You might also like
- Topic 6 IB TB Questions and AnswersDocument33 pagesTopic 6 IB TB Questions and Answersgeorgia92% (12)
- Pediatric Critical Care Nutrition PDFDocument324 pagesPediatric Critical Care Nutrition PDFNia DefinisiNo ratings yet
- DKADocument6 pagesDKAtiffarub91% (11)
- Diabetic Ketoacidosis Hypoglycemia: DR MD Mamunul Abedin ShimulDocument18 pagesDiabetic Ketoacidosis Hypoglycemia: DR MD Mamunul Abedin ShimulDr. Mamunul AbedinNo ratings yet
- Transfusions and BloodDocument48 pagesTransfusions and BloodMark Hammerschmidt100% (1)
- Euglycemic DkaDocument15 pagesEuglycemic DkaVemuri SrinivasNo ratings yet
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinNo ratings yet
- DKA Canadian ProtocolDocument2 pagesDKA Canadian Protocolplay_wright2084No ratings yet
- Type 1 Diabetes: Diabetic Ketoacidos ISDocument16 pagesType 1 Diabetes: Diabetic Ketoacidos ISapi-551073862No ratings yet
- Respiratory Distress SyndromeDocument54 pagesRespiratory Distress SyndromeKristine CaringalNo ratings yet
- Hypoglycemia, Hyperosmolar Hyperglycaemic State (HHS) and Diabetic Ketoacidosis (Dka)Document30 pagesHypoglycemia, Hyperosmolar Hyperglycaemic State (HHS) and Diabetic Ketoacidosis (Dka)kuncupcupu1368No ratings yet
- Neonatal Respiratory Distress SyndromeDocument4 pagesNeonatal Respiratory Distress SyndromePahw BaluisNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument8 pagesHyperosmolar Hyperglycemic StateEsra AljafferNo ratings yet
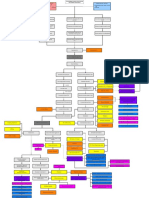
- Conceptual Map - Diabetic KetoacidosisDocument2 pagesConceptual Map - Diabetic KetoacidosisLovie Japhet LopezNo ratings yet
- Management of Diabetes Ketoacidosis in PregnancyDocument19 pagesManagement of Diabetes Ketoacidosis in PregnancySudhir PaulNo ratings yet
- DKA Draft 1 AM - Drawio 2Document1 pageDKA Draft 1 AM - Drawio 2Dud AccNo ratings yet
- Infant Respiratory Distress SyndromeDocument39 pagesInfant Respiratory Distress SyndromeIoana MuntianuNo ratings yet
- Respiratory Distress Syndrome - MBCHBDocument23 pagesRespiratory Distress Syndrome - MBCHBMalueth AnguiNo ratings yet
- EMTDocument73 pagesEMTLovely Acabado TampocoNo ratings yet
- Diabetic Ketoacidosis Demystified: Doctor's Secret GuideFrom EverandDiabetic Ketoacidosis Demystified: Doctor's Secret GuideNo ratings yet
- SGLT2i Beyond Glycemic ControlDocument55 pagesSGLT2i Beyond Glycemic ControlSwapnaNo ratings yet
- Management of Diabetes Emergencies''Document85 pagesManagement of Diabetes Emergencies''Princewill SeiyefaNo ratings yet
- CBT - Emergency Medicine EditedDocument14 pagesCBT - Emergency Medicine Editedchristy INo ratings yet
- Dka and HHSDocument25 pagesDka and HHSMouhammad Dawoud100% (2)
- Stroke EmergencyDocument56 pagesStroke EmergencyNachchakorn Dell100% (1)
- Carboplatin MonographDocument9 pagesCarboplatin Monographmerkuri100% (1)
- Diabetic KetoasidosisDocument33 pagesDiabetic KetoasidosisGrace UlyNo ratings yet
- Demensia Vs AlzheimerDocument16 pagesDemensia Vs AlzheimerUmmu ZaFaNo ratings yet
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDocument1 pageDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- Hospital Management System SoftwareDocument11 pagesHospital Management System SoftwareNikesh Solanki50% (2)
- Seizures in Children JULIO 2020Document29 pagesSeizures in Children JULIO 2020Elizabeth HendersonNo ratings yet
- Wound Care-Std1 1Document42 pagesWound Care-Std1 1twy113No ratings yet
- DKA and HHSDocument16 pagesDKA and HHSGepengCungkringNo ratings yet
- Tubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterDocument11 pagesTubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterJeremy HamptonNo ratings yet
- Ambulatory Care NursingDocument5 pagesAmbulatory Care NursingKim TanNo ratings yet
- Hypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TDocument44 pagesHypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TUsaid SulaimanNo ratings yet
- Clinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephDocument15 pagesClinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephArmeen AminNo ratings yet
- B U F N & H S N: Advanced Medical Surgical NURS 337 " Emergency Department Report "Document16 pagesB U F N & H S N: Advanced Medical Surgical NURS 337 " Emergency Department Report "Yousef JafarNo ratings yet
- Acute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoDocument20 pagesAcute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoGüids GalliganiNo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
- The Nurse in The Emergency Department Is Caring For A Patient With A PartialDocument13 pagesThe Nurse in The Emergency Department Is Caring For A Patient With A Partialhasan ahmdNo ratings yet
- Geria - CardioDocument4 pagesGeria - CardioLeah GordoncilloNo ratings yet
- S. 14.0 Fluid Therapy - Trauma CasesDocument7 pagesS. 14.0 Fluid Therapy - Trauma CasesroropujiNo ratings yet
- Rash BookDocument12 pagesRash BookPhoebe UsmleNo ratings yet
- Chronic Kidney Disease Demystified: Doctor’s Secret GuideFrom EverandChronic Kidney Disease Demystified: Doctor’s Secret GuideNo ratings yet
- Dialysis: Hemodialysis (HD) Peritoneal Dialysis (PD)Document66 pagesDialysis: Hemodialysis (HD) Peritoneal Dialysis (PD)joms_pasanoNo ratings yet
- Haemodynamic MonitoringDocument128 pagesHaemodynamic MonitoringDr. KNo ratings yet
- ShockDocument35 pagesShocktrip100No ratings yet
- Adult Nursing Skills On Complex CareDocument16 pagesAdult Nursing Skills On Complex CareNaftali OumaNo ratings yet
- Caleb KestnerDocument52 pagesCaleb KestnerCaleb Alan Kestner100% (2)
- Common Lab ValuesDocument4 pagesCommon Lab ValuesRaf LuisNo ratings yet
- Cellulitis in Adults - Guideline Flowchart Hospital in The Home Guideline For Management at HomeDocument2 pagesCellulitis in Adults - Guideline Flowchart Hospital in The Home Guideline For Management at HomeAnonymous 4txA8N8etNo ratings yet
- Periprocedural Anticoagulation GuidelineDocument14 pagesPeriprocedural Anticoagulation GuidelineTeky WidyariniNo ratings yet
- Hemodialysis FinalDocument40 pagesHemodialysis Finalrose FolwersNo ratings yet
- Type 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsDocument6 pagesType 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsTrifosa Ika Septiana EryaniNo ratings yet
- Pediatric DKA: Section I: Scenario DemographicsDocument8 pagesPediatric DKA: Section I: Scenario DemographicsSherein ShalabyNo ratings yet
- Management of Diabetes MellitusDocument42 pagesManagement of Diabetes Mellitusayu ersa lestari100% (1)
- Acid-Base Disorders NotesDocument10 pagesAcid-Base Disorders NotesLovely100% (1)
- Rekap Pasien Graha INCOVIT Minggu, 08 Agustus 2021Document25 pagesRekap Pasien Graha INCOVIT Minggu, 08 Agustus 2021Muhammad BilalNo ratings yet
- Mr. S/67 Yo/bengawan Solo WardDocument27 pagesMr. S/67 Yo/bengawan Solo WardMuhammad BilalNo ratings yet
- Effect of Poorly Absorbable Antibiotics On Hepatic Venous PressureDocument8 pagesEffect of Poorly Absorbable Antibiotics On Hepatic Venous PressureMuhammad BilalNo ratings yet
- Guias ESC para Insuficiencia Cardiaca CronicaDocument128 pagesGuias ESC para Insuficiencia Cardiaca CronicaKarla HernandezNo ratings yet
- Evidence Based Medicine and Practice: Critical Appraisal of Prognostic StudiesDocument2 pagesEvidence Based Medicine and Practice: Critical Appraisal of Prognostic StudiesMuhammad BilalNo ratings yet
- Guidelines For The Management of Hemophilia: 2 EditionDocument80 pagesGuidelines For The Management of Hemophilia: 2 EditionMuhammad BilalNo ratings yet
- Pulmonary Edema. A Complication of Diabetic KetoacidosisDocument2 pagesPulmonary Edema. A Complication of Diabetic KetoacidosisMuhammad BilalNo ratings yet
- Euglycemic Diabetic KetoacidosisDocument6 pagesEuglycemic Diabetic KetoacidosisMuhammad BilalNo ratings yet
- IJV Collapsibility Index Vs IVC Collapsibility IndexDocument11 pagesIJV Collapsibility Index Vs IVC Collapsibility IndexMuhammad BilalNo ratings yet
- A18 - KAD HHS - FullDocument9 pagesA18 - KAD HHS - FullMuhammad BilalNo ratings yet
- A03 - Guideline 2016 Myelodysplastic Syndromes (MDS) - Jurnal Hong 2017Document5 pagesA03 - Guideline 2016 Myelodysplastic Syndromes (MDS) - Jurnal Hong 2017Muhammad BilalNo ratings yet
- Physiology (Compatibility Mode) - 1Document40 pagesPhysiology (Compatibility Mode) - 1ahmad aliNo ratings yet
- 05 05 NOTES-HormonalDocument3 pages05 05 NOTES-HormonalSidney TyNo ratings yet
- Chapter Sixteen Cell SignalingDocument96 pagesChapter Sixteen Cell SignalingRu LiliNo ratings yet
- Relevance of Yoga Through Paschimottanasana On Type 2 Diabetes Mellitus - A Literature ReviewDocument11 pagesRelevance of Yoga Through Paschimottanasana On Type 2 Diabetes Mellitus - A Literature ReviewAbheek BardhanNo ratings yet
- Control and Coordination Chapter 1 Notes For Class 10 WBBSE - Ranjan ShawDocument12 pagesControl and Coordination Chapter 1 Notes For Class 10 WBBSE - Ranjan ShawRanjan ShawNo ratings yet
- Biochemistry Revalida 2021Document30 pagesBiochemistry Revalida 2021RM DulawanNo ratings yet
- IGCSE 0610 - Body Temperature and Gluco-RegulationDocument4 pagesIGCSE 0610 - Body Temperature and Gluco-Regulationckqx1234No ratings yet
- The Pathogenesis and Pathophysiology of Type 1 and PDFDocument12 pagesThe Pathogenesis and Pathophysiology of Type 1 and PDFasmawatiNo ratings yet
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocument69 pagesPancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNo ratings yet
- Biochemistry of HormonesDocument22 pagesBiochemistry of HormonesShaira Elyze GabrielNo ratings yet
- Glycogen MetabolismDocument17 pagesGlycogen Metabolismmags wagsNo ratings yet
- TYS Unit 2.7Document3 pagesTYS Unit 2.7prameetaNo ratings yet
- Homeostasis: Test Yourself 12.1 (Page 246)Document3 pagesHomeostasis: Test Yourself 12.1 (Page 246)lee100% (1)
- Handy Health Guide To DiabetesDocument49 pagesHandy Health Guide To DiabetesDiabetes Care100% (1)
- MCQ Questions AnswersDocument49 pagesMCQ Questions AnswersKajaNo ratings yet
- SIM Biochemistry ULO3Document31 pagesSIM Biochemistry ULO3Darl MalazarteNo ratings yet
- Endocrine ResonanceDocument51 pagesEndocrine ResonanceEkta ManglaniNo ratings yet
- G D Goenka Public School, Agra Session 2023 - 24 Class - XI, Winter Holiday HomeworkDocument41 pagesG D Goenka Public School, Agra Session 2023 - 24 Class - XI, Winter Holiday HomeworkPrince ParasharNo ratings yet
- 2012 Hormonal Regulation in Nutrients MetabolismDocument20 pages2012 Hormonal Regulation in Nutrients Metabolismatika_asti_pNo ratings yet
- Endocrinology Module Study Guide 2023 FinalDocument24 pagesEndocrinology Module Study Guide 2023 Finaldomitam105No ratings yet
- Physiology MCQDocument32 pagesPhysiology MCQdip171100% (4)
- Carbohydrates (CHO)Document190 pagesCarbohydrates (CHO)Mustafa KhandgawiNo ratings yet
- Diabetic Ketoacidosis: Pathophysiology and Treatment Diabetic Ketoacidosis: Pathophysiology and TreatmentDocument10 pagesDiabetic Ketoacidosis: Pathophysiology and Treatment Diabetic Ketoacidosis: Pathophysiology and TreatmentmirzaNo ratings yet
- Mark Scheme (Results) : Summer 2018Document11 pagesMark Scheme (Results) : Summer 2018Bara' HammadehNo ratings yet
- Chapter 18 Homeostasis (Summary)Document2 pagesChapter 18 Homeostasis (Summary)橙歌、No ratings yet
- Hyperglucemiia in NeonateDocument11 pagesHyperglucemiia in Neonateopix999100% (1)
- 1 6 Regulation of Blood Glucose PDFDocument3 pages1 6 Regulation of Blood Glucose PDFtiaraNo ratings yet
- Lesson 7 Glucose HomeostasisDocument39 pagesLesson 7 Glucose Homeostasissaja MuhammadNo ratings yet