Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Dance and Instrumental DifferDocument470 pagesDance and Instrumental Differaysun100% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Manual I5006.zf - en PDFDocument140 pagesManual I5006.zf - en PDFBaşarŞenNo ratings yet
- Turnip28 V16a Core RulesDocument73 pagesTurnip28 V16a Core RulesСлавік БачинськийNo ratings yet
- CDR-EL-1109 - CDR Sample ElectricalDocument1 pageCDR-EL-1109 - CDR Sample ElectricalCDR Download100% (1)
- Computer POST and Beep CodesDocument8 pagesComputer POST and Beep CodesJDNo ratings yet
- Kinsella Japanese Subculture in The 1990s PDFDocument29 pagesKinsella Japanese Subculture in The 1990s PDFmadadudeNo ratings yet
- HLARA ProcessDocument5 pagesHLARA ProcessRanjana SainiNo ratings yet
- Elln Matrix: Valenzuela South District Ilang-Ilang St. Karuhatan, Valenzuela City Tel/fax No. 2944246Document1 pageElln Matrix: Valenzuela South District Ilang-Ilang St. Karuhatan, Valenzuela City Tel/fax No. 2944246rafaela villanuevaNo ratings yet
- ReadmeDocument6 pagesReadmegabyorNo ratings yet
- CDP Proposal KavarattiDocument11 pagesCDP Proposal KavarattiShivansh Singh GautamNo ratings yet
- Pembumian 110705103913 Phpapp02Document33 pagesPembumian 110705103913 Phpapp02Noor Syazwani Md SharifNo ratings yet
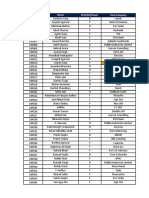
- Roll No. Name PPO/PPI/Finals Final CompanyDocument48 pagesRoll No. Name PPO/PPI/Finals Final CompanyYash AgarwalNo ratings yet
- PM1115UW Setup GuideDocument13 pagesPM1115UW Setup GuideFrancisco Baeza JiménezNo ratings yet
- When Waves Enter Shallow Water, They Slow Down and Their Amplitude (Height) IncreasesDocument2 pagesWhen Waves Enter Shallow Water, They Slow Down and Their Amplitude (Height) IncreasesPei LingNo ratings yet
- Blockchain Spec PDFDocument18 pagesBlockchain Spec PDFblueNo ratings yet
- ArtsDocument71 pagesArtsits.me.brader07No ratings yet
- Political Activism in Nursing Final PresentationDocument30 pagesPolitical Activism in Nursing Final PresentationDip Ayan MNo ratings yet
- Edcd797 001 Spring 2015 Eating Disorders SyllabusDocument9 pagesEdcd797 001 Spring 2015 Eating Disorders Syllabusapi-329795302No ratings yet
- Our Lady of Guadalupe Minor Seminary Junior High School: Curriculum Map in Information and Communication TechnologyDocument7 pagesOur Lady of Guadalupe Minor Seminary Junior High School: Curriculum Map in Information and Communication Technologyreycelyn corsinoNo ratings yet
- Roles and Characteristics of Problem Solving in The Mathematics Curriculum: A ReviewDocument19 pagesRoles and Characteristics of Problem Solving in The Mathematics Curriculum: A ReviewSarahNo ratings yet
- CC103 Engineering Surveying 1 Chapter 2Document15 pagesCC103 Engineering Surveying 1 Chapter 2Xendra AqeylaaNo ratings yet
- Earth As A SphereDocument96 pagesEarth As A SphereMarlina MohamedNo ratings yet
- Work in Team Environment Learning ModuleDocument3 pagesWork in Team Environment Learning ModuleNesri YayaNo ratings yet
- Huawei Transmission Configuring The Built-In WDM ServiceDocument5 pagesHuawei Transmission Configuring The Built-In WDM ServiceElizabeth RichNo ratings yet
- Retune For Live v1.4 READMEDocument5 pagesRetune For Live v1.4 README항가No ratings yet
- MGMT100S2 2019 - With Lecture Schedule PDFDocument8 pagesMGMT100S2 2019 - With Lecture Schedule PDFAkshayScamlattiNo ratings yet
- TalentTrees v1 PDFDocument22 pagesTalentTrees v1 PDFpaulopt21100% (1)
- 3 Object Oriented Modeling and DesignDocument9 pages3 Object Oriented Modeling and DesignMaya M SNo ratings yet
- The EMA Tasks: Ema: Is Intel'S Business Model Fit For The Future?Document3 pagesThe EMA Tasks: Ema: Is Intel'S Business Model Fit For The Future?saherhcc4686No ratings yet
- Voice Controlled Wheelchair: Project ReportDocument52 pagesVoice Controlled Wheelchair: Project Reportmughees sarwar awanNo ratings yet