
Karnataka, Bangalore
Karnataka, Bangalore
You might also like
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- Name of The Candidate and AddressDocument16 pagesName of The Candidate and AddressYash RamawatNo ratings yet
- PHD Thesis: University of Medicine and Pharmacy CraiovaDocument10 pagesPHD Thesis: University of Medicine and Pharmacy CraiovapaulNo ratings yet
- Synopsis Proforma For Registration of Subject For DissertationDocument18 pagesSynopsis Proforma For Registration of Subject For DissertationKenneth Myro GarciaNo ratings yet
- Dysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Document7 pagesDysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Jihan FaadhilahNo ratings yet
- 05 N501 28766Document23 pages05 N501 28766Rumela Ganguly ChakrabortyNo ratings yet
- Study of Metabolic Syndrome and Diabetes Mellitus Among Ischemic Stroke Patients in A Tertiary Hospital, Northern KarnatakaDocument7 pagesStudy of Metabolic Syndrome and Diabetes Mellitus Among Ischemic Stroke Patients in A Tertiary Hospital, Northern KarnatakaIJAR JOURNALNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutnidaNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutmaydamayNo ratings yet
- Final Synopsis Format Sample ACNDocument25 pagesFinal Synopsis Format Sample ACNAbhijit DasNo ratings yet
- 17 Analysis of Maternal Outcome of General Versus Spinal Anaesthesia For Caesarean Delivery in Severe Pre EclampsiaDocument7 pages17 Analysis of Maternal Outcome of General Versus Spinal Anaesthesia For Caesarean Delivery in Severe Pre EclampsiaUlfa PuspitaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument14 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaAnna StimNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleUmar MukhtarNo ratings yet
- Seminar: Amy S Jordan, David G Mcsharry, Atul MalhotraDocument12 pagesSeminar: Amy S Jordan, David G Mcsharry, Atul MalhotraSerkan KüçüktürkNo ratings yet
- Jurnal Jantung 1Document7 pagesJurnal Jantung 1Egga Mariana YudaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaYadnya SaputraNo ratings yet
- Nutrients: The Use of Enteral Nutrition in The Management of StrokeDocument6 pagesNutrients: The Use of Enteral Nutrition in The Management of StrokeMita SeptoryNo ratings yet
- Nutrients: The Use of Enteral Nutrition in The Management of StrokeDocument6 pagesNutrients: The Use of Enteral Nutrition in The Management of StrokeMiranda MetriaNo ratings yet
- Evaluación de TosDocument8 pagesEvaluación de TosCarolina CelisNo ratings yet
- Journal Pre-Proof: Clinical NutritionDocument19 pagesJournal Pre-Proof: Clinical NutritionThay SousaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument19 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaARJUN BNo ratings yet
- Swallow Respiratory Patterns and Aging Presbyphagia or DysphagiaDocument5 pagesSwallow Respiratory Patterns and Aging Presbyphagia or Dysphagiaariyanti rezekiNo ratings yet
- 05 N111 39956Document28 pages05 N111 39956Mahruri SaputraNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Prevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionDocument10 pagesPrevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionZaskia PutriNo ratings yet
- Refeeding Syndrome A Literature Review KhanDocument7 pagesRefeeding Syndrome A Literature Review Khangw060qpy100% (1)
- Psychological Aspects in Chronic Renal Failure: Review RticleDocument10 pagesPsychological Aspects in Chronic Renal Failure: Review RticleTry Febriani SiregarNo ratings yet
- Dysphagia Pada GeriatriDocument12 pagesDysphagia Pada Geriatrialfi syahrinNo ratings yet
- Summary ReportDocument27 pagesSummary ReportShweta GrigsonNo ratings yet
- "A Comparative Study To Assess Knowledge and Practice On Cardio Pulmonary Resuscitation Among Icu/Ccu NursesDocument21 pages"A Comparative Study To Assess Knowledge and Practice On Cardio Pulmonary Resuscitation Among Icu/Ccu NursesPushpa ChhillarNo ratings yet
- Final Pud CaseDocument155 pagesFinal Pud CaseLevy Garcia SanchezNo ratings yet
- 261-Article Text-435-1-10-20230103Document12 pages261-Article Text-435-1-10-20230103Vince Daniel VillalbaNo ratings yet
- 1 s2.0 S0753332220309148 MainDocument7 pages1 s2.0 S0753332220309148 Mainyayu latifahNo ratings yet
- Dysphagia in Older AdultsDocument10 pagesDysphagia in Older Adultsconstanza duran cordovaNo ratings yet
- Advances in Gerd: Management of Dysphagia in Stroke PatientsDocument3 pagesAdvances in Gerd: Management of Dysphagia in Stroke PatientsFeliciaNo ratings yet
- A Severe Asphyxiated Newborn: A Case ReportDocument13 pagesA Severe Asphyxiated Newborn: A Case ReportEeeeeeeeeNo ratings yet
- Case Presentation of Group 1Document45 pagesCase Presentation of Group 1Kirk Clarence FloresNo ratings yet
- 1625-Article Text-4407-1-10-20230707Document14 pages1625-Article Text-4407-1-10-20230707dewa putra yasaNo ratings yet
- Diana College of Nursing, No.68, Chokkanahalli, Jakkur Post, Bangalore-64Document28 pagesDiana College of Nursing, No.68, Chokkanahalli, Jakkur Post, Bangalore-64AnggraAnzhaniNo ratings yet
- Alvarez-Larruy2022 Article SpontaneousSwallowingFrequencyDocument11 pagesAlvarez-Larruy2022 Article SpontaneousSwallowingFrequencyYarisa Villar BonilloNo ratings yet
- Synopsis PallaviDocument31 pagesSynopsis PallaviSanjeet DuhanNo ratings yet
- Group 6 1Document48 pagesGroup 6 1baldosangelique14No ratings yet
- DiverticularDiseaseoftheColon PDFDocument12 pagesDiverticularDiseaseoftheColon PDFAdrian MucileanuNo ratings yet
- SarcopeniaDocument10 pagesSarcopeniaShuaib AhmadNo ratings yet
- Evaluacion Disfagia Esofagica Adulto MayorDocument24 pagesEvaluacion Disfagia Esofagica Adulto MayorPaulina Culebro EspinozaNo ratings yet
- Advpub JE20150123Document7 pagesAdvpub JE20150123Sherly KristiNo ratings yet
- The Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaDocument9 pagesThe Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaIJRASETPublicationsNo ratings yet
- Selección de Resúmenes de Menopausia Semana Del 30 de Julio Al 5 de Agosto de 2014Document3 pagesSelección de Resúmenes de Menopausia Semana Del 30 de Julio Al 5 de Agosto de 2014rocksurNo ratings yet
- GLX 041Document7 pagesGLX 041Tatta CamposNo ratings yet
- StudyDocument23 pagesStudyJose Paul RaderNo ratings yet
- Health Outcomes of Sarcopenia A Systematic ReviewDocument16 pagesHealth Outcomes of Sarcopenia A Systematic Reviewmanuel VenegasNo ratings yet
- MD Pulmonary Medicine Thesis TopicsDocument5 pagesMD Pulmonary Medicine Thesis Topicsamandareedsalem100% (2)
- Prevention of StrokeDocument10 pagesPrevention of StrokeRasvan Cristian StoicaNo ratings yet
- Nutrient Intake and Its Association With Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults A Population-Based StudyDocument11 pagesNutrient Intake and Its Association With Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults A Population-Based StudyJetri HansNo ratings yet
- Impact of The Systematic Use of The Gugging Swallowing Screen inDocument15 pagesImpact of The Systematic Use of The Gugging Swallowing Screen inalexandraNo ratings yet
- Dr. MD Rezaul Karim Thesis Prevalance of Micro and Macrovascular Complications in Newly DetecDocument22 pagesDr. MD Rezaul Karim Thesis Prevalance of Micro and Macrovascular Complications in Newly Detecrezalata38100% (1)
- Selección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014Document5 pagesSelección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014rocksurNo ratings yet
- Ehf2 8 625Document9 pagesEhf2 8 625elza pratiwiNo ratings yet
- Perioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceDocument10 pagesPerioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceBRENDA VANESSA TREVIZO ESTRADANo ratings yet
- J.S.S College of Nursing 1 Main Saraswathipuram, MysoreDocument18 pagesJ.S.S College of Nursing 1 Main Saraswathipuram, MysoreNurul HafizaNo ratings yet
- Letter Seeking Experts For Content Validity of ToolDocument1 pageLetter Seeking Experts For Content Validity of ToolpriyagerardNo ratings yet
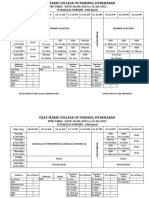
- Time Table-I - IV Year B.SC 2023Document36 pagesTime Table-I - IV Year B.SC 2023priyagerardNo ratings yet
- Adoption 150109001206 Conversion Gate01Document44 pagesAdoption 150109001206 Conversion Gate01priyagerardNo ratings yet
- College Report 2015Document120 pagesCollege Report 2015priyagerardNo ratings yet
- GNM Vol I Community Health Nursing Part 2 MinDocument446 pagesGNM Vol I Community Health Nursing Part 2 MinpriyagerardNo ratings yet
- BLINDNESSDocument24 pagesBLINDNESSpriyagerardNo ratings yet
- 4304 - M.Sc. - Community - Health - Nursing ImportantDocument84 pages4304 - M.Sc. - Community - Health - Nursing ImportantpriyagerardNo ratings yet
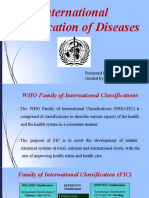
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- AMOEBIASISDocument31 pagesAMOEBIASISpriyagerard100% (1)
- 0 EndocrinedisordersseminarDocument52 pages0 EndocrinedisordersseminarpriyagerardNo ratings yet
- Nursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)Document35 pagesNursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)priyagerardNo ratings yet
- 2020 IA 3rd YearDocument7 pages2020 IA 3rd YearpriyagerardNo ratings yet
- S. No. ContentDocument167 pagesS. No. ContentpriyagerardNo ratings yet
- Unit Iv Body Fluid AnalysisDocument8 pagesUnit Iv Body Fluid AnalysispriyagerardNo ratings yet
- Pathology Notes HemalathaDocument117 pagesPathology Notes HemalathapriyagerardNo ratings yet
- Anatomy and Physiology Tonsils: MRS. Priya GerardDocument11 pagesAnatomy and Physiology Tonsils: MRS. Priya GerardpriyagerardNo ratings yet
- Body Cavity FluidsDocument29 pagesBody Cavity FluidspriyagerardNo ratings yet
- Rns Can Work in A Variety of Healthcare Settings, IncludingDocument6 pagesRns Can Work in A Variety of Healthcare Settings, IncludingpriyagerardNo ratings yet
- CHN I & Ii Course PlanDocument17 pagesCHN I & Ii Course PlanpriyagerardNo ratings yet
- Unit Iv: Body Fluid AnalysisDocument41 pagesUnit Iv: Body Fluid AnalysispriyagerardNo ratings yet
- Transcranial Magnetic Stimulation: A. Shyam SundarDocument45 pagesTranscranial Magnetic Stimulation: A. Shyam SundarpriyagerardNo ratings yet
- Suicide: Risk Factors, Assessment, Methodological Problems: Sweta Sheth Chair: Dr. Rajesh GopalakrishnanDocument59 pagesSuicide: Risk Factors, Assessment, Methodological Problems: Sweta Sheth Chair: Dr. Rajesh GopalakrishnanpriyagerardNo ratings yet
- A Study To Assess The Effectiveness of Swallowing Exercises On Swallowing Ability Among Patients WithDocument8 pagesA Study To Assess The Effectiveness of Swallowing Exercises On Swallowing Ability Among Patients WithpriyagerardNo ratings yet
- Disorders of Perception - DR Avinash WaghmareDocument30 pagesDisorders of Perception - DR Avinash WaghmarepriyagerardNo ratings yet
- NSTP Common Module 2 Drug EducationDocument33 pagesNSTP Common Module 2 Drug EducationMerylle Shayne GustiloNo ratings yet
- Honey and Water Therapy by T BlendsDocument17 pagesHoney and Water Therapy by T BlendsRazkhal KunmoNo ratings yet
- Short Course Steroids in COVID-19Document11 pagesShort Course Steroids in COVID-19drupadhyaygunjanNo ratings yet
- Journal of Prosthodontics - 2022 - Alkhatib - Dental Floss Ties For Rubber Dam Isolation A Proposed Classification and ADocument7 pagesJournal of Prosthodontics - 2022 - Alkhatib - Dental Floss Ties For Rubber Dam Isolation A Proposed Classification and AAmmyNo ratings yet
- Risk Assessment For Stain RemovalDocument4 pagesRisk Assessment For Stain Removalطارق رضوانNo ratings yet
- CASE - Alzheimer's DiseaseDocument7 pagesCASE - Alzheimer's DiseaseMaryjoy OdatoNo ratings yet
- HLTHPS007 Student Work Book V2 15.02.19Document92 pagesHLTHPS007 Student Work Book V2 15.02.19Bùi Thắng0% (1)
- Injuria Renal Aguda PDFDocument7 pagesInjuria Renal Aguda PDFCaaarolNo ratings yet
- Reprocessing and Preparation of Devices BK 9103302 en Master 1904 2 PDFDocument36 pagesReprocessing and Preparation of Devices BK 9103302 en Master 1904 2 PDFCinthia PachecoNo ratings yet
- Annexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Document1 pageAnnexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Shrasti SoniNo ratings yet
- G AnesthesiaPersonnelDocument3 pagesG AnesthesiaPersonnelSudhakar AvanigaddaNo ratings yet
- Thesis Statement Examples On Breast CancerDocument5 pagesThesis Statement Examples On Breast Cancermcpvhiief100% (2)
- Prioritized Nursing Problems For Rabies: Nursing Diagnosis Nursing Interventions RationaleDocument2 pagesPrioritized Nursing Problems For Rabies: Nursing Diagnosis Nursing Interventions RationaleJessica SurmiedaNo ratings yet
- Self Assessment Guide Pharmacy Services NC IIIDocument6 pagesSelf Assessment Guide Pharmacy Services NC IIIAnesa TuñacaoNo ratings yet
- The Four Topics Chart:: A Tool For Clinical Ethics Case AnalysisDocument25 pagesThe Four Topics Chart:: A Tool For Clinical Ethics Case AnalysisZuzu FinusNo ratings yet
- Resume NdetahDocument1 pageResume Ndetahapi-484395670No ratings yet
- TuberculosisDocument4 pagesTuberculosisbcnguye4No ratings yet
- Candida Vulvovaginitis - Clinical Manifestations and Diagnosis - UpToDateDocument18 pagesCandida Vulvovaginitis - Clinical Manifestations and Diagnosis - UpToDateCindyNo ratings yet
- Primary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Document27 pagesPrimary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Keluang Man WinchesterNo ratings yet
- B2.4 Student WorksheetDocument5 pagesB2.4 Student WorksheetAbdullaahNo ratings yet
- Journal: SPMC Launches Journal of Health Care ServicesDocument2 pagesJournal: SPMC Launches Journal of Health Care ServicesAngelo RyanNo ratings yet
- Position Paper: General PublicDocument12 pagesPosition Paper: General PublicJohaima HaronNo ratings yet
- IBD SummaryDocument6 pagesIBD SummaryHuda Al-AnabrNo ratings yet
- PREMATURIIDocument91 pagesPREMATURIIAdriana MelnicNo ratings yet
- Mr. Maroof Khan: Speech and Language Pathologist/TherapistDocument15 pagesMr. Maroof Khan: Speech and Language Pathologist/TherapistshamsNo ratings yet
- Mystery Nursing Home Outbreak 3 Dead, 46 Miles From For Detrick in July 2019Document2 pagesMystery Nursing Home Outbreak 3 Dead, 46 Miles From For Detrick in July 2019Kevin SteinerNo ratings yet
- Basic Ethical Principles Stewards 1. StewardshipDocument7 pagesBasic Ethical Principles Stewards 1. StewardshipElla EllaNo ratings yet
- Amoxicillin Clavulanic Acid Prescribing InformationDocument25 pagesAmoxicillin Clavulanic Acid Prescribing InformationMohammed shamiul ShahidNo ratings yet
- NCM 104 Lec 5388: Mrs. Mary Antoinetter Aseron - 1 SemesterDocument6 pagesNCM 104 Lec 5388: Mrs. Mary Antoinetter Aseron - 1 SemesterSherlyn GarcesNo ratings yet














































































































Download as docx, pdf, or txt
You might also like
- Nursing Care Plan For HypertensionDocument4 pagesNursing Care Plan For HypertensionKathleen Dimacali100% (2)
- Name of The Candidate and AddressDocument16 pagesName of The Candidate and AddressYash RamawatNo ratings yet
- PHD Thesis: University of Medicine and Pharmacy CraiovaDocument10 pagesPHD Thesis: University of Medicine and Pharmacy CraiovapaulNo ratings yet
- Synopsis Proforma For Registration of Subject For DissertationDocument18 pagesSynopsis Proforma For Registration of Subject For DissertationKenneth Myro GarciaNo ratings yet
- Dysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Document7 pagesDysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Jihan FaadhilahNo ratings yet
- 05 N501 28766Document23 pages05 N501 28766Rumela Ganguly ChakrabortyNo ratings yet
- Study of Metabolic Syndrome and Diabetes Mellitus Among Ischemic Stroke Patients in A Tertiary Hospital, Northern KarnatakaDocument7 pagesStudy of Metabolic Syndrome and Diabetes Mellitus Among Ischemic Stroke Patients in A Tertiary Hospital, Northern KarnatakaIJAR JOURNALNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutnidaNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutmaydamayNo ratings yet
- Final Synopsis Format Sample ACNDocument25 pagesFinal Synopsis Format Sample ACNAbhijit DasNo ratings yet
- 17 Analysis of Maternal Outcome of General Versus Spinal Anaesthesia For Caesarean Delivery in Severe Pre EclampsiaDocument7 pages17 Analysis of Maternal Outcome of General Versus Spinal Anaesthesia For Caesarean Delivery in Severe Pre EclampsiaUlfa PuspitaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument14 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaAnna StimNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleUmar MukhtarNo ratings yet
- Seminar: Amy S Jordan, David G Mcsharry, Atul MalhotraDocument12 pagesSeminar: Amy S Jordan, David G Mcsharry, Atul MalhotraSerkan KüçüktürkNo ratings yet
- Jurnal Jantung 1Document7 pagesJurnal Jantung 1Egga Mariana YudaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaYadnya SaputraNo ratings yet
- Nutrients: The Use of Enteral Nutrition in The Management of StrokeDocument6 pagesNutrients: The Use of Enteral Nutrition in The Management of StrokeMita SeptoryNo ratings yet
- Nutrients: The Use of Enteral Nutrition in The Management of StrokeDocument6 pagesNutrients: The Use of Enteral Nutrition in The Management of StrokeMiranda MetriaNo ratings yet
- Evaluación de TosDocument8 pagesEvaluación de TosCarolina CelisNo ratings yet
- Journal Pre-Proof: Clinical NutritionDocument19 pagesJournal Pre-Proof: Clinical NutritionThay SousaNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument19 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaARJUN BNo ratings yet
- Swallow Respiratory Patterns and Aging Presbyphagia or DysphagiaDocument5 pagesSwallow Respiratory Patterns and Aging Presbyphagia or Dysphagiaariyanti rezekiNo ratings yet
- 05 N111 39956Document28 pages05 N111 39956Mahruri SaputraNo ratings yet
- Content ServerDocument8 pagesContent ServerG. Araya MoraNo ratings yet
- Prevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionDocument10 pagesPrevalence of and Factors Associated With Sarcopenia Among Elderly Individuals With HypertensionZaskia PutriNo ratings yet
- Refeeding Syndrome A Literature Review KhanDocument7 pagesRefeeding Syndrome A Literature Review Khangw060qpy100% (1)
- Psychological Aspects in Chronic Renal Failure: Review RticleDocument10 pagesPsychological Aspects in Chronic Renal Failure: Review RticleTry Febriani SiregarNo ratings yet
- Dysphagia Pada GeriatriDocument12 pagesDysphagia Pada Geriatrialfi syahrinNo ratings yet
- Summary ReportDocument27 pagesSummary ReportShweta GrigsonNo ratings yet
- "A Comparative Study To Assess Knowledge and Practice On Cardio Pulmonary Resuscitation Among Icu/Ccu NursesDocument21 pages"A Comparative Study To Assess Knowledge and Practice On Cardio Pulmonary Resuscitation Among Icu/Ccu NursesPushpa ChhillarNo ratings yet
- Final Pud CaseDocument155 pagesFinal Pud CaseLevy Garcia SanchezNo ratings yet
- 261-Article Text-435-1-10-20230103Document12 pages261-Article Text-435-1-10-20230103Vince Daniel VillalbaNo ratings yet
- 1 s2.0 S0753332220309148 MainDocument7 pages1 s2.0 S0753332220309148 Mainyayu latifahNo ratings yet
- Dysphagia in Older AdultsDocument10 pagesDysphagia in Older Adultsconstanza duran cordovaNo ratings yet
- Advances in Gerd: Management of Dysphagia in Stroke PatientsDocument3 pagesAdvances in Gerd: Management of Dysphagia in Stroke PatientsFeliciaNo ratings yet
- A Severe Asphyxiated Newborn: A Case ReportDocument13 pagesA Severe Asphyxiated Newborn: A Case ReportEeeeeeeeeNo ratings yet
- Case Presentation of Group 1Document45 pagesCase Presentation of Group 1Kirk Clarence FloresNo ratings yet
- 1625-Article Text-4407-1-10-20230707Document14 pages1625-Article Text-4407-1-10-20230707dewa putra yasaNo ratings yet
- Diana College of Nursing, No.68, Chokkanahalli, Jakkur Post, Bangalore-64Document28 pagesDiana College of Nursing, No.68, Chokkanahalli, Jakkur Post, Bangalore-64AnggraAnzhaniNo ratings yet
- Alvarez-Larruy2022 Article SpontaneousSwallowingFrequencyDocument11 pagesAlvarez-Larruy2022 Article SpontaneousSwallowingFrequencyYarisa Villar BonilloNo ratings yet
- Synopsis PallaviDocument31 pagesSynopsis PallaviSanjeet DuhanNo ratings yet
- Group 6 1Document48 pagesGroup 6 1baldosangelique14No ratings yet
- DiverticularDiseaseoftheColon PDFDocument12 pagesDiverticularDiseaseoftheColon PDFAdrian MucileanuNo ratings yet
- SarcopeniaDocument10 pagesSarcopeniaShuaib AhmadNo ratings yet
- Evaluacion Disfagia Esofagica Adulto MayorDocument24 pagesEvaluacion Disfagia Esofagica Adulto MayorPaulina Culebro EspinozaNo ratings yet
- Advpub JE20150123Document7 pagesAdvpub JE20150123Sherly KristiNo ratings yet
- The Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaDocument9 pagesThe Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaIJRASETPublicationsNo ratings yet
- Selección de Resúmenes de Menopausia Semana Del 30 de Julio Al 5 de Agosto de 2014Document3 pagesSelección de Resúmenes de Menopausia Semana Del 30 de Julio Al 5 de Agosto de 2014rocksurNo ratings yet
- GLX 041Document7 pagesGLX 041Tatta CamposNo ratings yet
- StudyDocument23 pagesStudyJose Paul RaderNo ratings yet
- Health Outcomes of Sarcopenia A Systematic ReviewDocument16 pagesHealth Outcomes of Sarcopenia A Systematic Reviewmanuel VenegasNo ratings yet
- MD Pulmonary Medicine Thesis TopicsDocument5 pagesMD Pulmonary Medicine Thesis Topicsamandareedsalem100% (2)
- Prevention of StrokeDocument10 pagesPrevention of StrokeRasvan Cristian StoicaNo ratings yet
- Nutrient Intake and Its Association With Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults A Population-Based StudyDocument11 pagesNutrient Intake and Its Association With Appendicular Total Lean Mass and Muscle Function and Strength in Older Adults A Population-Based StudyJetri HansNo ratings yet
- Impact of The Systematic Use of The Gugging Swallowing Screen inDocument15 pagesImpact of The Systematic Use of The Gugging Swallowing Screen inalexandraNo ratings yet
- Dr. MD Rezaul Karim Thesis Prevalance of Micro and Macrovascular Complications in Newly DetecDocument22 pagesDr. MD Rezaul Karim Thesis Prevalance of Micro and Macrovascular Complications in Newly Detecrezalata38100% (1)
- Selección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014Document5 pagesSelección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014rocksurNo ratings yet
- Ehf2 8 625Document9 pagesEhf2 8 625elza pratiwiNo ratings yet
- Perioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceDocument10 pagesPerioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceBRENDA VANESSA TREVIZO ESTRADANo ratings yet
- J.S.S College of Nursing 1 Main Saraswathipuram, MysoreDocument18 pagesJ.S.S College of Nursing 1 Main Saraswathipuram, MysoreNurul HafizaNo ratings yet
- Letter Seeking Experts For Content Validity of ToolDocument1 pageLetter Seeking Experts For Content Validity of ToolpriyagerardNo ratings yet
- Time Table-I - IV Year B.SC 2023Document36 pagesTime Table-I - IV Year B.SC 2023priyagerardNo ratings yet
- Adoption 150109001206 Conversion Gate01Document44 pagesAdoption 150109001206 Conversion Gate01priyagerardNo ratings yet
- College Report 2015Document120 pagesCollege Report 2015priyagerardNo ratings yet
- GNM Vol I Community Health Nursing Part 2 MinDocument446 pagesGNM Vol I Community Health Nursing Part 2 MinpriyagerardNo ratings yet
- BLINDNESSDocument24 pagesBLINDNESSpriyagerardNo ratings yet
- 4304 - M.Sc. - Community - Health - Nursing ImportantDocument84 pages4304 - M.Sc. - Community - Health - Nursing ImportantpriyagerardNo ratings yet
- International Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikDocument56 pagesInternational Classification of Diseases: Presented By: DR Arijit Kundu Guided By: Prof. Sumitra PattanaikpriyagerardNo ratings yet
- AMOEBIASISDocument31 pagesAMOEBIASISpriyagerard100% (1)
- 0 EndocrinedisordersseminarDocument52 pages0 EndocrinedisordersseminarpriyagerardNo ratings yet
- Nursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)Document35 pagesNursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)priyagerardNo ratings yet
- 2020 IA 3rd YearDocument7 pages2020 IA 3rd YearpriyagerardNo ratings yet
- S. No. ContentDocument167 pagesS. No. ContentpriyagerardNo ratings yet
- Unit Iv Body Fluid AnalysisDocument8 pagesUnit Iv Body Fluid AnalysispriyagerardNo ratings yet
- Pathology Notes HemalathaDocument117 pagesPathology Notes HemalathapriyagerardNo ratings yet
- Anatomy and Physiology Tonsils: MRS. Priya GerardDocument11 pagesAnatomy and Physiology Tonsils: MRS. Priya GerardpriyagerardNo ratings yet
- Body Cavity FluidsDocument29 pagesBody Cavity FluidspriyagerardNo ratings yet
- Rns Can Work in A Variety of Healthcare Settings, IncludingDocument6 pagesRns Can Work in A Variety of Healthcare Settings, IncludingpriyagerardNo ratings yet
- CHN I & Ii Course PlanDocument17 pagesCHN I & Ii Course PlanpriyagerardNo ratings yet
- Unit Iv: Body Fluid AnalysisDocument41 pagesUnit Iv: Body Fluid AnalysispriyagerardNo ratings yet
- Transcranial Magnetic Stimulation: A. Shyam SundarDocument45 pagesTranscranial Magnetic Stimulation: A. Shyam SundarpriyagerardNo ratings yet
- Suicide: Risk Factors, Assessment, Methodological Problems: Sweta Sheth Chair: Dr. Rajesh GopalakrishnanDocument59 pagesSuicide: Risk Factors, Assessment, Methodological Problems: Sweta Sheth Chair: Dr. Rajesh GopalakrishnanpriyagerardNo ratings yet
- A Study To Assess The Effectiveness of Swallowing Exercises On Swallowing Ability Among Patients WithDocument8 pagesA Study To Assess The Effectiveness of Swallowing Exercises On Swallowing Ability Among Patients WithpriyagerardNo ratings yet
- Disorders of Perception - DR Avinash WaghmareDocument30 pagesDisorders of Perception - DR Avinash WaghmarepriyagerardNo ratings yet
- NSTP Common Module 2 Drug EducationDocument33 pagesNSTP Common Module 2 Drug EducationMerylle Shayne GustiloNo ratings yet
- Honey and Water Therapy by T BlendsDocument17 pagesHoney and Water Therapy by T BlendsRazkhal KunmoNo ratings yet
- Short Course Steroids in COVID-19Document11 pagesShort Course Steroids in COVID-19drupadhyaygunjanNo ratings yet
- Journal of Prosthodontics - 2022 - Alkhatib - Dental Floss Ties For Rubber Dam Isolation A Proposed Classification and ADocument7 pagesJournal of Prosthodontics - 2022 - Alkhatib - Dental Floss Ties For Rubber Dam Isolation A Proposed Classification and AAmmyNo ratings yet
- Risk Assessment For Stain RemovalDocument4 pagesRisk Assessment For Stain Removalطارق رضوانNo ratings yet
- CASE - Alzheimer's DiseaseDocument7 pagesCASE - Alzheimer's DiseaseMaryjoy OdatoNo ratings yet
- HLTHPS007 Student Work Book V2 15.02.19Document92 pagesHLTHPS007 Student Work Book V2 15.02.19Bùi Thắng0% (1)
- Injuria Renal Aguda PDFDocument7 pagesInjuria Renal Aguda PDFCaaarolNo ratings yet
- Reprocessing and Preparation of Devices BK 9103302 en Master 1904 2 PDFDocument36 pagesReprocessing and Preparation of Devices BK 9103302 en Master 1904 2 PDFCinthia PachecoNo ratings yet
- Annexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Document1 pageAnnexure II Compulsory Health Certificate For Kumbh Mela Haridwar - 2021Shrasti SoniNo ratings yet
- G AnesthesiaPersonnelDocument3 pagesG AnesthesiaPersonnelSudhakar AvanigaddaNo ratings yet
- Thesis Statement Examples On Breast CancerDocument5 pagesThesis Statement Examples On Breast Cancermcpvhiief100% (2)
- Prioritized Nursing Problems For Rabies: Nursing Diagnosis Nursing Interventions RationaleDocument2 pagesPrioritized Nursing Problems For Rabies: Nursing Diagnosis Nursing Interventions RationaleJessica SurmiedaNo ratings yet
- Self Assessment Guide Pharmacy Services NC IIIDocument6 pagesSelf Assessment Guide Pharmacy Services NC IIIAnesa TuñacaoNo ratings yet
- The Four Topics Chart:: A Tool For Clinical Ethics Case AnalysisDocument25 pagesThe Four Topics Chart:: A Tool For Clinical Ethics Case AnalysisZuzu FinusNo ratings yet
- Resume NdetahDocument1 pageResume Ndetahapi-484395670No ratings yet
- TuberculosisDocument4 pagesTuberculosisbcnguye4No ratings yet
- Candida Vulvovaginitis - Clinical Manifestations and Diagnosis - UpToDateDocument18 pagesCandida Vulvovaginitis - Clinical Manifestations and Diagnosis - UpToDateCindyNo ratings yet
- Primary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Document27 pagesPrimary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Keluang Man WinchesterNo ratings yet
- B2.4 Student WorksheetDocument5 pagesB2.4 Student WorksheetAbdullaahNo ratings yet
- Journal: SPMC Launches Journal of Health Care ServicesDocument2 pagesJournal: SPMC Launches Journal of Health Care ServicesAngelo RyanNo ratings yet
- Position Paper: General PublicDocument12 pagesPosition Paper: General PublicJohaima HaronNo ratings yet
- IBD SummaryDocument6 pagesIBD SummaryHuda Al-AnabrNo ratings yet
- PREMATURIIDocument91 pagesPREMATURIIAdriana MelnicNo ratings yet
- Mr. Maroof Khan: Speech and Language Pathologist/TherapistDocument15 pagesMr. Maroof Khan: Speech and Language Pathologist/TherapistshamsNo ratings yet
- Mystery Nursing Home Outbreak 3 Dead, 46 Miles From For Detrick in July 2019Document2 pagesMystery Nursing Home Outbreak 3 Dead, 46 Miles From For Detrick in July 2019Kevin SteinerNo ratings yet
- Basic Ethical Principles Stewards 1. StewardshipDocument7 pagesBasic Ethical Principles Stewards 1. StewardshipElla EllaNo ratings yet
- Amoxicillin Clavulanic Acid Prescribing InformationDocument25 pagesAmoxicillin Clavulanic Acid Prescribing InformationMohammed shamiul ShahidNo ratings yet
- NCM 104 Lec 5388: Mrs. Mary Antoinetter Aseron - 1 SemesterDocument6 pagesNCM 104 Lec 5388: Mrs. Mary Antoinetter Aseron - 1 SemesterSherlyn GarcesNo ratings yet