pagesPOGS PB Dystocia Sept 2022John Piox Badiang100% (1)
- KRA 1. Maternal, Neonatal, Child Health and Nutrition (MNCHN)Document7 pagesKRA 1. Maternal, Neonatal, Child Health and Nutrition (MNCHN)Tmo BosNo ratings yet
- SOGP AnaemiaDocument16 pagesSOGP AnaemiaMuhammad Farrukh ul IslamNo ratings yet
- GTDDocument56 pagesGTDRendy Adhitya PratamaNo ratings yet
- Topic 7 - Volunteerism Module 1Document9 pagesTopic 7 - Volunteerism Module 1Benjamin GabrielNo ratings yet
- Advanced Pediatric AssessmentDocument582 pagesAdvanced Pediatric AssessmentBenjamin Gabriel100% (1)
- 1) Benign Gynecologic Lesions - FINALDocument121 pages1) Benign Gynecologic Lesions - FINALJed Mostajo100% (1)
- OB - Normal Labor and DeliveryDocument51 pagesOB - Normal Labor and DeliveryJosh Matthew Rosales33% (3)
- Gyne Onco Interns NotesDocument54 pagesGyne Onco Interns NotesCoy NuñezNo ratings yet
- I. Dystocia: A. CausesDocument9 pagesI. Dystocia: A. CausesDianne GalangNo ratings yet
- 2 - Antenatal CareDocument44 pages2 - Antenatal CareJordanBangot50% (2)
- OB Gyne Clinical and Teaching CasesDocument221 pagesOB Gyne Clinical and Teaching CaseszzNo ratings yet
- Asthma in PregnancyDocument40 pagesAsthma in PregnancyKabo75% (4)
- Maternal Child Nursing (MCN) PDFDocument94 pagesMaternal Child Nursing (MCN) PDFirene8000No ratings yet
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- Gyne - Feu ReviewerDocument87 pagesGyne - Feu ReviewerKoko RoqueNo ratings yet
- Screening: Pogs CPG Guideline SDocument2 pagesScreening: Pogs CPG Guideline SNica Lopez FernandezNo ratings yet
- Hypertensive Disorders in Pregnancy (Williams 22 Edition)Document88 pagesHypertensive Disorders in Pregnancy (Williams 22 Edition)bagir_dm1067% (3)
- CPG Labor and Delivery 2015Document78 pagesCPG Labor and Delivery 2015TintalleNo ratings yet
- Obgyn Revalida Review 2022 RcsDocument248 pagesObgyn Revalida Review 2022 RcsSophia SaquilayanNo ratings yet
- Finals QuestionsDocument10 pagesFinals QuestionsBobet ReñaNo ratings yet
- Trans-Out Orders: NSVD Admitting Notes Postpartum OrdersDocument7 pagesTrans-Out Orders: NSVD Admitting Notes Postpartum OrdersDre ValdezNo ratings yet
- FInal Anemia in PregnancyDocument57 pagesFInal Anemia in PregnancyAiszel Angeli Pepito LigoNo ratings yet
- Pathologic Obstetrics Board Review RedDocument72 pagesPathologic Obstetrics Board Review RedNicole Santos100% (1)
- OB 1.01 DystociaDocument9 pagesOB 1.01 DystociaRaquel Reyes100% (1)
- Module 6 - Benign Gynecologic TumorsDocument9 pagesModule 6 - Benign Gynecologic TumorsRenz Francis SasaNo ratings yet
- Case Protocol SampleDocument1 pageCase Protocol SampleMarco Paulo Reyes NaoeNo ratings yet
- OB & GyneDocument24 pagesOB & GyneJohn Christopher LucesNo ratings yet
- FAMILY PLANNING - CEU Medicine Lecture Trans (Gynecology)Document7 pagesFAMILY PLANNING - CEU Medicine Lecture Trans (Gynecology)Ian Christopher RochaNo ratings yet
- O and G Notes Notebank NumberedDocument173 pagesO and G Notes Notebank NumberedPerscitus Ali القحطانيNo ratings yet
- OB - TransesDocument112 pagesOB - TransesAldwin BagtasNo ratings yet
- Ectopic Pregnancy FINALDocument32 pagesEctopic Pregnancy FINALZak KazNo ratings yet
- Pedia Lecture 1-b Preventive Healthcare in Pediatrics TransDocument10 pagesPedia Lecture 1-b Preventive Healthcare in Pediatrics TransRemelou Garchitorena AlfelorNo ratings yet
- OBGYNE Must-KnowsDocument10 pagesOBGYNE Must-KnowsPigwet KwisNo ratings yet
- Sensory ExaminationDocument4 pagesSensory ExaminationAthena BorjaNo ratings yet
- CC Silva - Rationalization 2022: # Rationale Answer: C. Contained in The Vestibule RationaleDocument34 pagesCC Silva - Rationalization 2022: # Rationale Answer: C. Contained in The Vestibule RationaleNicole Xyza JunsayNo ratings yet
- TOPNOTCH Ob-Gyne Supplement Handout by Joan Cabanting and Nina Banzuela - UPDATED DECEMBER 2017 PDFDocument27 pagesTOPNOTCH Ob-Gyne Supplement Handout by Joan Cabanting and Nina Banzuela - UPDATED DECEMBER 2017 PDFWaiwit KritayakiranaNo ratings yet
- 11.23b-Conduct of Normal Labor and DeliveryDocument8 pages11.23b-Conduct of Normal Labor and DeliveryJøshua Cruz100% (2)
- Who Par To GraphDocument59 pagesWho Par To GraphHandri Rezki VebrianNo ratings yet
- Prenatal Care FINALDocument94 pagesPrenatal Care FINALAngela SaldajenoNo ratings yet
- OSCE Revision OBG DocumentDocument60 pagesOSCE Revision OBG DocumentshreyaNo ratings yet
- C. Anovulation: C. Dysfunctional Uterine BleedingDocument18 pagesC. Anovulation: C. Dysfunctional Uterine BleedingJan Mikhail Frasco100% (1)
- CPG On Normal Labor and DeliveryDocument59 pagesCPG On Normal Labor and DeliveryHedy Suico Galela - Racines100% (2)
- Oral and Parenteral Iron Preparations in PregnancyDocument45 pagesOral and Parenteral Iron Preparations in PregnancyArun George100% (3)
- Physical Examination For Pregnant WomanDocument31 pagesPhysical Examination For Pregnant WomanFrancia ToledanoNo ratings yet
- Do Cervical Cancer Screening Recommendations Differ Among Women at Different Age Groups?Document8 pagesDo Cervical Cancer Screening Recommendations Differ Among Women at Different Age Groups?Nico Angelo CopoNo ratings yet
- OB Med Order KodigsDocument1 pageOB Med Order KodigsfloramaeyecyecNo ratings yet
- Hypertension in Pregnancy (Pogs-Cpg)Document60 pagesHypertension in Pregnancy (Pogs-Cpg)Ivy Combista Baya100% (1)
- History TakingDocument3 pagesHistory Takingmkct111100% (1)
- OB-Reviewer With AlgorithmDocument29 pagesOB-Reviewer With Algorithmriczen mae vilaNo ratings yet
- OB MustKnowsDocument90 pagesOB MustKnowsHarlyn MagsinoNo ratings yet
- Pregnancy Induced HypertensionDocument52 pagesPregnancy Induced HypertensionJoy GloryNo ratings yet
- SGOP 2008 (Guidelines On Management)Document87 pagesSGOP 2008 (Guidelines On Management)Via Alip100% (1)
- High Risk PregnancyDocument42 pagesHigh Risk PregnancyLisa KriestantoNo ratings yet
- Surgery Ple ReviewerDocument5 pagesSurgery Ple ReviewerReinhard Ivan MansibangNo ratings yet
- (Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringDocument8 pages(Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringKim RamosNo ratings yet
- Ob SGDDocument88 pagesOb SGDFerdinand Luis SuarezNo ratings yet
- ACOG Practice Bulletin On Thyroid Disease in PregnancyDocument5 pagesACOG Practice Bulletin On Thyroid Disease in Pregnancygenerics54321No ratings yet
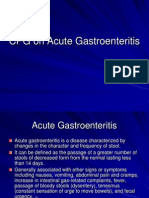
- CPG On Acute GastroenteritisDocument24 pagesCPG On Acute GastroenteritisAbegail Fermanejo-Generao100% (1)
- Ob Supplement Handout by DR - Chris SorianoDocument33 pagesOb Supplement Handout by DR - Chris SorianoHedley Chua75% (4)
- Page 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFDocument5 pagesPage 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFfitrah fajrianiNo ratings yet
- Obg Extra EdgeDocument201 pagesObg Extra EdgeabhishekbmcNo ratings yet
- History and PEDocument3 pagesHistory and PEBom TnaNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2Rating: 5 out of 5 stars5/5 (1)
- Obstetric HistoryDocument38 pagesObstetric HistoryHannah LeianNo ratings yet
- Community Health NursingDocument98 pagesCommunity Health NursingBenjamin GabrielNo ratings yet
- STS Instructional Modules Week 15a 2Document8 pagesSTS Instructional Modules Week 15a 2Benjamin GabrielNo ratings yet
- Communicable Diseases PresentationDocument225 pagesCommunicable Diseases PresentationBenjamin GabrielNo ratings yet
- Baroma Regina SalveDocument56 pagesBaroma Regina SalveBenjamin GabrielNo ratings yet
- How To Collect A Urine Sample From Babies: ImportantDocument2 pagesHow To Collect A Urine Sample From Babies: ImportantBenjamin GabrielNo ratings yet
- Age of Gestation: First TrimesterDocument4 pagesAge of Gestation: First TrimesterBenjamin GabrielNo ratings yet
- Maneuver Used in Delivery of FetusDocument1 pageManeuver Used in Delivery of FetusBenjamin GabrielNo ratings yet
- Info GraphicDocument1 pageInfo GraphicBenjamin GabrielNo ratings yet
- Module 1 Citizenship Training For Online and OfflineDocument17 pagesModule 1 Citizenship Training For Online and OfflineBenjamin GabrielNo ratings yet
- Terms of Pregnancy (C SU07)Document4 pagesTerms of Pregnancy (C SU07)عبدالرحمن الزيودNo ratings yet
- The Ethics of Perinatal Care For Black WomenDocument8 pagesThe Ethics of Perinatal Care For Black Womenapi-625120170No ratings yet
- Medstar ObGyn 2nd EditionDocument570 pagesMedstar ObGyn 2nd EditionMerahit Abera100% (2)
- Conversation Midwife With Patient On Examination PregnancyDocument5 pagesConversation Midwife With Patient On Examination Pregnancyachy chanNo ratings yet
- Antenatal CareDocument19 pagesAntenatal CareIshika RoyNo ratings yet
- Jurnal KebidananDocument12 pagesJurnal KebidananhanaNo ratings yet
- Programme Outcome B.Sc. Nursing CourseDocument7 pagesProgramme Outcome B.Sc. Nursing CoursePreeti ChouhanNo ratings yet
- Cardiac & Respiratory Diseases in PregnancyDocument30 pagesCardiac & Respiratory Diseases in PregnancyKerod AbebeNo ratings yet
- NCLEX Questions OB QuestionsDocument4 pagesNCLEX Questions OB QuestionsAlvin L. Rozier100% (1)
- Coffey vs. Murrumbidgee Local Health DistrictDocument83 pagesCoffey vs. Murrumbidgee Local Health DistrictToby VueNo ratings yet
- Health Talk TopicsDocument3 pagesHealth Talk Topicsvarshasharma0562% (13)
- 48.pelvic RockingDocument6 pages48.pelvic RockingRani MarianaNo ratings yet
- Literature Review Low Birth WeightDocument4 pagesLiterature Review Low Birth Weightc5qx9hq5100% (1)
- Inter-Hospital Variations in Labor Induction and OutcomesDocument9 pagesInter-Hospital Variations in Labor Induction and OutcomesStéphanieNo ratings yet
- Incomplete AbortionDocument18 pagesIncomplete AbortionAra DirganNo ratings yet
- Oxytocin Hormone Benefits and Side Effects by Ray SahelianDocument5 pagesOxytocin Hormone Benefits and Side Effects by Ray SahelianCondor7tNo ratings yet
- Margaret Jackson Prize Essay 2000 What's So Bad About Teenage Pregnancy?Document7 pagesMargaret Jackson Prize Essay 2000 What's So Bad About Teenage Pregnancy?Avela KwazaNo ratings yet
- Treatment of Pregnancy-Related Lumbar and Pelvic Girdle Pain by The Yoga Method: A Randomized Controlled StudyDocument8 pagesTreatment of Pregnancy-Related Lumbar and Pelvic Girdle Pain by The Yoga Method: A Randomized Controlled StudyJosephineeNo ratings yet
- NCP - Diabetes Mellitus Prepregnancy/GestationalDocument13 pagesNCP - Diabetes Mellitus Prepregnancy/GestationalClaudine Christophe100% (1)
- PNLE NCLEX Practice Exam For Maternal and Child Health Nursing 2Document5 pagesPNLE NCLEX Practice Exam For Maternal and Child Health Nursing 2bobtaguba100% (1)
- Phisiological Changes Due To PregnancyDocument21 pagesPhisiological Changes Due To PregnancyVijith.V.kumarNo ratings yet
- Saint Louis University School of Nursing Nutrition LectureDocument9 pagesSaint Louis University School of Nursing Nutrition LectureShaina Fe RabaneraNo ratings yet
- #4 - NCM 109 - TransesDocument22 pages#4 - NCM 109 - TransesJaimie BanaagNo ratings yet



































































































Download as pdf or txt
You might also like
- TEST BANK For Pediatric Nursing - A Case-Based Approach, 2nd Edition by (Tagher, 2024), Verified Chapters 1 - 34, Complete Newest VersionDocument55 pagesTEST BANK For Pediatric Nursing - A Case-Based Approach, 2nd Edition by (Tagher, 2024), Verified Chapters 1 - 34, Complete Newest Versionkevinkariuki227No ratings yet
- Kerr, Michael E - One Family's Story-A Primer On Bowen TheoryDocument23 pagesKerr, Michael E - One Family's Story-A Primer On Bowen Theoryhabermaniac75% (4)
- Textbook Ebook Foundations of Maternal Newborn and Womens Health Nursing Seventh Edition Sharon Smith Murray All Chapter PDFDocument43 pagesTextbook Ebook Foundations of Maternal Newborn and Womens Health Nursing Seventh Edition Sharon Smith Murray All Chapter PDFrichard.barr601100% (6)
- GuidelineDocument7 pagesGuidelinebelvacute0% (2)
- POGS PB Dystocia Sept 2022Document6 pagesPOGS PB Dystocia Sept 2022John Piox Badiang100% (1)
- KRA 1. Maternal, Neonatal, Child Health and Nutrition (MNCHN)Document7 pagesKRA 1. Maternal, Neonatal, Child Health and Nutrition (MNCHN)Tmo BosNo ratings yet
- SOGP AnaemiaDocument16 pagesSOGP AnaemiaMuhammad Farrukh ul IslamNo ratings yet
- GTDDocument56 pagesGTDRendy Adhitya PratamaNo ratings yet
- Topic 7 - Volunteerism Module 1Document9 pagesTopic 7 - Volunteerism Module 1Benjamin GabrielNo ratings yet
- Advanced Pediatric AssessmentDocument582 pagesAdvanced Pediatric AssessmentBenjamin Gabriel100% (1)
- 1) Benign Gynecologic Lesions - FINALDocument121 pages1) Benign Gynecologic Lesions - FINALJed Mostajo100% (1)
- OB - Normal Labor and DeliveryDocument51 pagesOB - Normal Labor and DeliveryJosh Matthew Rosales33% (3)
- Gyne Onco Interns NotesDocument54 pagesGyne Onco Interns NotesCoy NuñezNo ratings yet
- I. Dystocia: A. CausesDocument9 pagesI. Dystocia: A. CausesDianne GalangNo ratings yet
- 2 - Antenatal CareDocument44 pages2 - Antenatal CareJordanBangot50% (2)
- OB Gyne Clinical and Teaching CasesDocument221 pagesOB Gyne Clinical and Teaching CaseszzNo ratings yet
- Asthma in PregnancyDocument40 pagesAsthma in PregnancyKabo75% (4)
- Maternal Child Nursing (MCN) PDFDocument94 pagesMaternal Child Nursing (MCN) PDFirene8000No ratings yet
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- Gyne - Feu ReviewerDocument87 pagesGyne - Feu ReviewerKoko RoqueNo ratings yet
- Screening: Pogs CPG Guideline SDocument2 pagesScreening: Pogs CPG Guideline SNica Lopez FernandezNo ratings yet
- Hypertensive Disorders in Pregnancy (Williams 22 Edition)Document88 pagesHypertensive Disorders in Pregnancy (Williams 22 Edition)bagir_dm1067% (3)
- CPG Labor and Delivery 2015Document78 pagesCPG Labor and Delivery 2015TintalleNo ratings yet
- Obgyn Revalida Review 2022 RcsDocument248 pagesObgyn Revalida Review 2022 RcsSophia SaquilayanNo ratings yet
- Finals QuestionsDocument10 pagesFinals QuestionsBobet ReñaNo ratings yet
- Trans-Out Orders: NSVD Admitting Notes Postpartum OrdersDocument7 pagesTrans-Out Orders: NSVD Admitting Notes Postpartum OrdersDre ValdezNo ratings yet
- FInal Anemia in PregnancyDocument57 pagesFInal Anemia in PregnancyAiszel Angeli Pepito LigoNo ratings yet
- Pathologic Obstetrics Board Review RedDocument72 pagesPathologic Obstetrics Board Review RedNicole Santos100% (1)
- OB 1.01 DystociaDocument9 pagesOB 1.01 DystociaRaquel Reyes100% (1)
- Module 6 - Benign Gynecologic TumorsDocument9 pagesModule 6 - Benign Gynecologic TumorsRenz Francis SasaNo ratings yet
- Case Protocol SampleDocument1 pageCase Protocol SampleMarco Paulo Reyes NaoeNo ratings yet
- OB & GyneDocument24 pagesOB & GyneJohn Christopher LucesNo ratings yet
- FAMILY PLANNING - CEU Medicine Lecture Trans (Gynecology)Document7 pagesFAMILY PLANNING - CEU Medicine Lecture Trans (Gynecology)Ian Christopher RochaNo ratings yet
- O and G Notes Notebank NumberedDocument173 pagesO and G Notes Notebank NumberedPerscitus Ali القحطانيNo ratings yet
- OB - TransesDocument112 pagesOB - TransesAldwin BagtasNo ratings yet
- Ectopic Pregnancy FINALDocument32 pagesEctopic Pregnancy FINALZak KazNo ratings yet
- Pedia Lecture 1-b Preventive Healthcare in Pediatrics TransDocument10 pagesPedia Lecture 1-b Preventive Healthcare in Pediatrics TransRemelou Garchitorena AlfelorNo ratings yet
- OBGYNE Must-KnowsDocument10 pagesOBGYNE Must-KnowsPigwet KwisNo ratings yet
- Sensory ExaminationDocument4 pagesSensory ExaminationAthena BorjaNo ratings yet
- CC Silva - Rationalization 2022: # Rationale Answer: C. Contained in The Vestibule RationaleDocument34 pagesCC Silva - Rationalization 2022: # Rationale Answer: C. Contained in The Vestibule RationaleNicole Xyza JunsayNo ratings yet
- TOPNOTCH Ob-Gyne Supplement Handout by Joan Cabanting and Nina Banzuela - UPDATED DECEMBER 2017 PDFDocument27 pagesTOPNOTCH Ob-Gyne Supplement Handout by Joan Cabanting and Nina Banzuela - UPDATED DECEMBER 2017 PDFWaiwit KritayakiranaNo ratings yet
- 11.23b-Conduct of Normal Labor and DeliveryDocument8 pages11.23b-Conduct of Normal Labor and DeliveryJøshua Cruz100% (2)
- Who Par To GraphDocument59 pagesWho Par To GraphHandri Rezki VebrianNo ratings yet
- Prenatal Care FINALDocument94 pagesPrenatal Care FINALAngela SaldajenoNo ratings yet
- OSCE Revision OBG DocumentDocument60 pagesOSCE Revision OBG DocumentshreyaNo ratings yet
- C. Anovulation: C. Dysfunctional Uterine BleedingDocument18 pagesC. Anovulation: C. Dysfunctional Uterine BleedingJan Mikhail Frasco100% (1)
- CPG On Normal Labor and DeliveryDocument59 pagesCPG On Normal Labor and DeliveryHedy Suico Galela - Racines100% (2)
- Oral and Parenteral Iron Preparations in PregnancyDocument45 pagesOral and Parenteral Iron Preparations in PregnancyArun George100% (3)
- Physical Examination For Pregnant WomanDocument31 pagesPhysical Examination For Pregnant WomanFrancia ToledanoNo ratings yet
- Do Cervical Cancer Screening Recommendations Differ Among Women at Different Age Groups?Document8 pagesDo Cervical Cancer Screening Recommendations Differ Among Women at Different Age Groups?Nico Angelo CopoNo ratings yet
- OB Med Order KodigsDocument1 pageOB Med Order KodigsfloramaeyecyecNo ratings yet
- Hypertension in Pregnancy (Pogs-Cpg)Document60 pagesHypertension in Pregnancy (Pogs-Cpg)Ivy Combista Baya100% (1)
- History TakingDocument3 pagesHistory Takingmkct111100% (1)
- OB-Reviewer With AlgorithmDocument29 pagesOB-Reviewer With Algorithmriczen mae vilaNo ratings yet
- OB MustKnowsDocument90 pagesOB MustKnowsHarlyn MagsinoNo ratings yet
- Pregnancy Induced HypertensionDocument52 pagesPregnancy Induced HypertensionJoy GloryNo ratings yet
- SGOP 2008 (Guidelines On Management)Document87 pagesSGOP 2008 (Guidelines On Management)Via Alip100% (1)
- High Risk PregnancyDocument42 pagesHigh Risk PregnancyLisa KriestantoNo ratings yet
- Surgery Ple ReviewerDocument5 pagesSurgery Ple ReviewerReinhard Ivan MansibangNo ratings yet
- (Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringDocument8 pages(Ob) - 4s-1-Antepartum Surveillance and Intrapartum MonitoringKim RamosNo ratings yet
- Ob SGDDocument88 pagesOb SGDFerdinand Luis SuarezNo ratings yet
- ACOG Practice Bulletin On Thyroid Disease in PregnancyDocument5 pagesACOG Practice Bulletin On Thyroid Disease in Pregnancygenerics54321No ratings yet
- CPG On Acute GastroenteritisDocument24 pagesCPG On Acute GastroenteritisAbegail Fermanejo-Generao100% (1)
- Ob Supplement Handout by DR - Chris SorianoDocument33 pagesOb Supplement Handout by DR - Chris SorianoHedley Chua75% (4)
- Page 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFDocument5 pagesPage 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFfitrah fajrianiNo ratings yet
- Obg Extra EdgeDocument201 pagesObg Extra EdgeabhishekbmcNo ratings yet
- History and PEDocument3 pagesHistory and PEBom TnaNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2Rating: 5 out of 5 stars5/5 (1)
- Obstetric HistoryDocument38 pagesObstetric HistoryHannah LeianNo ratings yet
- Community Health NursingDocument98 pagesCommunity Health NursingBenjamin GabrielNo ratings yet
- STS Instructional Modules Week 15a 2Document8 pagesSTS Instructional Modules Week 15a 2Benjamin GabrielNo ratings yet
- Communicable Diseases PresentationDocument225 pagesCommunicable Diseases PresentationBenjamin GabrielNo ratings yet
- Baroma Regina SalveDocument56 pagesBaroma Regina SalveBenjamin GabrielNo ratings yet
- How To Collect A Urine Sample From Babies: ImportantDocument2 pagesHow To Collect A Urine Sample From Babies: ImportantBenjamin GabrielNo ratings yet
- Age of Gestation: First TrimesterDocument4 pagesAge of Gestation: First TrimesterBenjamin GabrielNo ratings yet
- Maneuver Used in Delivery of FetusDocument1 pageManeuver Used in Delivery of FetusBenjamin GabrielNo ratings yet
- Info GraphicDocument1 pageInfo GraphicBenjamin GabrielNo ratings yet
- Module 1 Citizenship Training For Online and OfflineDocument17 pagesModule 1 Citizenship Training For Online and OfflineBenjamin GabrielNo ratings yet
- Terms of Pregnancy (C SU07)Document4 pagesTerms of Pregnancy (C SU07)عبدالرحمن الزيودNo ratings yet
- The Ethics of Perinatal Care For Black WomenDocument8 pagesThe Ethics of Perinatal Care For Black Womenapi-625120170No ratings yet
- Medstar ObGyn 2nd EditionDocument570 pagesMedstar ObGyn 2nd EditionMerahit Abera100% (2)
- Conversation Midwife With Patient On Examination PregnancyDocument5 pagesConversation Midwife With Patient On Examination Pregnancyachy chanNo ratings yet
- Antenatal CareDocument19 pagesAntenatal CareIshika RoyNo ratings yet
- Jurnal KebidananDocument12 pagesJurnal KebidananhanaNo ratings yet
- Programme Outcome B.Sc. Nursing CourseDocument7 pagesProgramme Outcome B.Sc. Nursing CoursePreeti ChouhanNo ratings yet
- Cardiac & Respiratory Diseases in PregnancyDocument30 pagesCardiac & Respiratory Diseases in PregnancyKerod AbebeNo ratings yet
- NCLEX Questions OB QuestionsDocument4 pagesNCLEX Questions OB QuestionsAlvin L. Rozier100% (1)
- Coffey vs. Murrumbidgee Local Health DistrictDocument83 pagesCoffey vs. Murrumbidgee Local Health DistrictToby VueNo ratings yet
- Health Talk TopicsDocument3 pagesHealth Talk Topicsvarshasharma0562% (13)
- 48.pelvic RockingDocument6 pages48.pelvic RockingRani MarianaNo ratings yet
- Literature Review Low Birth WeightDocument4 pagesLiterature Review Low Birth Weightc5qx9hq5100% (1)
- Inter-Hospital Variations in Labor Induction and OutcomesDocument9 pagesInter-Hospital Variations in Labor Induction and OutcomesStéphanieNo ratings yet
- Incomplete AbortionDocument18 pagesIncomplete AbortionAra DirganNo ratings yet
- Oxytocin Hormone Benefits and Side Effects by Ray SahelianDocument5 pagesOxytocin Hormone Benefits and Side Effects by Ray SahelianCondor7tNo ratings yet
- Margaret Jackson Prize Essay 2000 What's So Bad About Teenage Pregnancy?Document7 pagesMargaret Jackson Prize Essay 2000 What's So Bad About Teenage Pregnancy?Avela KwazaNo ratings yet
- Treatment of Pregnancy-Related Lumbar and Pelvic Girdle Pain by The Yoga Method: A Randomized Controlled StudyDocument8 pagesTreatment of Pregnancy-Related Lumbar and Pelvic Girdle Pain by The Yoga Method: A Randomized Controlled StudyJosephineeNo ratings yet
- NCP - Diabetes Mellitus Prepregnancy/GestationalDocument13 pagesNCP - Diabetes Mellitus Prepregnancy/GestationalClaudine Christophe100% (1)
- PNLE NCLEX Practice Exam For Maternal and Child Health Nursing 2Document5 pagesPNLE NCLEX Practice Exam For Maternal and Child Health Nursing 2bobtaguba100% (1)
- Phisiological Changes Due To PregnancyDocument21 pagesPhisiological Changes Due To PregnancyVijith.V.kumarNo ratings yet
- Saint Louis University School of Nursing Nutrition LectureDocument9 pagesSaint Louis University School of Nursing Nutrition LectureShaina Fe RabaneraNo ratings yet
- #4 - NCM 109 - TransesDocument22 pages#4 - NCM 109 - TransesJaimie BanaagNo ratings yet