Download as pdf or txt
You might also like
- Nike Inc Executive SummaryDocument83 pagesNike Inc Executive Summarycorporatestrategy79% (14)
- SMT Generic Control PlanDocument3 pagesSMT Generic Control Plantuan mai vanNo ratings yet
- Marketing Project Topics and MaterialsDocument3 pagesMarketing Project Topics and MaterialsAlo Peter taiwoNo ratings yet
- 03 - Project For QCI AwardDocument43 pages03 - Project For QCI AwardAsawari JoshiNo ratings yet
- Dairy Farming Business Plan 19Document22 pagesDairy Farming Business Plan 19Josephine Chirwa100% (5)
- HA CEDAC Workshop INDO Kaizen PartDocument16 pagesHA CEDAC Workshop INDO Kaizen PartHardi BanuareaNo ratings yet
- Project Integration Management: Process GroupsDocument1 pageProject Integration Management: Process GroupsMallikarjuna RaoNo ratings yet
- DMAIC Process IllustrationDocument14 pagesDMAIC Process Illustrationsqaiba_gNo ratings yet
- Apqp ProblemsDocument1 pageApqp Problemskaran singhNo ratings yet
- Measurement System AnalysisDocument2 pagesMeasurement System AnalysispsathishthevanNo ratings yet
- Continuous Improvement Toolkit: Waste AnalysisDocument53 pagesContinuous Improvement Toolkit: Waste Analysisakdmech9621No ratings yet
- Final Report TPM PartDocument16 pagesFinal Report TPM PartNikita AwasthiNo ratings yet
- Statistical Process ControlDocument57 pagesStatistical Process ControlSandeep PasumarthiNo ratings yet
- MeasureDocument51 pagesMeasureAshwani KumarNo ratings yet
- 02W2-3 - Ch02 - Facilities Planning - Product, Process and Schedule DesignDocument45 pages02W2-3 - Ch02 - Facilities Planning - Product, Process and Schedule DesignQuynh Chau TranNo ratings yet
- VE Presentation July 15, 2019Document78 pagesVE Presentation July 15, 2019Danao ErickNo ratings yet
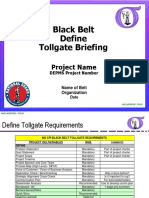
- Module 14. Define TollgateDocument17 pagesModule 14. Define Tollgatetaghavi1347No ratings yet
- Part1 Define - GBDocument38 pagesPart1 Define - GBNitesh GoyalNo ratings yet
- Impact of Defects-Measuring Defect LevelsDocument16 pagesImpact of Defects-Measuring Defect LevelsDiego FloresNo ratings yet
- Lean and Kanban-Based: Software DevelopmentDocument42 pagesLean and Kanban-Based: Software Developmentanafc1403No ratings yet
- Module 51. Improve TollgateDocument45 pagesModule 51. Improve Tollgatetaghavi1347No ratings yet
- M D A I C: Measure Define Improve ControlDocument1 pageM D A I C: Measure Define Improve ControlhhhhhhhhNo ratings yet
- The 5 Core ToolDocument17 pagesThe 5 Core ToolRajesh GhoshNo ratings yet
- Lean Manufacturing 1Document70 pagesLean Manufacturing 1AbhiNo ratings yet
- WCM Roi PDFDocument20 pagesWCM Roi PDFjackpedro_surf2No ratings yet
- Process Manager WorkshopDocument58 pagesProcess Manager WorkshopHamada AhmedNo ratings yet
- Kaizen EventsDocument35 pagesKaizen EventsIndhu SharmaKSNo ratings yet
- Chap 2Document28 pagesChap 2Keyredin SelmanNo ratings yet
- Dell Server Ordering Six Sigma Case StudyDocument2 pagesDell Server Ordering Six Sigma Case StudySteven BonacorsiNo ratings yet
- 4.chapter 2 Project Management ProcessesDocument9 pages4.chapter 2 Project Management ProcessesHlogi MalatjiNo ratings yet
- Dead Endclamp Failure AnalysisDocument26 pagesDead Endclamp Failure AnalysisRK KumarNo ratings yet
- Lennox Supplier Qualification Development Guidelines English February 2014 Rev 5Document27 pagesLennox Supplier Qualification Development Guidelines English February 2014 Rev 5alexrferreiraNo ratings yet
- Standardization Basics-24 Jul 09Document11 pagesStandardization Basics-24 Jul 09Dilfaraz KalawatNo ratings yet
- Quality PLNG Control Imp, Benchmarking SDDocument95 pagesQuality PLNG Control Imp, Benchmarking SDANKIT KUMARNo ratings yet
- The Visual Workplace: Includes Excerpts From: The Visual Factory, by Michel Greif Productivity PressDocument21 pagesThe Visual Workplace: Includes Excerpts From: The Visual Factory, by Michel Greif Productivity Pressmilou88No ratings yet
- Corrective Actions Preventive ActionsDocument33 pagesCorrective Actions Preventive ActionsVidya100% (1)
- Apqp RasicDocument5 pagesApqp RasicvishalNo ratings yet
- Summer Project REPORTDocument20 pagesSummer Project REPORTMrdev25555No ratings yet
- Chrysler Customer Specifics For PPAP 4th Edition July 11Document2 pagesChrysler Customer Specifics For PPAP 4th Edition July 11JOECOOL67No ratings yet
- Quality ManualDocument132 pagesQuality ManualstacayNo ratings yet
- Test Paper 7 QC ToolsDocument3 pagesTest Paper 7 QC Toolsb-consultant960No ratings yet
- A Process Capability Study On CNC Operation by The Application of Statistical Process Control ApproachDocument14 pagesA Process Capability Study On CNC Operation by The Application of Statistical Process Control ApproachvivgukgjujgNo ratings yet
- SAQP Elements OverviewDocument38 pagesSAQP Elements OverviewBoštjan Dokl MenihNo ratings yet
- UCLA Extension Project Management 49processesDocument1 pageUCLA Extension Project Management 49processesSeveral SunNo ratings yet
- 8D's Process Worksheet: MDR/SCAR Number: Supplier: Response Due DateDocument3 pages8D's Process Worksheet: MDR/SCAR Number: Supplier: Response Due DateUlysses CarrascoNo ratings yet
- ApqpDocument11 pagesApqpChandru JattiNo ratings yet
- 3c Red Tag TemplateDocument1 page3c Red Tag TemplatehiteshcparmarNo ratings yet
- Guideline APQP Workbook Rev DDocument19 pagesGuideline APQP Workbook Rev Dmpedraza-1100% (1)
- 供应商培训资料 8D PDFDocument77 pages供应商培训资料 8D PDFFisher1987No ratings yet
- 3L and 5 Why Presentation - MKGDocument70 pages3L and 5 Why Presentation - MKGMukesh GuptaNo ratings yet
- Cellular Manufacturing Flexible OperationsDocument16 pagesCellular Manufacturing Flexible OperationsAlpha Excellence consultingNo ratings yet
- Chapter 1introduction To Six SigmaDocument39 pagesChapter 1introduction To Six SigmaKaranShindeNo ratings yet
- Apqp A StoryDocument13 pagesApqp A StoryJayantRK50% (2)
- Six Sigma For Chemical Engineers: George LiebermannDocument39 pagesSix Sigma For Chemical Engineers: George LiebermannDave CNo ratings yet
- Intro To Six SigmaDocument84 pagesIntro To Six Sigmaguriya khanNo ratings yet
- Quick Change OverDocument14 pagesQuick Change Overghaos1No ratings yet
- Poka-Yoke Team 4Document14 pagesPoka-Yoke Team 4Ratandeep PandeyNo ratings yet
- Apqp PpapDocument50 pagesApqp PpapAlpkan YılmazNo ratings yet
- Unblocking BottlenecksDocument3 pagesUnblocking BottlenecksMaggie GonzalesNo ratings yet
- A1 - Process CapabilityDocument40 pagesA1 - Process CapabilityAzer Asociados SacNo ratings yet
- Kaizen Idea Sheet: CountermeasureDocument1 pageKaizen Idea Sheet: CountermeasurerahulNo ratings yet
- Social Policy, Inequalities and The Battle of Rights in Latin AmericaDocument18 pagesSocial Policy, Inequalities and The Battle of Rights in Latin AmericaHannahNo ratings yet
- Warehouse InchargeDocument2 pagesWarehouse InchargeAmanullah AmarNo ratings yet
- 4201-232-V4-8900-08018 - 001 - Code 2Document82 pages4201-232-V4-8900-08018 - 001 - Code 2Shoaib KhanNo ratings yet
- The Advantages and Disadvantages of Strategic ManagementDocument3 pagesThe Advantages and Disadvantages of Strategic ManagementBrian KerrNo ratings yet
- TATA Motors - Starbuses Strategic Analysis - MBA Summer Training Project Report PDF DownloadDocument73 pagesTATA Motors - Starbuses Strategic Analysis - MBA Summer Training Project Report PDF DownloadZAFAR AHSAN ADILNo ratings yet
- 005 - 1965 - Law Relating To TaxationDocument15 pages005 - 1965 - Law Relating To TaxationSubhayan BoralNo ratings yet
- Updated Arrears Estimator Clerical StaffDocument8 pagesUpdated Arrears Estimator Clerical Staffkmuraleedharan09No ratings yet
- G11 - Acctng1 - Problem JournalsDocument10 pagesG11 - Acctng1 - Problem JournalsKaye VillaflorNo ratings yet
- Marketing Strategy of Hyundai MotorsDocument142 pagesMarketing Strategy of Hyundai MotorsSourabh SoniNo ratings yet
- Influential Factors in Rising Needs of Mobile BankingDocument5 pagesInfluential Factors in Rising Needs of Mobile BankingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- "Inventory Management of ": A Project Report OnDocument29 pages"Inventory Management of ": A Project Report OnJasleen AbbottNo ratings yet
- Day Trading PEG Red To Green SetupsDocument5 pagesDay Trading PEG Red To Green Setupsarenaman0528No ratings yet
- Chapter 6 LearningDocument28 pagesChapter 6 Learningفيصل ابراهيمNo ratings yet
- Inspection Release Note: Purchase Order DetailsDocument1 pageInspection Release Note: Purchase Order DetailsLauraNo ratings yet
- Global StrategyDocument14 pagesGlobal StrategyAhsan SheikhNo ratings yet
- AVATAR Portfolio BriefDocument3 pagesAVATAR Portfolio BriefTK chengNo ratings yet
- Marketing Department of BritanniaDocument6 pagesMarketing Department of BritanniaradhikaNo ratings yet
- Pooja 2023 CVDocument6 pagesPooja 2023 CVVipinNo ratings yet
- kinh tế vi môDocument13 pageskinh tế vi môÁnh Nguyễn ThịNo ratings yet
- Macroeconomics 20th Edition Mcconnell Test Bank Full Chapter PDFDocument41 pagesMacroeconomics 20th Edition Mcconnell Test Bank Full Chapter PDFdeanwheeler24031987dtp100% (12)
- BEC Vantage PG 8Document1 pageBEC Vantage PG 8juanNo ratings yet
- Impact of Advertisement On Children Behaviour - Sanjukta BanerjeeDocument57 pagesImpact of Advertisement On Children Behaviour - Sanjukta BanerjeeSanjukta BanerjeeNo ratings yet
- Ibm Gatt and WtoDocument14 pagesIbm Gatt and Wto6038 Mugilan kNo ratings yet
- Ric Profit Rates 17-06-2021Document4 pagesRic Profit Rates 17-06-2021Mobashir Mehmood KhanNo ratings yet
- Class Notes IA Marks Guidelines First Grade CollegeDocument52 pagesClass Notes IA Marks Guidelines First Grade CollegeyallappaNo ratings yet
- Kotex Maxi Pads Night With Wings (Pack of 8s X 10) 80 Sanitary Pads - Buy Online at Best Price in UAE - Amazon - AeDocument4 pagesKotex Maxi Pads Night With Wings (Pack of 8s X 10) 80 Sanitary Pads - Buy Online at Best Price in UAE - Amazon - AemuhammadNo ratings yet