Download as docx, pdf, or txt
You might also like
- Post Operative-Teaching Care PlanDocument9 pagesPost Operative-Teaching Care PlanKit Lara88% (8)
- Chest PhysiotherapyDocument22 pagesChest Physiotherapyغيداء الذويبي100% (1)
- NCP CholeDocument8 pagesNCP CholeAndrewAlvinTemploNo ratings yet
- Balance Skeletal TractionDocument4 pagesBalance Skeletal TractionIris BalinoNo ratings yet
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- Hubli Bye LawsDocument17 pagesHubli Bye LawsShrinivas Sonnad100% (3)
- Marketing PlanDocument18 pagesMarketing PlannaphNo ratings yet
- Station User Panel Railway Station Useability PrinciplesDocument32 pagesStation User Panel Railway Station Useability PrinciplesVan Hong Tan80% (5)
- Preoperative Care: Patient EducationDocument11 pagesPreoperative Care: Patient Educationrence_8913100% (1)
- NSO Chest PhysiotherapyDocument5 pagesNSO Chest PhysiotherapyAlih KathlyannNo ratings yet
- Preop & Postop Nursing InterventionsDocument8 pagesPreop & Postop Nursing InterventionsLizethNo ratings yet
- 11 SurgeriesDocument11 pages11 SurgeriesJanely EstreraNo ratings yet
- SKILL: Chest PhysiotherapyDocument3 pagesSKILL: Chest PhysiotherapyArmie Joy Embat CariazoNo ratings yet
- Pre and OpDocument6 pagesPre and OpFatimah Alshareef100% (1)
- MS PeriopDocument4 pagesMS PeriopJinx GonNo ratings yet
- Inbound 4624314230825210461Document58 pagesInbound 4624314230825210461Roy AmataNo ratings yet
- Gowning, Gloving (Open and Closed Techniques-Unassisted)Document11 pagesGowning, Gloving (Open and Closed Techniques-Unassisted)Grape JuiceNo ratings yet
- Fon Model Test Paper With Answer KeyDocument7 pagesFon Model Test Paper With Answer KeyD Dimpy ThakurNo ratings yet
- Kozier's Peri Operative NSG ChecklistDocument15 pagesKozier's Peri Operative NSG ChecklistMichaelNo ratings yet
- Conduct-Of-Normal-Labor - LABISDocument2 pagesConduct-Of-Normal-Labor - LABISDianne LabisNo ratings yet
- Nursing Management in Abdominal SurgeryDocument19 pagesNursing Management in Abdominal Surgeryejguy7777100% (2)
- Nursing Responsibilities in The Care of Casts Traction FixatorsDocument20 pagesNursing Responsibilities in The Care of Casts Traction FixatorsBasmah A. AdompingNo ratings yet
- Critical Thinking Nursing Care LippincotsDocument35 pagesCritical Thinking Nursing Care Lippincotseric100% (1)
- Care of Surgical Patients - 1Document14 pagesCare of Surgical Patients - 1mr.moutkalanNo ratings yet
- Mobilization Protocols (As Being Performed in HospitalsDocument14 pagesMobilization Protocols (As Being Performed in HospitalsMuhammad asif samiNo ratings yet
- Module or JAKEDocument10 pagesModule or JAKEJake Yvan DizonNo ratings yet
- Chest Physiotherapy: ObjectivesDocument7 pagesChest Physiotherapy: ObjectivesstorageforiyangNo ratings yet
- Perioperative Concepts and Nursing Management: NCM 112-LecturerDocument98 pagesPerioperative Concepts and Nursing Management: NCM 112-LecturerJaylord Verazon100% (1)
- Assisting With A Liver BiopsyDocument8 pagesAssisting With A Liver BiopsyCharLie BlackNo ratings yet
- Procedure Checklist Chapter 35: Performing Percussion, Vibration, and Postural DrainageDocument2 pagesProcedure Checklist Chapter 35: Performing Percussion, Vibration, and Postural DrainagejthsNo ratings yet
- 1F Procedure Guide (CAUSIN)Document12 pages1F Procedure Guide (CAUSIN)CAUSIN, Lance Matthew,No ratings yet
- Nursing Care of Client During Labor and Delivery 1Document8 pagesNursing Care of Client During Labor and Delivery 1Arcel SasaluyaNo ratings yet
- 4.3 Respi. Percussion VibrationDocument8 pages4.3 Respi. Percussion VibrationRiza Angela BarazanNo ratings yet
- Thora Procedure 1Document10 pagesThora Procedure 1E PadzNo ratings yet
- Occupational First AidDocument12 pagesOccupational First AidEddie Bulwayan Endeken Jr.No ratings yet
- Nusing Skills Output (Nso)Document3 pagesNusing Skills Output (Nso)leroux2890No ratings yet
- Surgery: Cholecystectomy: Mariano Marcos State UniversityDocument23 pagesSurgery: Cholecystectomy: Mariano Marcos State UniversityFrancine JoseNo ratings yet
- Postural Drainage and PercussionDocument4 pagesPostural Drainage and Percussionhsk_khalsaNo ratings yet
- Transfer of A PatientDocument8 pagesTransfer of A Patienttrupti patelNo ratings yet
- Cesarean DeliveryDocument6 pagesCesarean DeliveryShella Marie UsquisaNo ratings yet
- Operating Room ConceptsDocument47 pagesOperating Room ConceptsLoungayvan Batuyog100% (1)
- Pre-Lecture I. You Are The Provider: Chapter 4: Lifting and Moving PatientsDocument9 pagesPre-Lecture I. You Are The Provider: Chapter 4: Lifting and Moving PatientsJasonJejametNo ratings yet
- Demo ChecklistDocument4 pagesDemo ChecklistDanielle Audrey BanNo ratings yet
- Different of Position For Medical ExaminationDocument19 pagesDifferent of Position For Medical ExaminationQueeny Anne Apil100% (1)
- The Application of A Continuous Strip of Woven Material To A Body PartDocument15 pagesThe Application of A Continuous Strip of Woven Material To A Body Partczeremar chanNo ratings yet
- Peri Operative NursingDocument22 pagesPeri Operative NursingIvyBanez100% (1)
- Lesson 2 Chest Physiotherapy Incentive Spirometry Chest DrainageDocument14 pagesLesson 2 Chest Physiotherapy Incentive Spirometry Chest DrainageRENEROSE TORRESNo ratings yet
- HERNIORRHAPYDocument2 pagesHERNIORRHAPYYessaminNo ratings yet
- WORKSHEET For Unit 14 On PEDIATRIC MUSCULOSKELETAL DISORDERSDocument14 pagesWORKSHEET For Unit 14 On PEDIATRIC MUSCULOSKELETAL DISORDERScorisNo ratings yet
- Client's Intake of Medications (E.g., Narcotics, Sedatives, Tranquilizers, andDocument6 pagesClient's Intake of Medications (E.g., Narcotics, Sedatives, Tranquilizers, and하나No ratings yet
- NP3 SET A With AnswersDocument11 pagesNP3 SET A With AnswersMiss GNo ratings yet
- Diagnostic ExamDocument19 pagesDiagnostic ExamChannelGNo ratings yet
- 3 Intraoperative PhaseDocument28 pages3 Intraoperative Phaseada_beer100% (2)
- Explain To The Patient The Purpose of Lumbar Puncture, How and Where It's Done, and Who Will Perform The ProcedureDocument3 pagesExplain To The Patient The Purpose of Lumbar Puncture, How and Where It's Done, and Who Will Perform The ProcedureChristian Anthony L. GamoloNo ratings yet
- AKTIVITAS NantaDocument40 pagesAKTIVITAS Nantapradnyadewi2005No ratings yet
- Clinical Practicum 100.Pptx11Document24 pagesClinical Practicum 100.Pptx11krezelflores2No ratings yet
- Care of Patients With Traction TractionDocument5 pagesCare of Patients With Traction TractionMOHAMMAD JABBER M. PAUDACJRNo ratings yet
- Perioperative or TechDocument11 pagesPerioperative or TechCezanne Danabelle HutallaNo ratings yet
- Perioperative Nursing NotesDocument13 pagesPerioperative Nursing NotesJuliana Lourdes V. CañadaNo ratings yet
- Deep Breath JADIDocument3 pagesDeep Breath JADIKucing ViralNo ratings yet
- Pelvic Traction SlingDocument3 pagesPelvic Traction SlingryanNo ratings yet
- If they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.From EverandIf they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.No ratings yet
- Week 4 - The Nursing ProcessDocument10 pagesWeek 4 - The Nursing ProcessMiss VinaNo ratings yet
- Week 12 - Fluids, Electrolytes and Acid-Base BalanceDocument10 pagesWeek 12 - Fluids, Electrolytes and Acid-Base BalanceMiss VinaNo ratings yet
- Week 11 - Oxygenation, Circulation, Loss, Grieving and DeathDocument10 pagesWeek 11 - Oxygenation, Circulation, Loss, Grieving and DeathMiss VinaNo ratings yet
- Week 5 - Vital Signs and AsepsisDocument16 pagesWeek 5 - Vital Signs and AsepsisMiss VinaNo ratings yet
- Week 1 - The Nature of NursingDocument7 pagesWeek 1 - The Nature of NursingMiss VinaNo ratings yet
- Week 3 - Health, Wellness and IllnessDocument6 pagesWeek 3 - Health, Wellness and IllnessMiss VinaNo ratings yet
- Week 2 - The Integral Aspects of NursingDocument5 pagesWeek 2 - The Integral Aspects of NursingMiss VinaNo ratings yet
- Sleep, Pain Management and NutritionDocument36 pagesSleep, Pain Management and NutritionMiss VinaNo ratings yet
- Week 3Document21 pagesWeek 3Miss VinaNo ratings yet
- Fluid, Electrolyte and Acid-Base BalanceDocument42 pagesFluid, Electrolyte and Acid-Base BalanceMiss Vina100% (1)
- The Integral Aspects of NursingDocument26 pagesThe Integral Aspects of NursingMiss VinaNo ratings yet
- Week 1Document31 pagesWeek 1Miss VinaNo ratings yet
- CE Project-WheelchairDocument24 pagesCE Project-WheelchairHemanth YenniNo ratings yet
- A Home Exercise BookDocument28 pagesA Home Exercise BookNameeta Shroff JainNo ratings yet
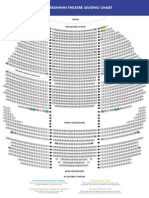
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- Literarure StudyDocument41 pagesLiterarure StudyAmit KumarNo ratings yet
- Requirements For Urban Buses in New ZealandDocument48 pagesRequirements For Urban Buses in New ZealandasdfNo ratings yet
- 01 IntroductionDocument43 pages01 IntroductionkhagendraNo ratings yet
- Full Textbook - CHCCCS011Document62 pagesFull Textbook - CHCCCS011Kabita123 NepzzNo ratings yet
- Sky Chair-Iot DescriptionDocument4 pagesSky Chair-Iot DescriptionMTBowers67No ratings yet
- Airports Authority of India PRM Handbook, 2019Document117 pagesAirports Authority of India PRM Handbook, 2019Radhika v-sheshNo ratings yet
- 110id0625 18 PDFDocument40 pages110id0625 18 PDFPatel RonakNo ratings yet
- Hyundai Walking CarDocument2 pagesHyundai Walking CarAswani B RajNo ratings yet
- Voice Recognition Based Intelligent Wheelchair and Gps Tracking SystemDocument6 pagesVoice Recognition Based Intelligent Wheelchair and Gps Tracking Systempraveenkammar9No ratings yet
- Ergometry: LT Book Für Inhouse-DruckDocument8 pagesErgometry: LT Book Für Inhouse-DruckjoseNo ratings yet
- Literature Review of Voice Controlled WheelchairDocument6 pagesLiterature Review of Voice Controlled Wheelchairfvhacvjd100% (1)
- Smart Chair SystemDocument10 pagesSmart Chair SystemyashNo ratings yet
- Design and Development of A Hand-Glove Controlled Wheel ChairDocument5 pagesDesign and Development of A Hand-Glove Controlled Wheel ChairAbdur RahmanNo ratings yet
- Chapter 4 - Technologies That Enable MobilityDocument48 pagesChapter 4 - Technologies That Enable Mobilitysara sallaqNo ratings yet
- Wheelchair FolderDocument30 pagesWheelchair FolderSyafiq Fauzi100% (1)
- Nursing Care Plan Sample 5Document13 pagesNursing Care Plan Sample 5GEN ERIGBUAGASNo ratings yet
- Mechanical Restraint ProceduresDocument15 pagesMechanical Restraint ProceduresMomoNo ratings yet
- Solutions For Improving The Accessibility of Existing Elevators To People With Limited MobilityDocument4 pagesSolutions For Improving The Accessibility of Existing Elevators To People With Limited MobilityKleemmann Hellas SANo ratings yet
- Requirements As Per Government of India Ministry of Tourism For Four Star HotelDocument10 pagesRequirements As Per Government of India Ministry of Tourism For Four Star HotelRoyal JadhavNo ratings yet
- Ambulift - Low Cabin - Specs - V2Document5 pagesAmbulift - Low Cabin - Specs - V2gueusquinNo ratings yet
- Stretchy Wchair ReportDocument17 pagesStretchy Wchair ReportBoopathi KalaiNo ratings yet
- Interior ErgonomicsDocument8 pagesInterior Ergonomicsv_anand78No ratings yet
- (ERGONOMIC) Circulation Space in OfficesDocument13 pages(ERGONOMIC) Circulation Space in OfficesSANJU RANINo ratings yet
- Katalog 2019 - EN - v1 - Web PDFDocument120 pagesKatalog 2019 - EN - v1 - Web PDFpaulhau2002No ratings yet