Download as pdf or txt
You might also like
- Orange Juice SongbookDocument60 pagesOrange Juice SongbookLewis BlossNo ratings yet
- Virtual Memory Lab-2Document14 pagesVirtual Memory Lab-2Hafiz Muhammad Umar Aslam0% (1)
- Ankle FractureDocument87 pagesAnkle FractureStar Cruise100% (1)
- "Let Not The Failure and The Pain Turn Aside The WorshippersDocument35 pages"Let Not The Failure and The Pain Turn Aside The Worshipperspdavidthomas100% (1)
- Ritual of The Rose Cross (Golden Dawn)Document4 pagesRitual of The Rose Cross (Golden Dawn)solomon5678No ratings yet
- St. Paul's Motion To Dismiss and OrderDocument5 pagesSt. Paul's Motion To Dismiss and OrderKentFaulkNo ratings yet
- Lecture 2 Unit VIDocument53 pagesLecture 2 Unit VIRiya AdhangleNo ratings yet
- Adult-Acquired Flatfoot DeformityDocument27 pagesAdult-Acquired Flatfoot DeformityNajeeb BsoulNo ratings yet
- Orthopedics Standard of Care GuidelinesDocument543 pagesOrthopedics Standard of Care GuidelinesppeterarmstrongNo ratings yet
- Achilles RuptureDocument23 pagesAchilles RupturePhysiotherapist AliNo ratings yet
- Anatomy Biomechanics of AnkleDocument82 pagesAnatomy Biomechanics of AnklelypiheNo ratings yet
- Departement of Orthopaedic and TraumatologyDocument89 pagesDepartement of Orthopaedic and TraumatologyMukhizalNo ratings yet
- Pengayaan Koass Ortho - Update 5 VersionDocument122 pagesPengayaan Koass Ortho - Update 5 Versionanon_967171484No ratings yet
- Ankle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTDocument28 pagesAnkle Fractures: Winda Alviranisa/20204010293 Pembimbing: Dr. Muhammad Pandu Nugraha, SP - OTwinda alviraNo ratings yet
- The KneeDocument57 pagesThe Kneeniamh traceyNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- Assessment of KneeDocument113 pagesAssessment of KneeIqra Iftikhar100% (1)
- Wrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptDocument59 pagesWrist / Fingers Injuries: DR - Shafaq Shahid Lecturer DPT, Ms-OmptNabiha AjmalNo ratings yet
- Tuberculosis of Knee: Presented By: DR Dipendra Maharjan 2 Yr Resident, MS Orthopaedics NAMS, Bir HospitalDocument25 pagesTuberculosis of Knee: Presented By: DR Dipendra Maharjan 2 Yr Resident, MS Orthopaedics NAMS, Bir HospitalshravaniNo ratings yet
- Ankle Fractures: Dr. T. VikramDocument35 pagesAnkle Fractures: Dr. T. VikramVicky VikramNo ratings yet
- Foot and Ankle Injuries Kylee Phillips - 0Document74 pagesFoot and Ankle Injuries Kylee Phillips - 0Charlez OhanuNo ratings yet
- Lecture 13 Bone, Joint, Tendon, and Soft Tissue Injury in Lower Limb (Knee)Document143 pagesLecture 13 Bone, Joint, Tendon, and Soft Tissue Injury in Lower Limb (Knee)Wilson HalimNo ratings yet
- Foot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDDocument55 pagesFoot and Ankle Injuries and Pain: Indranil Neel' Kushare, MDrizwan.mughal1997No ratings yet
- Musculoskeletal SystemDocument44 pagesMusculoskeletal Systemayesharajput5110No ratings yet
- Nur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin PalembangDocument38 pagesNur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin Palembangsoleha09la solehaNo ratings yet
- Musculoskeletal SystemDocument44 pagesMusculoskeletal SystemHasnat AhmedNo ratings yet
- MCHT Leading and Managing Your Organisation Musculoskeletal Education IC3Document49 pagesMCHT Leading and Managing Your Organisation Musculoskeletal Education IC3nickmirad2No ratings yet
- New Introduction To Ortho 1 Jan 20016Document67 pagesNew Introduction To Ortho 1 Jan 20016BIOLOGY BY ISMAIL ANSARINo ratings yet
- Facture/Dislocation: R I C EDocument23 pagesFacture/Dislocation: R I C EKrishnamurti KambleNo ratings yet
- Emergency in Orthopaedic: Dr. Primadika Rubiansyah, SpotDocument37 pagesEmergency in Orthopaedic: Dr. Primadika Rubiansyah, SpotMuhammad DzulfikarNo ratings yet
- Ankle Sprain TreatmentDocument5 pagesAnkle Sprain TreatmentTushar GajjarNo ratings yet
- Knee Examination OSCE GuideDocument23 pagesKnee Examination OSCE GuideAaron Nameer Abrar RahmanNo ratings yet
- Common CasesDocument44 pagesCommon CasesRebecca WongNo ratings yet
- Club Foot-Dr J SahooDocument9 pagesClub Foot-Dr J SahooSheel Gupta100% (1)
- Foot and Ankle Injuries Kylee Phillips - 0Document74 pagesFoot and Ankle Injuries Kylee Phillips - 0rizwan.mughal1997No ratings yet
- MusculoskeletalDocument77 pagesMusculoskeletalMiden AlbanoNo ratings yet
- Principles Fracture ManagementDocument88 pagesPrinciples Fracture ManagementYauffa Hanna Elt MisykahNo ratings yet
- Introduction To The Musculoskeletal SystemDocument39 pagesIntroduction To The Musculoskeletal SystemdesyNo ratings yet
- Musculoskeletal System AssessmentDocument75 pagesMusculoskeletal System AssessmentRolinette DaneNo ratings yet
- Physical Assessment MSK Level 3 2019Document93 pagesPhysical Assessment MSK Level 3 2019Daniela OrtalNo ratings yet
- Dr. Muh. Sakti SpotDocument25 pagesDr. Muh. Sakti SpotTiti Afrida SariNo ratings yet
- Types of FractureDocument11 pagesTypes of FractureDimple Castañeto CalloNo ratings yet
- Orthopaedics Diagnosis & Therapy: Dr. Su Djie To Rante, M.Biomed, SP - OTDocument75 pagesOrthopaedics Diagnosis & Therapy: Dr. Su Djie To Rante, M.Biomed, SP - OTDiana MarcusNo ratings yet
- Musculoskeletal Disorders: Aurang ZebDocument73 pagesMusculoskeletal Disorders: Aurang ZebMuhammadNo ratings yet
- Fractures and Dislocations of The Mid-Foot Including Lisfranc InjuriesDocument67 pagesFractures and Dislocations of The Mid-Foot Including Lisfranc Injuriesmaria_meNo ratings yet
- Sport Traumatology-III Foot and Ankle Joint-15Document47 pagesSport Traumatology-III Foot and Ankle Joint-15kamran aliNo ratings yet
- Malleolar Fractures - Handout PDFDocument14 pagesMalleolar Fractures - Handout PDFAlin Bratu100% (2)
- Fractures and DislocationsDocument53 pagesFractures and Dislocationsagha_sajjad90No ratings yet
- 10 - Musculoskeletal InjuriesDocument8 pages10 - Musculoskeletal InjuriesEastern SamarNo ratings yet
- GALS Screen: G Gait A Arms L Legs S SpineDocument6 pagesGALS Screen: G Gait A Arms L Legs S SpineJoseph FreerNo ratings yet
- MSK PDFDocument90 pagesMSK PDFJay Rome100% (1)
- Ankle FracturesDocument41 pagesAnkle Fracturesshammasbm100% (12)
- Group 7 LMRDocument32 pagesGroup 7 LMRQamar AhmedNo ratings yet
- Osteoarthritis: Dr. C. C. VisserDocument85 pagesOsteoarthritis: Dr. C. C. VisserAhmad Fathira FitraNo ratings yet
- Musculoskeletal Examination Under GraduatesDocument98 pagesMusculoskeletal Examination Under GraduatesEsraa SalemNo ratings yet
- Ankle D.DDocument16 pagesAnkle D.Dمحمد عقلNo ratings yet
- Knee Anatomy and InjuriesDocument120 pagesKnee Anatomy and Injurieserfan mohammadi100% (2)
- Pes PlanusDocument18 pagesPes Planushacker ammerNo ratings yet
- Genu Valgus Genu VarusDocument35 pagesGenu Valgus Genu VarusRatu FaniaNo ratings yet
- 30.ankle & Foot DiseasesDocument46 pages30.ankle & Foot DiseasesDuha HamidNo ratings yet
- New Microsoft Power Point PresentationDocument20 pagesNew Microsoft Power Point PresentationAkram KhatriNo ratings yet
- ORP - Handout - English - Malleolar FracturesDocument15 pagesORP - Handout - English - Malleolar Fracturesadrian1989No ratings yet
- AnD FT Elbow-1Document26 pagesAnD FT Elbow-1Nazwa KamilatunnisaNo ratings yet
- Plantar Heel Pain, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPlantar Heel Pain, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Achilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAchilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Keep 425Document12 pagesKeep 425Johan SukweenadhiNo ratings yet
- 2003 Animal Rights AnswersDocument5 pages2003 Animal Rights AnswersVarshLokNo ratings yet
- Cronica Report Malcolm McLeanDocument2 pagesCronica Report Malcolm McLeanomar andres rodriguez veraNo ratings yet
- Ethics of Student Final PDFDocument15 pagesEthics of Student Final PDFAmtul KafiNo ratings yet
- A Marriage Proposal by Anton ChekovDocument2 pagesA Marriage Proposal by Anton ChekovJade MBNo ratings yet
- Sample Essay Describe YourselfDocument4 pagesSample Essay Describe Yourselfafabfzoqr100% (2)
- Single Axis Solar Tracking System: (I) PurposeDocument23 pagesSingle Axis Solar Tracking System: (I) Purposeelectrical engineeringNo ratings yet
- Parasite - Global Issues - English LPDocument4 pagesParasite - Global Issues - English LPSiddhesh SoodNo ratings yet
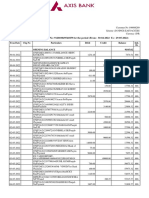
- Statement of Axis Account No:912010049541859 For The Period (From: 30-04-2022 To: 29-05-2022)Document5 pagesStatement of Axis Account No:912010049541859 For The Period (From: 30-04-2022 To: 29-05-2022)Rahul BansalNo ratings yet
- Practical Training ReportDocument6 pagesPractical Training ReportGorishsharmaNo ratings yet
- 9 CH 1 2024-25Document12 pages9 CH 1 2024-25Muhammad Abdullah ToufiqueNo ratings yet
- Working at Heights: Engr. Jobelle B MalaygayDocument50 pagesWorking at Heights: Engr. Jobelle B MalaygayJohn Cedrik Retardo100% (1)
- Nahla Youisf-ResumeDocument2 pagesNahla Youisf-ResumenahlaNo ratings yet
- Application of I4.0 and The Role of Sustainability in GCC Construction IndustryDocument14 pagesApplication of I4.0 and The Role of Sustainability in GCC Construction IndustryKanchan LakhwaniNo ratings yet
- MB Intel Server S3200SHDocument128 pagesMB Intel Server S3200SHZainal AbidinNo ratings yet
- System Requirements Autodesk Revit 2024Document8 pagesSystem Requirements Autodesk Revit 2024Alemat RedaeNo ratings yet
- 0610 BIOLOGY: MARK SCHEME For The October/November 2015 SeriesDocument2 pages0610 BIOLOGY: MARK SCHEME For The October/November 2015 Seriesmath magicNo ratings yet
- Nitrosamine Impurities - European Medicines AgencyDocument13 pagesNitrosamine Impurities - European Medicines Agencymarwaw7hNo ratings yet
- Recent Advances in The Synthesis of Pipe Rid Ones and Piperidines PM Weintraub JS Sabol JM Kane DR Borcherding Tetrahedron 59 2953 2989 2003Document37 pagesRecent Advances in The Synthesis of Pipe Rid Ones and Piperidines PM Weintraub JS Sabol JM Kane DR Borcherding Tetrahedron 59 2953 2989 2003KybernetikumNo ratings yet
- 102 - SCO8048A-Alert - Fixings-FinalDocument3 pages102 - SCO8048A-Alert - Fixings-FinalO SNo ratings yet
- Wireless Price ListDocument21 pagesWireless Price ListnboninaNo ratings yet
- Avaya G250 Media Gateway With An Avaya S8300 ServerDocument22 pagesAvaya G250 Media Gateway With An Avaya S8300 ServerRoberto MontagnanaNo ratings yet
- Welcome To Oneg ShabbatDocument19 pagesWelcome To Oneg ShabbatTovaNo ratings yet
- GX71 GX51 PDFDocument18 pagesGX71 GX51 PDFRepresentaciones y Distribuciones FALNo ratings yet
- Thermal Efficiency Fired HeaterDocument5 pagesThermal Efficiency Fired Heatermuhammad_asim_10No ratings yet