Download as pdf or txt
You might also like
- Modern BeggDocument18 pagesModern BeggRishika EkNo ratings yet
- Basic Edgewise TechniqueDocument109 pagesBasic Edgewise TechniqueRajshekhar Banerjee100% (1)
- Rodney Vs Death Rabies RadioLab Homework Assignment VMCDocument5 pagesRodney Vs Death Rabies RadioLab Homework Assignment VMCRonalda GuevarraNo ratings yet
- cs2 NCPDocument1 pagecs2 NCPapi-251084195No ratings yet
- Administration of Medication Through Nasogastric TubeDocument10 pagesAdministration of Medication Through Nasogastric TubeBlinkeen Woods100% (1)
- PMDC Index Pakistan of Recognized JournalsDocument3 pagesPMDC Index Pakistan of Recognized JournalsAhmed MateenNo ratings yet
- SHSB Health Contact DetailsDocument35 pagesSHSB Health Contact DetailsDharmendra Saw100% (2)
- MBT 2Document135 pagesMBT 2anandkadintiNo ratings yet
- T Loop Mechanics For Effective Space Closure in Bimaxillary Dentoalveolar Protrusion - A Case ReportDocument5 pagesT Loop Mechanics For Effective Space Closure in Bimaxillary Dentoalveolar Protrusion - A Case ReportVishal VijNo ratings yet
- UNIT-II - (Part-5) CIRCULAR SLABSDocument32 pagesUNIT-II - (Part-5) CIRCULAR SLABSDuraid FalihNo ratings yet
- JCDR 10 ZD04Document3 pagesJCDR 10 ZD04MAYRA ALEJANDRA BAHAMON TRUJILLONo ratings yet
- ISSN 2347-5579: 0.018" Versus 0.022" Bracket Slot Systems in Orthodontics: A ReviewDocument4 pagesISSN 2347-5579: 0.018" Versus 0.022" Bracket Slot Systems in Orthodontics: A ReviewRahulLife's100% (1)
- Ijodr 2 (1) 32-33Document2 pagesIjodr 2 (1) 32-33ALBERTO JESUS PACHECO DIAZNo ratings yet
- FinishingDocument76 pagesFinishingsahar emadNo ratings yet
- Art 2022 DistalizacionDocument11 pagesArt 2022 DistalizacionrioscasosclinicosNo ratings yet
- Principles and Technique: Antonino G. Secchi, DMD, MSDocument22 pagesPrinciples and Technique: Antonino G. Secchi, DMD, MSCatia Sofia A PNo ratings yet
- MBT IDocument125 pagesMBT INeelima ChandranNo ratings yet
- WP RonconeDocument10 pagesWP RonconeAhmad EgbariaNo ratings yet
- 0.18 Vs O.022Document18 pages0.18 Vs O.022DrParmod Tayal100% (3)
- Teknik Operasi Fraktur MandibulaDocument18 pagesTeknik Operasi Fraktur MandibulaGun Gun GunawanNo ratings yet
- CCO System - Introduction 2Document128 pagesCCO System - Introduction 2Adriana FalconNo ratings yet
- A New Lingual Straight-Wire TechniqueDocument10 pagesA New Lingual Straight-Wire TechniquedesantosalbaNo ratings yet
- The Seismic Design and Performance of Reinforced Concrete Beam-Column Knee JointsDocument8 pagesThe Seismic Design and Performance of Reinforced Concrete Beam-Column Knee JointsMarimuthu KaliyamoorthyNo ratings yet
- Canal Preparation and Obturation: An Updated View of The Two Pillars of Nonsurgical EndodonticsDocument8 pagesCanal Preparation and Obturation: An Updated View of The Two Pillars of Nonsurgical EndodonticsMaryam MandsaurwalaNo ratings yet
- PIIS0889540610007730Document1 pagePIIS0889540610007730Aly OsmanNo ratings yet
- 6.0 Column: VerticallyDocument27 pages6.0 Column: VerticallyWah KhaingNo ratings yet
- Refinements in Beggs TechniqueDocument136 pagesRefinements in Beggs TechniqueGokul SivaNo ratings yet
- Base Plate Dan Bite RimDocument13 pagesBase Plate Dan Bite Rimmuhammad100% (1)
- Catalog Slim LineDocument16 pagesCatalog Slim LineAlina SecrețeanuNo ratings yet
- TranslateDocument3 pagesTranslatenurulhidayahfkgNo ratings yet
- BMD Lab Manual Yr 2023-24Document19 pagesBMD Lab Manual Yr 2023-24HarshilNo ratings yet
- Brackets 2Document14 pagesBrackets 2Cristian DavilaNo ratings yet
- Resto To SeriesDocument14 pagesResto To SeriesSondosNo ratings yet
- 7Document6 pages7Sungo GridsawanNo ratings yet
- 10 Review JaiswalDocument7 pages10 Review JaiswalAniket PotnisNo ratings yet
- Cast Metal Restorations 2021Document56 pagesCast Metal Restorations 2021nandani kumariNo ratings yet
- Orthodontic BracketsDocument9 pagesOrthodontic Bracketsdevi kanthNo ratings yet
- Finishing Stage Part 2Document132 pagesFinishing Stage Part 2sahar emadNo ratings yet
- Torque Expression Capacity of 0.018 and 0.022 Bracket Slots by Changing Archwire Material and Cross SectionDocument18 pagesTorque Expression Capacity of 0.018 and 0.022 Bracket Slots by Changing Archwire Material and Cross SectionRebin AliNo ratings yet
- Keles Slider Book ChapterDocument12 pagesKeles Slider Book ChapterLiliana Aguilar VillarrealNo ratings yet
- OSL CatalougeDocument28 pagesOSL CatalougeVishalSharmaNo ratings yet
- SJ Mepla Brief IntroductionDocument13 pagesSJ Mepla Brief IntroductiondynamicsbookNo ratings yet
- Brackets IN ORTHODONTICSDocument122 pagesBrackets IN ORTHODONTICSMohammed Hussain80% (5)
- SpringsDocument7 pagesSpringsshihap2020738650988No ratings yet
- Self - Use of Sma and Buckling Restrained Braces To Reduce Seismic Residual Deformations in Low-Rise RC FramesDocument11 pagesSelf - Use of Sma and Buckling Restrained Braces To Reduce Seismic Residual Deformations in Low-Rise RC FramesludwingNo ratings yet
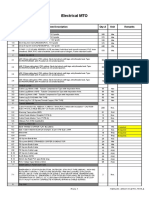
- Electrical MTO: Sr. No. Item Description Qty-A Unit RemarksDocument2 pagesElectrical MTO: Sr. No. Item Description Qty-A Unit RemarksadilsiddiqueNo ratings yet
- Pro Tape Run I HintsDocument20 pagesPro Tape Run I HintsIvasuc AlexandruNo ratings yet
- Insturments Used in EndodonticsDocument22 pagesInsturments Used in EndodonticsIna BogdanNo ratings yet
- Orthodontia Notes by Dr. RounikDocument22 pagesOrthodontia Notes by Dr. RounikRounik TalukdarNo ratings yet
- Z.4-Frictional-forces AJO Feb-2008 KimDocument10 pagesZ.4-Frictional-forces AJO Feb-2008 KimSprix ZenNo ratings yet
- CBCT Imaging To Diagnose and Correct The Failure Ofmaxillary Arch Retraction With IZC Screw Anchorage PDFDocument14 pagesCBCT Imaging To Diagnose and Correct The Failure Ofmaxillary Arch Retraction With IZC Screw Anchorage PDFSoe San KyawNo ratings yet
- BPT Part IIDocument99 pagesBPT Part IISaumya SinghNo ratings yet
- Flexural Properties of Rectangular Nickel-Titanium Orthodontic Wires When Used As Ribbon ArchwiresDocument10 pagesFlexural Properties of Rectangular Nickel-Titanium Orthodontic Wires When Used As Ribbon ArchwiresjamesNo ratings yet
- Bioprogressive TherapyDocument4 pagesBioprogressive TherapyKemo HusseinNo ratings yet
- Space Closure by AlmuzianDocument16 pagesSpace Closure by AlmuzianNizam MuhamadNo ratings yet
- New Design Space Regainers JCDocument43 pagesNew Design Space Regainers JCsnehasthaNo ratings yet
- LED Infinity Cube End TableDocument23 pagesLED Infinity Cube End TableEldglay da Silva DomingosNo ratings yet
- Frictionless MichanicsDocument57 pagesFrictionless MichanicsdrshreyabagrawalNo ratings yet
- NO. Sub Bagian 1 Laring-Faring: Usulan Kebutuhan Implant KSM THT-KL 2021Document6 pagesNO. Sub Bagian 1 Laring-Faring: Usulan Kebutuhan Implant KSM THT-KL 2021rahmihaolonganNo ratings yet
- Biomat 2Document24 pagesBiomat 2Habib AbdurrahmanNo ratings yet
- Flex MasterDocument9 pagesFlex MastervanillalavenderNo ratings yet
- Literature Feeding and Eating Quick GuideDocument17 pagesLiterature Feeding and Eating Quick GuideHana alassafNo ratings yet
- 3 Chronic MyringitisDocument19 pages3 Chronic MyringitissyahputriNo ratings yet
- Guidelines On Aesthetic Medical Practice For Registered Medical PractitionersDocument47 pagesGuidelines On Aesthetic Medical Practice For Registered Medical Practitionerszahisma8950% (2)
- Brosur AtenololDocument1 pageBrosur AtenololEva RiskiNo ratings yet
- Observacion y Practica de AferesisDocument296 pagesObservacion y Practica de AferesisWilmer Cruzado CarrascoNo ratings yet
- Pain Management NCLEXDocument5 pagesPain Management NCLEXPotchiee PfizerNo ratings yet
- AQA GCSE Science Biology Keeping HealthyDocument30 pagesAQA GCSE Science Biology Keeping HealthySteve BishopNo ratings yet
- 77.18 Shen Guan and Three Emperors - Master Kidney PointDocument3 pages77.18 Shen Guan and Three Emperors - Master Kidney Pointalbar ismuNo ratings yet
- Recommended Reading MeterialsDocument160 pagesRecommended Reading MeterialsdilNo ratings yet
- Midwifery Pharmacology-32Document1 pageMidwifery Pharmacology-32georgeloto12No ratings yet
- Case Study For PneumothoraxDocument4 pagesCase Study For PneumothoraxGabbii CincoNo ratings yet
- Perevod Behzod Nodira PDFDocument327 pagesPerevod Behzod Nodira PDFMayur WakchaureNo ratings yet
- ICU AlgorithmsDocument45 pagesICU AlgorithmsHashimIdreesNo ratings yet
- RNA VirusesDocument404 pagesRNA VirusesSisayNo ratings yet
- 1 PBDocument7 pages1 PBmanusia relaNo ratings yet
- Basalimplants 3 130724225029 Phpapp02Document26 pagesBasalimplants 3 130724225029 Phpapp02joephinNo ratings yet
- Health Flow ChartDocument1 pageHealth Flow ChartAlex Cainoy JrNo ratings yet
- Treatment of MalariaDocument56 pagesTreatment of MalariaBung FauziNo ratings yet
- Style Guide - NCDJDocument11 pagesStyle Guide - NCDJVaishnavi JayakumarNo ratings yet
- Afp 20140501 P 731Document8 pagesAfp 20140501 P 731metabolismeproteinNo ratings yet
- MHS 6401Document5 pagesMHS 6401Delelegn EmwodewNo ratings yet
- Nonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewDocument9 pagesNonadherence To Medications Among Persons With Bipolar Affective Disorder - A ReviewIra DomunNo ratings yet
- Medi Test Urine Analysis ENDocument12 pagesMedi Test Urine Analysis ENCandy ManNo ratings yet
- Maternal and Early-Life Nutrition and HealthDocument4 pagesMaternal and Early-Life Nutrition and HealthTiffani_Vanessa01No ratings yet
- HematocritDocument3 pagesHematocritMaybelle Acap PatnubayNo ratings yet