
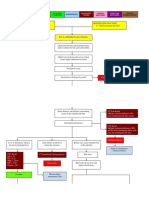
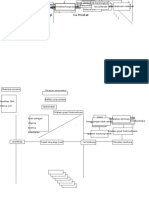
Chronic Pancreatitis: Causes Complications
Chronic Pancreatitis: Causes Complications
You might also like
- Acute PancreatitisDocument31 pagesAcute PancreatitisAmoroso, Marian Corneth D.No ratings yet
- Pathophysiology - Obstructive JaundiceDocument3 pagesPathophysiology - Obstructive JaundiceAbigail Lonogan0% (1)
- Endocrine HarmonyDocument68 pagesEndocrine HarmonyafnanNo ratings yet
- ANAPHY Lec Session #21 - SAS (Agdana, Nicole Ken)Document8 pagesANAPHY Lec Session #21 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Anatomy and Physiology Final Exam MsuDocument10 pagesAnatomy and Physiology Final Exam MsuAlibasher Macalnas100% (1)
- Whipple Procedure Case Study PresentationDocument30 pagesWhipple Procedure Case Study Presentationapi-315408947100% (3)
- Endocrine System MCQDocument19 pagesEndocrine System MCQBijay Kumar MahatoNo ratings yet
- Complications: Acute PancreatitisDocument2 pagesComplications: Acute PancreatitisNikey LimNo ratings yet
- ACUTE PANCREATITISDocument19 pagesACUTE PANCREATITISMaaz MansoorNo ratings yet
- Pathophysiology of Acute Renal FailureDocument1 pagePathophysiology of Acute Renal FailureAina HaravataNo ratings yet
- MS A - Mod 1 Cont Hepatobiliary and Pancreatic DisorderDocument1 pageMS A - Mod 1 Cont Hepatobiliary and Pancreatic DisorderCrisanta Grace OpondaNo ratings yet
- Week 3 Liver Func, AlterDocument12 pagesWeek 3 Liver Func, AlterMarquez Robee Xan DanielNo ratings yet
- Cholelithiasis CholecystitisDocument1 pageCholelithiasis Cholecystitissamliebareng77No ratings yet
- Diagnostic Methods: AmylaseDocument34 pagesDiagnostic Methods: Amylaseclaudia mcheikNo ratings yet
- Isolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionDocument3 pagesIsolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionleozdmNo ratings yet
- Chronic PancreatitisDocument3 pagesChronic PancreatitisCharry AlupiasNo ratings yet
- 116 Theory NotesDocument84 pages116 Theory NotesKirstie Goc-ongNo ratings yet
- EA Cocept Map2Document2 pagesEA Cocept Map2Katie LopezNo ratings yet
- An Approach To Obstructive JaundiceDocument5 pagesAn Approach To Obstructive JaundiceEvediciNo ratings yet
- Chapter-7-Pathophysiology Nephrotic SyndromeDocument3 pagesChapter-7-Pathophysiology Nephrotic SyndromeCxarina RamirezNo ratings yet
- Allopurinol (Drug Study)Document2 pagesAllopurinol (Drug Study)Daisy PalisocNo ratings yet
- Neuro TumoresDocument14 pagesNeuro TumoresCarlos SotoNo ratings yet
- Omeprazole (FSW)Document3 pagesOmeprazole (FSW)khelxoNo ratings yet
- Acute Chronic PancreatitisDocument17 pagesAcute Chronic Pancreatitisjimjose antonyNo ratings yet
- Trans Hepatobiliary SystemDocument5 pagesTrans Hepatobiliary SystemJulie CatianNo ratings yet
- Payhway IleusDocument1 pagePayhway IleusLarasparkyu ElfNo ratings yet
- PPK Prost atDocument2 pagesPPK Prost atlisarahmaasrilNo ratings yet
- Mesenteric Vascular Insufficiency: ClassificationDocument2 pagesMesenteric Vascular Insufficiency: ClassificationIsabel CastilloNo ratings yet
- MHD Exam 5 MaterialDocument122 pagesMHD Exam 5 Materialnaexuis5467100% (1)
- MED 1.19 - PancreatitisDocument3 pagesMED 1.19 - PancreatitisZazaNo ratings yet
- Ketorolac DRUG STUDYDocument3 pagesKetorolac DRUG STUDYA.No ratings yet
- WBS Kul - Trauma UroDocument19 pagesWBS Kul - Trauma UroRizal ArzaniNo ratings yet
- Percutaneous Transhepatic Biliary InterventionsDocument11 pagesPercutaneous Transhepatic Biliary InterventionsLe Hu ThaNo ratings yet
- PathyDocument3 pagesPathyTRIXY MAE HORTILLANO100% (1)
- Gastrointestinal SurgeryDocument12 pagesGastrointestinal SurgeryHafsa AliNo ratings yet
- Ampullary Carcinoma - Dr. Limchiaco, J.Document11 pagesAmpullary Carcinoma - Dr. Limchiaco, J.Neil Victor Ongco PajugotNo ratings yet
- Urinary Tract Obstruction: DefinitionsDocument14 pagesUrinary Tract Obstruction: DefinitionsAuliaNo ratings yet
- Enzymes in Clinical DiagnosisDocument2 pagesEnzymes in Clinical DiagnosisShobe ChuaNo ratings yet
- Pancreas RobbinsDocument13 pagesPancreas RobbinsAndrea PescosolidoNo ratings yet
- Acute Pancreatitis, Hepatitis, Liver Cirrhosis: Ma Eileen O Pascua, MD, FPCP, FPSG, FpsdeDocument24 pagesAcute Pancreatitis, Hepatitis, Liver Cirrhosis: Ma Eileen O Pascua, MD, FPCP, FPSG, FpsdePrincess Noreen SavellanoNo ratings yet
- C HPB (Blue Keyword Pyq)Document5 pagesC HPB (Blue Keyword Pyq)Irsyad SiddeeqNo ratings yet
- Not Activity No. 7Document12 pagesNot Activity No. 7Patricia Marie Laman YadaoNo ratings yet
- Anytime I Don'T Remember Something From Uworld, I Go Straight To MemorangDocument3 pagesAnytime I Don'T Remember Something From Uworld, I Go Straight To MemorangRa ViNo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Week 2Document5 pagesWeek 2Maica LectanaNo ratings yet
- Uro Spots SummaryDocument25 pagesUro Spots Summarynthabiseng maboganaNo ratings yet
- SystemicSclerosis GastrointestinalDiseaseandIts ManagementDocument15 pagesSystemicSclerosis GastrointestinalDiseaseandIts ManagementMércia FonsecaNo ratings yet
- Kuliah Trauma Urologi - DR WibisonoDocument34 pagesKuliah Trauma Urologi - DR WibisonoAgung Budi SuristioNo ratings yet
- Gastroenterology PancreatitisDocument1 pageGastroenterology PancreatitisNour SamadNo ratings yet
- Osacicon Poster Annular PancreasDocument1 pageOsacicon Poster Annular PancreasAbhishek Soham SatpathyNo ratings yet
- OMEPRAZOLEDocument2 pagesOMEPRAZOLERea LynNo ratings yet
- ARF PathoDocument3 pagesARF PathoNikki RodrigoNo ratings yet
- Peptic Ulcer DiseaseDocument119 pagesPeptic Ulcer DiseaseJoy LacunaNo ratings yet
- Case Pre Drug StudyDocument22 pagesCase Pre Drug StudyBenjie DimayacyacNo ratings yet
- Poster Vishnu Semi Copy2Document1 pagePoster Vishnu Semi Copy2sri harshaNo ratings yet
- Gastrointestinal OsmosisDocument174 pagesGastrointestinal OsmosisfabicontrerasenarmNo ratings yet
- Acute PancreatitisDocument8 pagesAcute PancreatitisAthan AntonioNo ratings yet
- Surgical Masters TacticsDocument7 pagesSurgical Masters TacticsaizatamlikhaNo ratings yet
- Drug StudyDocument3 pagesDrug StudyalysNo ratings yet
- CHOLANGITISDocument7 pagesCHOLANGITISWill GutierrezNo ratings yet
- MS-2 GallbladderDocument2 pagesMS-2 Gallbladderelijahdale.guillergan-05No ratings yet
- Nursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationDocument2 pagesNursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationOmar IzzoNo ratings yet
- Disorders of PancreasDocument43 pagesDisorders of Pancreasindu mathiNo ratings yet
- Pathophysiology CholeDocument3 pagesPathophysiology CholeClyde AleczandreNo ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- Complications: Acute PancreatitisDocument2 pagesComplications: Acute PancreatitisNikey LimNo ratings yet
- History: Clinical ManifestationsDocument2 pagesHistory: Clinical ManifestationsNikey LimNo ratings yet
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseNikey LimNo ratings yet
- Resp 3Document2 pagesResp 3Nikey LimNo ratings yet
- Ideas From The One-Minute Manager: Strategic ManagementDocument2 pagesIdeas From The One-Minute Manager: Strategic ManagementNikey LimNo ratings yet
- Sleep-Related Upper Airway Obstruction in ChildrenDocument1 pageSleep-Related Upper Airway Obstruction in ChildrenNikey LimNo ratings yet
- Paeds Surgery 1Document2 pagesPaeds Surgery 1Nikey LimNo ratings yet
- Resp 1Document2 pagesResp 1Nikey LimNo ratings yet
- Section 03 Concepts of Family MedicineDocument2 pagesSection 03 Concepts of Family MedicineNikey LimNo ratings yet
- Section 04: Being A ManagerDocument2 pagesSection 04: Being A ManagerNikey LimNo ratings yet
- Care of The Patient and His FamilyDocument2 pagesCare of The Patient and His FamilyNikey LimNo ratings yet
- Doctor/Patient Communication: Family SupportDocument2 pagesDoctor/Patient Communication: Family SupportNikey LimNo ratings yet
- Inborn Errors of MetabolismDocument2 pagesInborn Errors of MetabolismNikey LimNo ratings yet
- Heart Failure 1Document2 pagesHeart Failure 1Nikey LimNo ratings yet
- Bradycardia and Conduction Disorders Sinus Bradycardia (Fig. 1.6)Document2 pagesBradycardia and Conduction Disorders Sinus Bradycardia (Fig. 1.6)Nikey LimNo ratings yet
- Arrhythmia 3Document2 pagesArrhythmia 3Nikey LimNo ratings yet
- Respiratory DiseaseDocument1 pageRespiratory DiseaseNikey LimNo ratings yet
- Proteus: Boys Girls (Form Phosphate Stone) Pseudomonas: Structural Abnormality in UT Plastic CathetersDocument2 pagesProteus: Boys Girls (Form Phosphate Stone) Pseudomonas: Structural Abnormality in UT Plastic CathetersNikey LimNo ratings yet
- Data StreamDocument87 pagesData StreamL-Va AndesNo ratings yet
- PhysAssessAbdomen 1Document21 pagesPhysAssessAbdomen 1David DvoskineNo ratings yet
- Management of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeDocument13 pagesManagement of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeSole GonzalezNo ratings yet
- Cancer Self TreatmentDocument35 pagesCancer Self TreatmentRichard HoltNo ratings yet
- CF NutritionDocument288 pagesCF Nutritionrkuip960% (1)
- Uji Efek Ekstrak Etanol Kulit Terung Ungu Terhadap Gambaran Histopatologi Pankreas Tikus Putih JantanDocument10 pagesUji Efek Ekstrak Etanol Kulit Terung Ungu Terhadap Gambaran Histopatologi Pankreas Tikus Putih Jantanridho kNo ratings yet
- AP-2 Lab Report - Lab 01 The Endrocine SystemDocument15 pagesAP-2 Lab Report - Lab 01 The Endrocine Systemrcdunfee86% (7)
- Cholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarDocument25 pagesCholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarMc Crister Silang100% (1)
- Redox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsDocument6 pagesRedox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsEdisher TsivtsivadzeNo ratings yet
- BAB I PancreatoblastomaDocument5 pagesBAB I PancreatoblastomaHana YunikoNo ratings yet
- The Digestive System: Ontent Earning CtivityDocument18 pagesThe Digestive System: Ontent Earning CtivityCamille Ann Faigao FamisanNo ratings yet
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- Literature Review On Prevalence of Diabetes MellitusDocument8 pagesLiterature Review On Prevalence of Diabetes MellitusnnactlvkgNo ratings yet
- Annular Pancreas Divisumtreated With Whipple Procedure: A Case Reportand Update of Arare ConditionDocument5 pagesAnnular Pancreas Divisumtreated With Whipple Procedure: A Case Reportand Update of Arare ConditionIJAR JOURNALNo ratings yet
- Surgery 2 PancreasDocument28 pagesSurgery 2 PancreasPARADISE JanoNo ratings yet
- Full Download Test Bank For Krauses Food and The Nutrition Care Process 14th Edition by Mahan PDF Full ChapterDocument36 pagesFull Download Test Bank For Krauses Food and The Nutrition Care Process 14th Edition by Mahan PDF Full Chaptercentimedisallyj0v47y100% (21)
- Histologia de PeixesDocument139 pagesHistologia de PeixesLetícia S. de CarvalhoNo ratings yet
- Sorted Feedback TopicwiseDocument55 pagesSorted Feedback TopicwiseLokesh BakshiNo ratings yet
- AIFSET 2021 Exam PaperDocument17 pagesAIFSET 2021 Exam Paperreshu.reshumiNo ratings yet
- Acute PancreatitisDocument39 pagesAcute PancreatitisJm Bernardo100% (1)
- 2.4.4.5c Acute PancreatitisDocument38 pages2.4.4.5c Acute PancreatitisAlfathush ShalihahNo ratings yet
- OCR A A-Level Biology Retrieval Roulette COMPLETEDocument115 pagesOCR A A-Level Biology Retrieval Roulette COMPLETEtikif31811No ratings yet
- Digestive System ReviewerDocument2 pagesDigestive System ReviewerDivino BauzonNo ratings yet
- Surgical Approach To Peritonitis and Abdominal Sepsis - Background, Preoperative Preparation, Considerations For Surgical ManagementDocument8 pagesSurgical Approach To Peritonitis and Abdominal Sepsis - Background, Preoperative Preparation, Considerations For Surgical ManagementCiubuc AndrianNo ratings yet
- PassAMCQ Study Companion 21Document30 pagesPassAMCQ Study Companion 21nitesawakeningNo ratings yet









































































































Download as doc, pdf, or txt
You might also like
- Acute PancreatitisDocument31 pagesAcute PancreatitisAmoroso, Marian Corneth D.No ratings yet
- Pathophysiology - Obstructive JaundiceDocument3 pagesPathophysiology - Obstructive JaundiceAbigail Lonogan0% (1)
- Endocrine HarmonyDocument68 pagesEndocrine HarmonyafnanNo ratings yet
- ANAPHY Lec Session #21 - SAS (Agdana, Nicole Ken)Document8 pagesANAPHY Lec Session #21 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Anatomy and Physiology Final Exam MsuDocument10 pagesAnatomy and Physiology Final Exam MsuAlibasher Macalnas100% (1)
- Whipple Procedure Case Study PresentationDocument30 pagesWhipple Procedure Case Study Presentationapi-315408947100% (3)
- Endocrine System MCQDocument19 pagesEndocrine System MCQBijay Kumar MahatoNo ratings yet
- Complications: Acute PancreatitisDocument2 pagesComplications: Acute PancreatitisNikey LimNo ratings yet
- ACUTE PANCREATITISDocument19 pagesACUTE PANCREATITISMaaz MansoorNo ratings yet
- Pathophysiology of Acute Renal FailureDocument1 pagePathophysiology of Acute Renal FailureAina HaravataNo ratings yet
- MS A - Mod 1 Cont Hepatobiliary and Pancreatic DisorderDocument1 pageMS A - Mod 1 Cont Hepatobiliary and Pancreatic DisorderCrisanta Grace OpondaNo ratings yet
- Week 3 Liver Func, AlterDocument12 pagesWeek 3 Liver Func, AlterMarquez Robee Xan DanielNo ratings yet
- Cholelithiasis CholecystitisDocument1 pageCholelithiasis Cholecystitissamliebareng77No ratings yet
- Diagnostic Methods: AmylaseDocument34 pagesDiagnostic Methods: Amylaseclaudia mcheikNo ratings yet
- Isolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionDocument3 pagesIsolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionleozdmNo ratings yet
- Chronic PancreatitisDocument3 pagesChronic PancreatitisCharry AlupiasNo ratings yet
- 116 Theory NotesDocument84 pages116 Theory NotesKirstie Goc-ongNo ratings yet
- EA Cocept Map2Document2 pagesEA Cocept Map2Katie LopezNo ratings yet
- An Approach To Obstructive JaundiceDocument5 pagesAn Approach To Obstructive JaundiceEvediciNo ratings yet
- Chapter-7-Pathophysiology Nephrotic SyndromeDocument3 pagesChapter-7-Pathophysiology Nephrotic SyndromeCxarina RamirezNo ratings yet
- Allopurinol (Drug Study)Document2 pagesAllopurinol (Drug Study)Daisy PalisocNo ratings yet
- Neuro TumoresDocument14 pagesNeuro TumoresCarlos SotoNo ratings yet
- Omeprazole (FSW)Document3 pagesOmeprazole (FSW)khelxoNo ratings yet
- Acute Chronic PancreatitisDocument17 pagesAcute Chronic Pancreatitisjimjose antonyNo ratings yet
- Trans Hepatobiliary SystemDocument5 pagesTrans Hepatobiliary SystemJulie CatianNo ratings yet
- Payhway IleusDocument1 pagePayhway IleusLarasparkyu ElfNo ratings yet
- PPK Prost atDocument2 pagesPPK Prost atlisarahmaasrilNo ratings yet
- Mesenteric Vascular Insufficiency: ClassificationDocument2 pagesMesenteric Vascular Insufficiency: ClassificationIsabel CastilloNo ratings yet
- MHD Exam 5 MaterialDocument122 pagesMHD Exam 5 Materialnaexuis5467100% (1)
- MED 1.19 - PancreatitisDocument3 pagesMED 1.19 - PancreatitisZazaNo ratings yet
- Ketorolac DRUG STUDYDocument3 pagesKetorolac DRUG STUDYA.No ratings yet
- WBS Kul - Trauma UroDocument19 pagesWBS Kul - Trauma UroRizal ArzaniNo ratings yet
- Percutaneous Transhepatic Biliary InterventionsDocument11 pagesPercutaneous Transhepatic Biliary InterventionsLe Hu ThaNo ratings yet
- PathyDocument3 pagesPathyTRIXY MAE HORTILLANO100% (1)
- Gastrointestinal SurgeryDocument12 pagesGastrointestinal SurgeryHafsa AliNo ratings yet
- Ampullary Carcinoma - Dr. Limchiaco, J.Document11 pagesAmpullary Carcinoma - Dr. Limchiaco, J.Neil Victor Ongco PajugotNo ratings yet
- Urinary Tract Obstruction: DefinitionsDocument14 pagesUrinary Tract Obstruction: DefinitionsAuliaNo ratings yet
- Enzymes in Clinical DiagnosisDocument2 pagesEnzymes in Clinical DiagnosisShobe ChuaNo ratings yet
- Pancreas RobbinsDocument13 pagesPancreas RobbinsAndrea PescosolidoNo ratings yet
- Acute Pancreatitis, Hepatitis, Liver Cirrhosis: Ma Eileen O Pascua, MD, FPCP, FPSG, FpsdeDocument24 pagesAcute Pancreatitis, Hepatitis, Liver Cirrhosis: Ma Eileen O Pascua, MD, FPCP, FPSG, FpsdePrincess Noreen SavellanoNo ratings yet
- C HPB (Blue Keyword Pyq)Document5 pagesC HPB (Blue Keyword Pyq)Irsyad SiddeeqNo ratings yet
- Not Activity No. 7Document12 pagesNot Activity No. 7Patricia Marie Laman YadaoNo ratings yet
- Anytime I Don'T Remember Something From Uworld, I Go Straight To MemorangDocument3 pagesAnytime I Don'T Remember Something From Uworld, I Go Straight To MemorangRa ViNo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Week 2Document5 pagesWeek 2Maica LectanaNo ratings yet
- Uro Spots SummaryDocument25 pagesUro Spots Summarynthabiseng maboganaNo ratings yet
- SystemicSclerosis GastrointestinalDiseaseandIts ManagementDocument15 pagesSystemicSclerosis GastrointestinalDiseaseandIts ManagementMércia FonsecaNo ratings yet
- Kuliah Trauma Urologi - DR WibisonoDocument34 pagesKuliah Trauma Urologi - DR WibisonoAgung Budi SuristioNo ratings yet
- Gastroenterology PancreatitisDocument1 pageGastroenterology PancreatitisNour SamadNo ratings yet
- Osacicon Poster Annular PancreasDocument1 pageOsacicon Poster Annular PancreasAbhishek Soham SatpathyNo ratings yet
- OMEPRAZOLEDocument2 pagesOMEPRAZOLERea LynNo ratings yet
- ARF PathoDocument3 pagesARF PathoNikki RodrigoNo ratings yet
- Peptic Ulcer DiseaseDocument119 pagesPeptic Ulcer DiseaseJoy LacunaNo ratings yet
- Case Pre Drug StudyDocument22 pagesCase Pre Drug StudyBenjie DimayacyacNo ratings yet
- Poster Vishnu Semi Copy2Document1 pagePoster Vishnu Semi Copy2sri harshaNo ratings yet
- Gastrointestinal OsmosisDocument174 pagesGastrointestinal OsmosisfabicontrerasenarmNo ratings yet
- Acute PancreatitisDocument8 pagesAcute PancreatitisAthan AntonioNo ratings yet
- Surgical Masters TacticsDocument7 pagesSurgical Masters TacticsaizatamlikhaNo ratings yet
- Drug StudyDocument3 pagesDrug StudyalysNo ratings yet
- CHOLANGITISDocument7 pagesCHOLANGITISWill GutierrezNo ratings yet
- MS-2 GallbladderDocument2 pagesMS-2 Gallbladderelijahdale.guillergan-05No ratings yet
- Nursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationDocument2 pagesNursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationOmar IzzoNo ratings yet
- Disorders of PancreasDocument43 pagesDisorders of Pancreasindu mathiNo ratings yet
- Pathophysiology CholeDocument3 pagesPathophysiology CholeClyde AleczandreNo ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- Complications: Acute PancreatitisDocument2 pagesComplications: Acute PancreatitisNikey LimNo ratings yet
- History: Clinical ManifestationsDocument2 pagesHistory: Clinical ManifestationsNikey LimNo ratings yet
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseNikey LimNo ratings yet
- Resp 3Document2 pagesResp 3Nikey LimNo ratings yet
- Ideas From The One-Minute Manager: Strategic ManagementDocument2 pagesIdeas From The One-Minute Manager: Strategic ManagementNikey LimNo ratings yet
- Sleep-Related Upper Airway Obstruction in ChildrenDocument1 pageSleep-Related Upper Airway Obstruction in ChildrenNikey LimNo ratings yet
- Paeds Surgery 1Document2 pagesPaeds Surgery 1Nikey LimNo ratings yet
- Resp 1Document2 pagesResp 1Nikey LimNo ratings yet
- Section 03 Concepts of Family MedicineDocument2 pagesSection 03 Concepts of Family MedicineNikey LimNo ratings yet
- Section 04: Being A ManagerDocument2 pagesSection 04: Being A ManagerNikey LimNo ratings yet
- Care of The Patient and His FamilyDocument2 pagesCare of The Patient and His FamilyNikey LimNo ratings yet
- Doctor/Patient Communication: Family SupportDocument2 pagesDoctor/Patient Communication: Family SupportNikey LimNo ratings yet
- Inborn Errors of MetabolismDocument2 pagesInborn Errors of MetabolismNikey LimNo ratings yet
- Heart Failure 1Document2 pagesHeart Failure 1Nikey LimNo ratings yet
- Bradycardia and Conduction Disorders Sinus Bradycardia (Fig. 1.6)Document2 pagesBradycardia and Conduction Disorders Sinus Bradycardia (Fig. 1.6)Nikey LimNo ratings yet
- Arrhythmia 3Document2 pagesArrhythmia 3Nikey LimNo ratings yet
- Respiratory DiseaseDocument1 pageRespiratory DiseaseNikey LimNo ratings yet
- Proteus: Boys Girls (Form Phosphate Stone) Pseudomonas: Structural Abnormality in UT Plastic CathetersDocument2 pagesProteus: Boys Girls (Form Phosphate Stone) Pseudomonas: Structural Abnormality in UT Plastic CathetersNikey LimNo ratings yet
- Data StreamDocument87 pagesData StreamL-Va AndesNo ratings yet
- PhysAssessAbdomen 1Document21 pagesPhysAssessAbdomen 1David DvoskineNo ratings yet
- Management of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeDocument13 pagesManagement of Incidental Pancreatic Cysts: A White Paper of The ACR Incidental Findings CommitteeSole GonzalezNo ratings yet
- Cancer Self TreatmentDocument35 pagesCancer Self TreatmentRichard HoltNo ratings yet
- CF NutritionDocument288 pagesCF Nutritionrkuip960% (1)
- Uji Efek Ekstrak Etanol Kulit Terung Ungu Terhadap Gambaran Histopatologi Pankreas Tikus Putih JantanDocument10 pagesUji Efek Ekstrak Etanol Kulit Terung Ungu Terhadap Gambaran Histopatologi Pankreas Tikus Putih Jantanridho kNo ratings yet
- AP-2 Lab Report - Lab 01 The Endrocine SystemDocument15 pagesAP-2 Lab Report - Lab 01 The Endrocine Systemrcdunfee86% (7)
- Cholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarDocument25 pagesCholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarMc Crister Silang100% (1)
- Redox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsDocument6 pagesRedox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsEdisher TsivtsivadzeNo ratings yet
- BAB I PancreatoblastomaDocument5 pagesBAB I PancreatoblastomaHana YunikoNo ratings yet
- The Digestive System: Ontent Earning CtivityDocument18 pagesThe Digestive System: Ontent Earning CtivityCamille Ann Faigao FamisanNo ratings yet
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- Literature Review On Prevalence of Diabetes MellitusDocument8 pagesLiterature Review On Prevalence of Diabetes MellitusnnactlvkgNo ratings yet
- Annular Pancreas Divisumtreated With Whipple Procedure: A Case Reportand Update of Arare ConditionDocument5 pagesAnnular Pancreas Divisumtreated With Whipple Procedure: A Case Reportand Update of Arare ConditionIJAR JOURNALNo ratings yet
- Surgery 2 PancreasDocument28 pagesSurgery 2 PancreasPARADISE JanoNo ratings yet
- Full Download Test Bank For Krauses Food and The Nutrition Care Process 14th Edition by Mahan PDF Full ChapterDocument36 pagesFull Download Test Bank For Krauses Food and The Nutrition Care Process 14th Edition by Mahan PDF Full Chaptercentimedisallyj0v47y100% (21)
- Histologia de PeixesDocument139 pagesHistologia de PeixesLetícia S. de CarvalhoNo ratings yet
- Sorted Feedback TopicwiseDocument55 pagesSorted Feedback TopicwiseLokesh BakshiNo ratings yet
- AIFSET 2021 Exam PaperDocument17 pagesAIFSET 2021 Exam Paperreshu.reshumiNo ratings yet
- Acute PancreatitisDocument39 pagesAcute PancreatitisJm Bernardo100% (1)
- 2.4.4.5c Acute PancreatitisDocument38 pages2.4.4.5c Acute PancreatitisAlfathush ShalihahNo ratings yet
- OCR A A-Level Biology Retrieval Roulette COMPLETEDocument115 pagesOCR A A-Level Biology Retrieval Roulette COMPLETEtikif31811No ratings yet
- Digestive System ReviewerDocument2 pagesDigestive System ReviewerDivino BauzonNo ratings yet
- Surgical Approach To Peritonitis and Abdominal Sepsis - Background, Preoperative Preparation, Considerations For Surgical ManagementDocument8 pagesSurgical Approach To Peritonitis and Abdominal Sepsis - Background, Preoperative Preparation, Considerations For Surgical ManagementCiubuc AndrianNo ratings yet
- PassAMCQ Study Companion 21Document30 pagesPassAMCQ Study Companion 21nitesawakeningNo ratings yet