Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anesthesia Policy and Procedure Manual - SampleDocument5 pagesAnesthesia Policy and Procedure Manual - SampleSamathaSAM100% (1)
- Dark Heresy Character Sheet 5 PageDocument5 pagesDark Heresy Character Sheet 5 PagePreacher8794No ratings yet
- Work Stress As A Risk Factor For Cardiovascular DiseaseDocument9 pagesWork Stress As A Risk Factor For Cardiovascular DiseaseVictor abramonteNo ratings yet
- Systematic Reviews and Meta-And Pooled AnalysesDocument11 pagesSystematic Reviews and Meta-And Pooled AnalysesVictor abramonteNo ratings yet
- Postulantes UNSM T 2015 IDocument31 pagesPostulantes UNSM T 2015 IVictor abramonteNo ratings yet
- Tumores Desmoides: Cuadro Clínico y SobrevidaDocument8 pagesTumores Desmoides: Cuadro Clínico y SobrevidaVictor abramonteNo ratings yet
- United States v. Rodney Thompson, 4th Cir. (1999)Document6 pagesUnited States v. Rodney Thompson, 4th Cir. (1999)Scribd Government DocsNo ratings yet
- TEAL Center Fact Sheet No. 8: Effective Lesson Planning: Access Resources For State Adult Education StaffDocument6 pagesTEAL Center Fact Sheet No. 8: Effective Lesson Planning: Access Resources For State Adult Education StaffKimberly Jamili MiayoNo ratings yet
- Insurance Reviewer Notes by Atty. SaclutiDocument12 pagesInsurance Reviewer Notes by Atty. SaclutiGayFleur Cabatit RamosNo ratings yet
- Analysis of Sabrimala ControversyDocument29 pagesAnalysis of Sabrimala ControversyShambhavi PathakNo ratings yet
- Words and Their Characteristics Word Classes: Horse-SDocument2 pagesWords and Their Characteristics Word Classes: Horse-SsammiedearbornNo ratings yet
- Analysis of Variance: Testing Equality of Means Across GroupsDocument7 pagesAnalysis of Variance: Testing Equality of Means Across GroupsMuraliManoharNo ratings yet
- The Jaya MahabharataDocument4 pagesThe Jaya Mahabharataannakumar2678No ratings yet
- Semillas Ecologia de La Regeneracion en Plantas PDFDocument423 pagesSemillas Ecologia de La Regeneracion en Plantas PDFjuanchotirador100% (1)
- Cash and Marketable SecuritiesDocument8 pagesCash and Marketable SecuritieserikaNo ratings yet
- Pozlaćena Fibula SirmiumDocument12 pagesPozlaćena Fibula SirmiumPero68No ratings yet
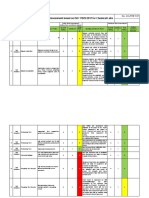
- Lab Risk Assessment Based On ISO 17025:2017 For Chemical LabsDocument5 pagesLab Risk Assessment Based On ISO 17025:2017 For Chemical Labsgristy100% (1)
- Welfare Policies of Dawar FootwearDocument110 pagesWelfare Policies of Dawar FootwearRohit Soni33% (3)
- Epilepsy SurgeryDocument13 pagesEpilepsy SurgeryDon RomanNo ratings yet
- Chap 007Document18 pagesChap 007Ahmed A HakimNo ratings yet
- Evaluating Algebraic Expressions Worksheet PDFDocument2 pagesEvaluating Algebraic Expressions Worksheet PDFLilly0% (1)
- NRF52 Online Power ProfilerDocument6 pagesNRF52 Online Power Profilerzhongkai chengNo ratings yet
- I Will Follow You IntoDocument156 pagesI Will Follow You Intoisis perezNo ratings yet
- Related To Limited Financial ResourcesDocument2 pagesRelated To Limited Financial ResourcesDan HizonNo ratings yet
- Managing Occupational Health and Safety in The Mining IndustryDocument12 pagesManaging Occupational Health and Safety in The Mining IndustryalexNo ratings yet
- Chapter 17 - Special RelativityDocument37 pagesChapter 17 - Special Relativityascd_msvuNo ratings yet
- Improving Access To Medicines For Non-Communicable Diseases in Rural India: A Mixed Methods Study Protocol Using Quasi-Experimental DesignDocument19 pagesImproving Access To Medicines For Non-Communicable Diseases in Rural India: A Mixed Methods Study Protocol Using Quasi-Experimental DesignNino AlicNo ratings yet
- Examen - Week 10 - Task - Bill's Daily RoutineDocument3 pagesExamen - Week 10 - Task - Bill's Daily RoutineEstrella Facundo VilchezNo ratings yet
- 2018 CAS Path To SuccessDocument1 page2018 CAS Path To SuccesskidNo ratings yet
- Accenture Placement Paper 1) Aptitude Test:: WWW - Edugeeks.inDocument9 pagesAccenture Placement Paper 1) Aptitude Test:: WWW - Edugeeks.inSourabh KvlNo ratings yet
- Uv VisibleDocument20 pagesUv VisibleahmedNo ratings yet
- ReferencesDocument4 pagesReferencesMahmud Abdullahi SarkiNo ratings yet
- Cir Vs WyethDocument1 pageCir Vs WyethHollyhock Mmgrzhfm100% (1)
- (MATUTE, RODEL) Module-3-LESSON-1-SPEAR-3-TAKYANDocument4 pages(MATUTE, RODEL) Module-3-LESSON-1-SPEAR-3-TAKYANRodel MatuteNo ratings yet