
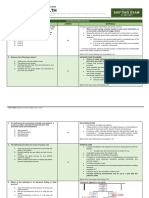
Sample:: Based On The HPI Alone, The Physician Should Already Have An Initial Impression and Differential Diagnosis
Sample:: Based On The HPI Alone, The Physician Should Already Have An Initial Impression and Differential Diagnosis
You might also like
- Hydrocarbons Worksheet AnswersDocument2 pagesHydrocarbons Worksheet AnswersNorman Vryne Cadua100% (1)
- Vet Clin Procedures - Large Animal History TakingDocument7 pagesVet Clin Procedures - Large Animal History TakinglechamariaNo ratings yet
- Pediatric HX and PEDocument8 pagesPediatric HX and PEsahani100% (2)
- Pediatric History & Physical ExamDocument5 pagesPediatric History & Physical ExamLloyd Jay Lin100% (2)
- Physical Therapy Initial Evaluation GUIDEDocument152 pagesPhysical Therapy Initial Evaluation GUIDEFredderick Federico100% (1)
- PE and HX Taking HandoutDocument11 pagesPE and HX Taking HandoutJoshua RivasNo ratings yet
- Overview of Pediatric Physical AssessmentDocument7 pagesOverview of Pediatric Physical AssessmentLloyd Jay Lin100% (1)
- 1.2 Approach To Diagnosis of Childhood Diseases MarkedDocument11 pages1.2 Approach To Diagnosis of Childhood Diseases MarkedSandeep VaghelaNo ratings yet
- 01.01 (PED) History CasubhaDocument6 pages01.01 (PED) History CasubhaAnonymouscatNo ratings yet
- CHN TransesDocument3 pagesCHN TransesShaira PacallesNo ratings yet
- 109 - Review On AssessmentDocument3 pages109 - Review On AssessmentCharisa Antonette HuelvaNo ratings yet
- Approach To The Evaluation of A PatientDocument7 pagesApproach To The Evaluation of A PatienthithNo ratings yet
- Pediatric History and PE - Dr. LeonesDocument4 pagesPediatric History and PE - Dr. LeonesmedicoNo ratings yet
- 108 - Medical HistoryDocument3 pages108 - Medical HistoryCharisa Antonette HuelvaNo ratings yet
- Pediatric Clinical HistoryDocument11 pagesPediatric Clinical HistoryRissa DeocampoNo ratings yet
- 01.07.01 Interviewing Skills - Filipino Medical LanguageDocument4 pages01.07.01 Interviewing Skills - Filipino Medical LanguageMikmik DGNo ratings yet
- Adult History Taking and Physical ExaminationDocument6 pagesAdult History Taking and Physical ExaminationDoc Prince Caballero100% (1)
- Module 3 HA Comprehensive Health History 1Document16 pagesModule 3 HA Comprehensive Health History 1Rosalinda LacuestaNo ratings yet
- Lec EpidemiologyDocument4 pagesLec EpidemiologyKelly James CuberoNo ratings yet
- 4 Year Clerkship in Psychiatry UWI MB, BS Programme: at The End of This Lecture, Students Should Be Able ToDocument10 pages4 Year Clerkship in Psychiatry UWI MB, BS Programme: at The End of This Lecture, Students Should Be Able ToNay ThureinNo ratings yet
- Space and DistanceDocument3 pagesSpace and DistanceJohn Paul MolinaNo ratings yet
- Nusring Case Analysis FormatDocument6 pagesNusring Case Analysis Formatchazney casianoNo ratings yet
- Exam 1 Study Guide Summary Advanced Health AssessmentDocument27 pagesExam 1 Study Guide Summary Advanced Health AssessmentRhoda Mae Cubilla100% (1)
- Autonomy: The Oldest Child of TheDocument9 pagesAutonomy: The Oldest Child of TheAC NaurgenNo ratings yet
- PX Ass Lecture Unit 2Document2 pagesPX Ass Lecture Unit 2henlo hiNo ratings yet
- Bates - History Taking SummeryDocument11 pagesBates - History Taking Summeryقيس نصراللهNo ratings yet
- 04 - Family - Nursing - Process - CHN Part2-1Document9 pages04 - Family - Nursing - Process - CHN Part2-1Ivan MaximusNo ratings yet
- Medical History, Patient Exam, and Patient Evaluation: Principles of MedicineDocument2 pagesMedical History, Patient Exam, and Patient Evaluation: Principles of MedicineBea YmsnNo ratings yet
- ST NDDocument9 pagesST NDOtiosse MyosotisNo ratings yet
- Strat4 Tool 1 IDEAL CHKLST DischargeDocument7 pagesStrat4 Tool 1 IDEAL CHKLST DischargeNurbaitiNo ratings yet
- Health AssessmentDocument4 pagesHealth Assessmentkatrina estanteNo ratings yet
- History, Physical Examination and Preventive Health CareDocument9 pagesHistory, Physical Examination and Preventive Health CareChristine Evan HoNo ratings yet
- Nursing Process - AdultDocument7 pagesNursing Process - Adultjoannamae molagaNo ratings yet
- NURSING CARE - Adhaini Widiyawati 2014901051Document9 pagesNURSING CARE - Adhaini Widiyawati 2014901051Adhaini WidiyawatiNo ratings yet
- Introduction To Oral Manifestations of Systemic DiseasesDocument8 pagesIntroduction To Oral Manifestations of Systemic DiseasesVitória SilvaNo ratings yet
- Preparation For Hospital Adaptation Presentation - 20240329 - 072106 - 0000Document38 pagesPreparation For Hospital Adaptation Presentation - 20240329 - 072106 - 0000Krizamay AggerNo ratings yet
- Physical Diagnosis - The Art of History TakingDocument3 pagesPhysical Diagnosis - The Art of History TakingCassandra Doyaoen100% (1)
- The Nursing Health History (NHH) : NCM 101-A: Health AssessmentDocument7 pagesThe Nursing Health History (NHH) : NCM 101-A: Health Assessmentthe someoneNo ratings yet
- Long Quiz Geron LecDocument3 pagesLong Quiz Geron LecDarwin QuirimitNo ratings yet
- (PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFDocument6 pages(PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFMon Kristoper CastilloNo ratings yet
- Care Plan Format MSNDocument8 pagesCare Plan Format MSNLijoNo ratings yet
- Preparing The Physical Setting: Nursing Care of The Older Adult WellnessDocument11 pagesPreparing The Physical Setting: Nursing Care of The Older Adult WellnessRose Ann HajironNo ratings yet
- I. Vital Information: W La Paz, Iloilo CityDocument7 pagesI. Vital Information: W La Paz, Iloilo CityelleNo ratings yet
- Skill 1Document13 pagesSkill 1Roshan VjNo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitPrincess Faniega SugatonNo ratings yet
- Comprehensive Health Assessment of The Older Person in Health and Aged CareDocument24 pagesComprehensive Health Assessment of The Older Person in Health and Aged Carenavdeep1133No ratings yet
- DIAGNOSISDocument4 pagesDIAGNOSISKriznilyn SibugNo ratings yet
- Module 4a NCM 114Document84 pagesModule 4a NCM 114SONZA JENNEFERNo ratings yet
- Diagnosis Procedure: DRG Sri Rezeki, SP - PMDocument94 pagesDiagnosis Procedure: DRG Sri Rezeki, SP - PMNiska DarliantiNo ratings yet
- 2013 History Taking - and Examination For UGDocument75 pages2013 History Taking - and Examination For UGsmitha manjunathNo ratings yet
- Health Assessment SKILLS NOTESDocument9 pagesHealth Assessment SKILLS NOTESPauline AñesNo ratings yet
- Clinical Evaluation of The Psychiatric PatientDocument4 pagesClinical Evaluation of The Psychiatric Patienthannjazz100% (1)
- Diklat Rekam MedikDocument196 pagesDiklat Rekam MedikMulyono Aba AthiyaNo ratings yet
- Revised Kanda NCPDocument3 pagesRevised Kanda NCPhaxa yzaNo ratings yet
- Family Health: Shifting ExamDocument19 pagesFamily Health: Shifting ExamRix tanNo ratings yet
- Chn-Health Nursing ProcessDocument7 pagesChn-Health Nursing ProcessBSN 1-N CASTRO, RicciNo ratings yet
- Katharine KolcabaDocument4 pagesKatharine KolcabaimmajinbuxoxoNo ratings yet
- Assessment: Complete Health HistoryDocument5 pagesAssessment: Complete Health HistoryNathan BarrerasNo ratings yet
- Week 15 Outbreak InvestigationDocument13 pagesWeek 15 Outbreak InvestigationAngeline LimNo ratings yet
- 07 History, Physical Examination, and Preventive Health CareDocument16 pages07 History, Physical Examination, and Preventive Health CareMwesigye Ruzindana EugeneNo ratings yet
- General Principles and Empirically Supported Techniques of Cognitive Behavior TherapyFrom EverandGeneral Principles and Empirically Supported Techniques of Cognitive Behavior TherapyNo ratings yet
- 10.2 PSYCH III Psychiatric Interview Mental Status ExamDocument24 pages10.2 PSYCH III Psychiatric Interview Mental Status ExamNorman Vryne CaduaNo ratings yet
- Ectopic Pregnancy - Ob PathoDocument32 pagesEctopic Pregnancy - Ob PathoNorman Vryne CaduaNo ratings yet
- Uti-Simple Task 2Document1 pageUti-Simple Task 2Norman Vryne CaduaNo ratings yet
- CMC Abruptio PlacentaDocument76 pagesCMC Abruptio PlacentaNorman Vryne CaduaNo ratings yet
- ENT Blank Drug Index For Clinical Clerks v1.0Document7 pagesENT Blank Drug Index For Clinical Clerks v1.0Norman Vryne CaduaNo ratings yet
- Clinico-Pathologic Conference OutputDocument3 pagesClinico-Pathologic Conference OutputNorman Vryne CaduaNo ratings yet
- Physio Ratio 8 FINALDocument19 pagesPhysio Ratio 8 FINALNorman Vryne CaduaNo ratings yet
- Assignment in PhysicsDocument7 pagesAssignment in PhysicsNorman Vryne CaduaNo ratings yet
- BIOCHEMISTRY: Laboratory DiscussionDocument7 pagesBIOCHEMISTRY: Laboratory DiscussionNorman Vryne CaduaNo ratings yet
- Aerobic DanceDocument17 pagesAerobic DanceRichard Dela CruzNo ratings yet
- Parenting Style and Self-EsteemDocument2 pagesParenting Style and Self-EsteemESPINO, GHILYNN M.No ratings yet
- Othmer Bab 3Document54 pagesOthmer Bab 3JHWNo ratings yet
- Abdominal "Signs" Table: Sign Diagnosis/ConditionDocument1 pageAbdominal "Signs" Table: Sign Diagnosis/ConditionMeg AmoonNo ratings yet
- Professional Development PlanDocument5 pagesProfessional Development Planapi-520853476No ratings yet
- Case Report: Psoriasis Vulgaris in Children - Case PresentationDocument5 pagesCase Report: Psoriasis Vulgaris in Children - Case PresentationInryuu ZenNo ratings yet
- SLMQ1G11to12DRRM3 v2Document20 pagesSLMQ1G11to12DRRM3 v2Joie OsherNo ratings yet
- Magsaysay Marine Inc. V, Michael Atraje, July 23, 2018Document2 pagesMagsaysay Marine Inc. V, Michael Atraje, July 23, 2018Russ TuazonNo ratings yet
- Worsheets Janina Fisher PDFDocument26 pagesWorsheets Janina Fisher PDFIgor Alejandro100% (2)
- Fitness RX For Women PDFDocument100 pagesFitness RX For Women PDFSuryaAagneya100% (3)
- Palliative Nursing Care: University of Eastern PhilippinesDocument2 pagesPalliative Nursing Care: University of Eastern PhilippinesZalde TuballasNo ratings yet
- Brief Psychotic Disorder Case PresDocument43 pagesBrief Psychotic Disorder Case PresTheressa TironaNo ratings yet
- Use of The Goldberg General Health Questionnaire (GHQ-28) To Detect Psychosocial Problems in The Family Physician's OfficeDocument9 pagesUse of The Goldberg General Health Questionnaire (GHQ-28) To Detect Psychosocial Problems in The Family Physician's OfficeIlto SandovalNo ratings yet
- Trags In-House Safety Induction TrainingDocument14 pagesTrags In-House Safety Induction TrainingRajesh MNo ratings yet
- What Is A Health AssessmentDocument2 pagesWhat Is A Health AssessmentKleeNo ratings yet
- Book Garba SamskaraDocument3 pagesBook Garba SamskaraYogaguru NehaNo ratings yet
- STR SIZ Hit Points DEX APP Luck INT EDU Sanity CON POW Magic PointsDocument3 pagesSTR SIZ Hit Points DEX APP Luck INT EDU Sanity CON POW Magic PointsArthur NunesNo ratings yet
- Politics Masquerading As Science: Ralph Greenson, Anna Freud, and The Klein WarsDocument17 pagesPolitics Masquerading As Science: Ralph Greenson, Anna Freud, and The Klein Warsmelpomena81No ratings yet
- 10 Ways To Reduce StressDocument1 page10 Ways To Reduce StressSamantha MojicaNo ratings yet
- Jung Typology ExplainedDocument34 pagesJung Typology Explainederic silvaNo ratings yet
- 20th National Awareness Week For The Prevention ofDocument2 pages20th National Awareness Week For The Prevention ofKur EneiNo ratings yet
- Electronic Document Management System (EDMS) Implementation: Implications For The Future of Digital Transformation in Philippine HealthcareDocument10 pagesElectronic Document Management System (EDMS) Implementation: Implications For The Future of Digital Transformation in Philippine HealthcareEthan OuroNo ratings yet
- CAPD ExplorationDocument2 pagesCAPD Explorationtito mnyoneNo ratings yet
- Assessments For The Newborn BabiesDocument11 pagesAssessments For The Newborn BabiesBeatrice ChenNo ratings yet
- Laboratory Procedure Manual: Alanine Amino Transferase (ALT) Refrigerated SerumDocument9 pagesLaboratory Procedure Manual: Alanine Amino Transferase (ALT) Refrigerated Serumحيدر كاملNo ratings yet
- Chapter 2 Fire Fighter SafetyDocument2 pagesChapter 2 Fire Fighter SafetyMuhammad Alshikh100% (1)
- BEARD, Victoria A. Learning Radical Planning The Power of Collective Action. Plannning Theory, 2003.Document24 pagesBEARD, Victoria A. Learning Radical Planning The Power of Collective Action. Plannning Theory, 2003.Fɑbio PrietoNo ratings yet
- Unit 6 Growth and Development and Care of The AdolescentDocument17 pagesUnit 6 Growth and Development and Care of The AdolescentKyla CapituloNo ratings yet
- Microbiology Compilation (MRS Saliu)Document15 pagesMicrobiology Compilation (MRS Saliu)Nifemi AketanNo ratings yet
- Therapeutic Area Data Standards User Guide For Diabetes: (Provisional)Document170 pagesTherapeutic Area Data Standards User Guide For Diabetes: (Provisional)pathuri rangaNo ratings yet


































































































Download as pdf or txt
You might also like
- Hydrocarbons Worksheet AnswersDocument2 pagesHydrocarbons Worksheet AnswersNorman Vryne Cadua100% (1)
- Vet Clin Procedures - Large Animal History TakingDocument7 pagesVet Clin Procedures - Large Animal History TakinglechamariaNo ratings yet
- Pediatric HX and PEDocument8 pagesPediatric HX and PEsahani100% (2)
- Pediatric History & Physical ExamDocument5 pagesPediatric History & Physical ExamLloyd Jay Lin100% (2)
- Physical Therapy Initial Evaluation GUIDEDocument152 pagesPhysical Therapy Initial Evaluation GUIDEFredderick Federico100% (1)
- PE and HX Taking HandoutDocument11 pagesPE and HX Taking HandoutJoshua RivasNo ratings yet
- Overview of Pediatric Physical AssessmentDocument7 pagesOverview of Pediatric Physical AssessmentLloyd Jay Lin100% (1)
- 1.2 Approach To Diagnosis of Childhood Diseases MarkedDocument11 pages1.2 Approach To Diagnosis of Childhood Diseases MarkedSandeep VaghelaNo ratings yet
- 01.01 (PED) History CasubhaDocument6 pages01.01 (PED) History CasubhaAnonymouscatNo ratings yet
- CHN TransesDocument3 pagesCHN TransesShaira PacallesNo ratings yet
- 109 - Review On AssessmentDocument3 pages109 - Review On AssessmentCharisa Antonette HuelvaNo ratings yet
- Approach To The Evaluation of A PatientDocument7 pagesApproach To The Evaluation of A PatienthithNo ratings yet
- Pediatric History and PE - Dr. LeonesDocument4 pagesPediatric History and PE - Dr. LeonesmedicoNo ratings yet
- 108 - Medical HistoryDocument3 pages108 - Medical HistoryCharisa Antonette HuelvaNo ratings yet
- Pediatric Clinical HistoryDocument11 pagesPediatric Clinical HistoryRissa DeocampoNo ratings yet
- 01.07.01 Interviewing Skills - Filipino Medical LanguageDocument4 pages01.07.01 Interviewing Skills - Filipino Medical LanguageMikmik DGNo ratings yet
- Adult History Taking and Physical ExaminationDocument6 pagesAdult History Taking and Physical ExaminationDoc Prince Caballero100% (1)
- Module 3 HA Comprehensive Health History 1Document16 pagesModule 3 HA Comprehensive Health History 1Rosalinda LacuestaNo ratings yet
- Lec EpidemiologyDocument4 pagesLec EpidemiologyKelly James CuberoNo ratings yet
- 4 Year Clerkship in Psychiatry UWI MB, BS Programme: at The End of This Lecture, Students Should Be Able ToDocument10 pages4 Year Clerkship in Psychiatry UWI MB, BS Programme: at The End of This Lecture, Students Should Be Able ToNay ThureinNo ratings yet
- Space and DistanceDocument3 pagesSpace and DistanceJohn Paul MolinaNo ratings yet
- Nusring Case Analysis FormatDocument6 pagesNusring Case Analysis Formatchazney casianoNo ratings yet
- Exam 1 Study Guide Summary Advanced Health AssessmentDocument27 pagesExam 1 Study Guide Summary Advanced Health AssessmentRhoda Mae Cubilla100% (1)
- Autonomy: The Oldest Child of TheDocument9 pagesAutonomy: The Oldest Child of TheAC NaurgenNo ratings yet
- PX Ass Lecture Unit 2Document2 pagesPX Ass Lecture Unit 2henlo hiNo ratings yet
- Bates - History Taking SummeryDocument11 pagesBates - History Taking Summeryقيس نصراللهNo ratings yet
- 04 - Family - Nursing - Process - CHN Part2-1Document9 pages04 - Family - Nursing - Process - CHN Part2-1Ivan MaximusNo ratings yet
- Medical History, Patient Exam, and Patient Evaluation: Principles of MedicineDocument2 pagesMedical History, Patient Exam, and Patient Evaluation: Principles of MedicineBea YmsnNo ratings yet
- ST NDDocument9 pagesST NDOtiosse MyosotisNo ratings yet
- Strat4 Tool 1 IDEAL CHKLST DischargeDocument7 pagesStrat4 Tool 1 IDEAL CHKLST DischargeNurbaitiNo ratings yet
- Health AssessmentDocument4 pagesHealth Assessmentkatrina estanteNo ratings yet
- History, Physical Examination and Preventive Health CareDocument9 pagesHistory, Physical Examination and Preventive Health CareChristine Evan HoNo ratings yet
- Nursing Process - AdultDocument7 pagesNursing Process - Adultjoannamae molagaNo ratings yet
- NURSING CARE - Adhaini Widiyawati 2014901051Document9 pagesNURSING CARE - Adhaini Widiyawati 2014901051Adhaini WidiyawatiNo ratings yet
- Introduction To Oral Manifestations of Systemic DiseasesDocument8 pagesIntroduction To Oral Manifestations of Systemic DiseasesVitória SilvaNo ratings yet
- Preparation For Hospital Adaptation Presentation - 20240329 - 072106 - 0000Document38 pagesPreparation For Hospital Adaptation Presentation - 20240329 - 072106 - 0000Krizamay AggerNo ratings yet
- Physical Diagnosis - The Art of History TakingDocument3 pagesPhysical Diagnosis - The Art of History TakingCassandra Doyaoen100% (1)
- The Nursing Health History (NHH) : NCM 101-A: Health AssessmentDocument7 pagesThe Nursing Health History (NHH) : NCM 101-A: Health Assessmentthe someoneNo ratings yet
- Long Quiz Geron LecDocument3 pagesLong Quiz Geron LecDarwin QuirimitNo ratings yet
- (PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFDocument6 pages(PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFMon Kristoper CastilloNo ratings yet
- Care Plan Format MSNDocument8 pagesCare Plan Format MSNLijoNo ratings yet
- Preparing The Physical Setting: Nursing Care of The Older Adult WellnessDocument11 pagesPreparing The Physical Setting: Nursing Care of The Older Adult WellnessRose Ann HajironNo ratings yet
- I. Vital Information: W La Paz, Iloilo CityDocument7 pagesI. Vital Information: W La Paz, Iloilo CityelleNo ratings yet
- Skill 1Document13 pagesSkill 1Roshan VjNo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitPrincess Faniega SugatonNo ratings yet
- Comprehensive Health Assessment of The Older Person in Health and Aged CareDocument24 pagesComprehensive Health Assessment of The Older Person in Health and Aged Carenavdeep1133No ratings yet
- DIAGNOSISDocument4 pagesDIAGNOSISKriznilyn SibugNo ratings yet
- Module 4a NCM 114Document84 pagesModule 4a NCM 114SONZA JENNEFERNo ratings yet
- Diagnosis Procedure: DRG Sri Rezeki, SP - PMDocument94 pagesDiagnosis Procedure: DRG Sri Rezeki, SP - PMNiska DarliantiNo ratings yet
- 2013 History Taking - and Examination For UGDocument75 pages2013 History Taking - and Examination For UGsmitha manjunathNo ratings yet
- Health Assessment SKILLS NOTESDocument9 pagesHealth Assessment SKILLS NOTESPauline AñesNo ratings yet
- Clinical Evaluation of The Psychiatric PatientDocument4 pagesClinical Evaluation of The Psychiatric Patienthannjazz100% (1)
- Diklat Rekam MedikDocument196 pagesDiklat Rekam MedikMulyono Aba AthiyaNo ratings yet
- Revised Kanda NCPDocument3 pagesRevised Kanda NCPhaxa yzaNo ratings yet
- Family Health: Shifting ExamDocument19 pagesFamily Health: Shifting ExamRix tanNo ratings yet
- Chn-Health Nursing ProcessDocument7 pagesChn-Health Nursing ProcessBSN 1-N CASTRO, RicciNo ratings yet
- Katharine KolcabaDocument4 pagesKatharine KolcabaimmajinbuxoxoNo ratings yet
- Assessment: Complete Health HistoryDocument5 pagesAssessment: Complete Health HistoryNathan BarrerasNo ratings yet
- Week 15 Outbreak InvestigationDocument13 pagesWeek 15 Outbreak InvestigationAngeline LimNo ratings yet
- 07 History, Physical Examination, and Preventive Health CareDocument16 pages07 History, Physical Examination, and Preventive Health CareMwesigye Ruzindana EugeneNo ratings yet
- General Principles and Empirically Supported Techniques of Cognitive Behavior TherapyFrom EverandGeneral Principles and Empirically Supported Techniques of Cognitive Behavior TherapyNo ratings yet
- 10.2 PSYCH III Psychiatric Interview Mental Status ExamDocument24 pages10.2 PSYCH III Psychiatric Interview Mental Status ExamNorman Vryne CaduaNo ratings yet
- Ectopic Pregnancy - Ob PathoDocument32 pagesEctopic Pregnancy - Ob PathoNorman Vryne CaduaNo ratings yet
- Uti-Simple Task 2Document1 pageUti-Simple Task 2Norman Vryne CaduaNo ratings yet
- CMC Abruptio PlacentaDocument76 pagesCMC Abruptio PlacentaNorman Vryne CaduaNo ratings yet
- ENT Blank Drug Index For Clinical Clerks v1.0Document7 pagesENT Blank Drug Index For Clinical Clerks v1.0Norman Vryne CaduaNo ratings yet
- Clinico-Pathologic Conference OutputDocument3 pagesClinico-Pathologic Conference OutputNorman Vryne CaduaNo ratings yet
- Physio Ratio 8 FINALDocument19 pagesPhysio Ratio 8 FINALNorman Vryne CaduaNo ratings yet
- Assignment in PhysicsDocument7 pagesAssignment in PhysicsNorman Vryne CaduaNo ratings yet
- BIOCHEMISTRY: Laboratory DiscussionDocument7 pagesBIOCHEMISTRY: Laboratory DiscussionNorman Vryne CaduaNo ratings yet
- Aerobic DanceDocument17 pagesAerobic DanceRichard Dela CruzNo ratings yet
- Parenting Style and Self-EsteemDocument2 pagesParenting Style and Self-EsteemESPINO, GHILYNN M.No ratings yet
- Othmer Bab 3Document54 pagesOthmer Bab 3JHWNo ratings yet
- Abdominal "Signs" Table: Sign Diagnosis/ConditionDocument1 pageAbdominal "Signs" Table: Sign Diagnosis/ConditionMeg AmoonNo ratings yet
- Professional Development PlanDocument5 pagesProfessional Development Planapi-520853476No ratings yet
- Case Report: Psoriasis Vulgaris in Children - Case PresentationDocument5 pagesCase Report: Psoriasis Vulgaris in Children - Case PresentationInryuu ZenNo ratings yet
- SLMQ1G11to12DRRM3 v2Document20 pagesSLMQ1G11to12DRRM3 v2Joie OsherNo ratings yet
- Magsaysay Marine Inc. V, Michael Atraje, July 23, 2018Document2 pagesMagsaysay Marine Inc. V, Michael Atraje, July 23, 2018Russ TuazonNo ratings yet
- Worsheets Janina Fisher PDFDocument26 pagesWorsheets Janina Fisher PDFIgor Alejandro100% (2)
- Fitness RX For Women PDFDocument100 pagesFitness RX For Women PDFSuryaAagneya100% (3)
- Palliative Nursing Care: University of Eastern PhilippinesDocument2 pagesPalliative Nursing Care: University of Eastern PhilippinesZalde TuballasNo ratings yet
- Brief Psychotic Disorder Case PresDocument43 pagesBrief Psychotic Disorder Case PresTheressa TironaNo ratings yet
- Use of The Goldberg General Health Questionnaire (GHQ-28) To Detect Psychosocial Problems in The Family Physician's OfficeDocument9 pagesUse of The Goldberg General Health Questionnaire (GHQ-28) To Detect Psychosocial Problems in The Family Physician's OfficeIlto SandovalNo ratings yet
- Trags In-House Safety Induction TrainingDocument14 pagesTrags In-House Safety Induction TrainingRajesh MNo ratings yet
- What Is A Health AssessmentDocument2 pagesWhat Is A Health AssessmentKleeNo ratings yet
- Book Garba SamskaraDocument3 pagesBook Garba SamskaraYogaguru NehaNo ratings yet
- STR SIZ Hit Points DEX APP Luck INT EDU Sanity CON POW Magic PointsDocument3 pagesSTR SIZ Hit Points DEX APP Luck INT EDU Sanity CON POW Magic PointsArthur NunesNo ratings yet
- Politics Masquerading As Science: Ralph Greenson, Anna Freud, and The Klein WarsDocument17 pagesPolitics Masquerading As Science: Ralph Greenson, Anna Freud, and The Klein Warsmelpomena81No ratings yet
- 10 Ways To Reduce StressDocument1 page10 Ways To Reduce StressSamantha MojicaNo ratings yet
- Jung Typology ExplainedDocument34 pagesJung Typology Explainederic silvaNo ratings yet
- 20th National Awareness Week For The Prevention ofDocument2 pages20th National Awareness Week For The Prevention ofKur EneiNo ratings yet
- Electronic Document Management System (EDMS) Implementation: Implications For The Future of Digital Transformation in Philippine HealthcareDocument10 pagesElectronic Document Management System (EDMS) Implementation: Implications For The Future of Digital Transformation in Philippine HealthcareEthan OuroNo ratings yet
- CAPD ExplorationDocument2 pagesCAPD Explorationtito mnyoneNo ratings yet
- Assessments For The Newborn BabiesDocument11 pagesAssessments For The Newborn BabiesBeatrice ChenNo ratings yet
- Laboratory Procedure Manual: Alanine Amino Transferase (ALT) Refrigerated SerumDocument9 pagesLaboratory Procedure Manual: Alanine Amino Transferase (ALT) Refrigerated Serumحيدر كاملNo ratings yet
- Chapter 2 Fire Fighter SafetyDocument2 pagesChapter 2 Fire Fighter SafetyMuhammad Alshikh100% (1)
- BEARD, Victoria A. Learning Radical Planning The Power of Collective Action. Plannning Theory, 2003.Document24 pagesBEARD, Victoria A. Learning Radical Planning The Power of Collective Action. Plannning Theory, 2003.Fɑbio PrietoNo ratings yet
- Unit 6 Growth and Development and Care of The AdolescentDocument17 pagesUnit 6 Growth and Development and Care of The AdolescentKyla CapituloNo ratings yet
- Microbiology Compilation (MRS Saliu)Document15 pagesMicrobiology Compilation (MRS Saliu)Nifemi AketanNo ratings yet
- Therapeutic Area Data Standards User Guide For Diabetes: (Provisional)Document170 pagesTherapeutic Area Data Standards User Guide For Diabetes: (Provisional)pathuri rangaNo ratings yet