Download as docx, pdf, or txt
You might also like
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito75% (4)
- Pretest IV TherapyDocument3 pagesPretest IV TherapyMeranda Martin0% (2)
- NCLEX RN Review For Reduction of Risk PotentialDocument7 pagesNCLEX RN Review For Reduction of Risk Potentialpaulinatia100% (1)
- IV InsertionDocument18 pagesIV InsertionRochelle Valero100% (2)
- IV CannulationDocument10 pagesIV CannulationDatta Bedkkir100% (1)
- Practice Teaching Demonstration: Intravenous InfusionDocument11 pagesPractice Teaching Demonstration: Intravenous InfusionMegha lakraNo ratings yet
- Sim Scenario 4Document31 pagesSim Scenario 4lilchibaby3161No ratings yet
- On IV TherapyDocument40 pagesOn IV TherapyDeology Juanino79% (14)
- Topic: Intravenous Cannulation, Therapy and Blood TransfusionDocument32 pagesTopic: Intravenous Cannulation, Therapy and Blood TransfusionAngelica Kaye BuanNo ratings yet
- Intravenous TherapyDocument22 pagesIntravenous TherapyMatt Lao Dionela100% (1)
- DIALYSISDocument21 pagesDIALYSISEadrian ReyesNo ratings yet
- IV TherapyDocument9 pagesIV TherapyJackson Pukya Gabino PabloNo ratings yet
- Intravenous Therapy Is Treatment That Infuses Intravenous Solutions, Medications, Blood, or BloodDocument5 pagesIntravenous Therapy Is Treatment That Infuses Intravenous Solutions, Medications, Blood, or BloodShehada Marcos BondadNo ratings yet
- C 13Document11 pagesC 13Jo100% (1)
- IV InsertionDocument22 pagesIV InsertionRA100% (1)
- IV Therapy SsDocument56 pagesIV Therapy Sssaeed_chohan100% (8)
- Hazards For IV Therapy-1Document9 pagesHazards For IV Therapy-1Arooj HussainNo ratings yet
- IV Therapy: AdvantagesDocument9 pagesIV Therapy: AdvantagesKaren HutchinsonNo ratings yet
- Tugas 1 Ne Nurul HendrianiDocument6 pagesTugas 1 Ne Nurul HendrianiNurul HendrianiNo ratings yet
- IV InsertionDocument17 pagesIV Insertionleih jsNo ratings yet
- IV Cannulation CourseDocument6 pagesIV Cannulation CourseKaiwan AzadNo ratings yet
- Complications of IV TherapyDocument6 pagesComplications of IV TherapyLorilei Rose JuntillaNo ratings yet
- Intravenous Therapy A. DefinitionDocument18 pagesIntravenous Therapy A. Definitionlainey101No ratings yet
- Nursing Proses Diabetes ESRDDocument9 pagesNursing Proses Diabetes ESRDJamilah SudinNo ratings yet
- Infection Control During IV AsesesDocument20 pagesInfection Control During IV AsesesVineeth venuNo ratings yet
- Are Over 40 Years of Age.: Nonsteroidal Anti-Inflammatory Drugs (Nsaids)Document10 pagesAre Over 40 Years of Age.: Nonsteroidal Anti-Inflammatory Drugs (Nsaids)Anjali NaudiyalNo ratings yet
- Intravenous FluidsDocument3 pagesIntravenous FluidsKristine Artes AguilarNo ratings yet
- Port A CathDocument14 pagesPort A CathMerika JimenezNo ratings yet
- Assessing Iv SiteDocument7 pagesAssessing Iv SiteFaviano AnceroNo ratings yet
- Level 3 - NCM 112j RLE: ALTAR, Catherine Sienna B. (180777) BSN 3 - DDocument3 pagesLevel 3 - NCM 112j RLE: ALTAR, Catherine Sienna B. (180777) BSN 3 - DsenyorakathNo ratings yet
- PB2 NP3Document8 pagesPB2 NP3Herne BalberdeNo ratings yet
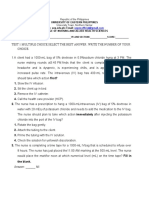
- Name: - Yr and Section: - ScoreDocument12 pagesName: - Yr and Section: - Scoregabrielle magdaraogNo ratings yet
- Iv Therapy: Presented By: Steven Jones, NREMT-PDocument29 pagesIv Therapy: Presented By: Steven Jones, NREMT-Pbalab2311No ratings yet
- PMLS Lesson 5Document3 pagesPMLS Lesson 5Void MelromarcNo ratings yet
- Newborn Critical Care Center (NCCC) Guidelines: Umbilical Line PlacementDocument5 pagesNewborn Critical Care Center (NCCC) Guidelines: Umbilical Line PlacementMyra BuellaNo ratings yet
- Nursing Care Plan An Unoccupied Bed Is PreparedDocument13 pagesNursing Care Plan An Unoccupied Bed Is PreparedDevhan RyuNo ratings yet
- Intrevenous TherapyDocument5 pagesIntrevenous TherapyCharles DoradoNo ratings yet
- Approved: June 7, 2017 21: Page 1 ofDocument21 pagesApproved: June 7, 2017 21: Page 1 ofmalathiNo ratings yet
- Exam Preparation League #30 by Subhash ChoudharyDocument5 pagesExam Preparation League #30 by Subhash ChoudharySubhash chandNo ratings yet
- Intravenous TherapyDocument10 pagesIntravenous TherapyS. AmberNo ratings yet
- Intravenous (IV) CannulationDocument6 pagesIntravenous (IV) CannulationSahaaneiy IlmeeNo ratings yet
- What Is Infusion TherapyDocument14 pagesWhat Is Infusion Therapybeautifulme031690No ratings yet
- Abdominal ParacentesisDocument5 pagesAbdominal ParacentesisVijith.V.kumar100% (1)
- 9, Procedure of PICCDocument9 pages9, Procedure of PICCputriseptinaNo ratings yet
- INTRAVENOUSDocument38 pagesINTRAVENOUSLorelyn DelfinNo ratings yet
- 2008 NP4Document11 pages2008 NP4Jeremiash Noblesala Dela CruzNo ratings yet
- Port-A-Cath: Ayah Omairi Mrs. Boughdana JaberDocument13 pagesPort-A-Cath: Ayah Omairi Mrs. Boughdana Jaberayah omairi100% (1)
- IVT ComplicationsDocument4 pagesIVT ComplicationsAlthea AlcalaNo ratings yet
- Central Venous Catheters: Iv Terapy &Document71 pagesCentral Venous Catheters: Iv Terapy &Florence Liem0% (1)
- Chest Drainage Medical ManagementDocument3 pagesChest Drainage Medical ManagementPaul John RutaquioNo ratings yet
- National Norcet Test-2 (Answer Key)Document97 pagesNational Norcet Test-2 (Answer Key)SHIVANIINo ratings yet
- Pmlslec M003 PDFDocument7 pagesPmlslec M003 PDFpasswordNo ratings yet
- DocumentDocument13 pagesDocumentGlynn AposagaNo ratings yet
- 9 Intravenous TherapyDocument23 pages9 Intravenous TherapyKareem Mae Pines RaborNo ratings yet
- ASSISTING IV INSERTION V 2Document2 pagesASSISTING IV INSERTION V 2Kim XiaoNo ratings yet
- DIALYSISDocument7 pagesDIALYSISIvy E. LantapeNo ratings yet
- HemodialysisDocument30 pagesHemodialysiswaadessa1No ratings yet
- Nursezone 4 Floor Florentine Bldg. Bonifacio St. Davao City 2865436Document4 pagesNursezone 4 Floor Florentine Bldg. Bonifacio St. Davao City 2865436Bok Delos SantosNo ratings yet
- EMERGENCY MEIDICINE - IV - Access - PrintableDocument5 pagesEMERGENCY MEIDICINE - IV - Access - PrintableMedic DestinationNo ratings yet
- Intravenous Therapy Administration: a practical guideFrom EverandIntravenous Therapy Administration: a practical guideRating: 4 out of 5 stars4/5 (1)
- NCM: 112 Care of The Client With Problem in Oxygenation Venipuncture Using Needle or CatheterDocument7 pagesNCM: 112 Care of The Client With Problem in Oxygenation Venipuncture Using Needle or CatheterIssaiah Nicolle CeciliaNo ratings yet
- CECILIA, ISSAIAH NICOLLE-EvaluationDocument1 pageCECILIA, ISSAIAH NICOLLE-EvaluationIssaiah Nicolle CeciliaNo ratings yet
- Cecilia, Issaiah Nicolle-Pneumothorax-NcpDocument7 pagesCecilia, Issaiah Nicolle-Pneumothorax-NcpIssaiah Nicolle Cecilia100% (1)
- Issaiah Nicolle L. Cecilia 3 BSN - ADocument14 pagesIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- Issaiah Nicolle L. Cecilia 3 BSN - ADocument2 pagesIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- Issaiah Nicolle L. Cecilia 3 BSN - ADocument6 pagesIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- Group 3 Group 3: 3 BSN - A 3 BSN - ADocument71 pagesGroup 3 Group 3: 3 BSN - A 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- Issaiah Nicolle L. Cecilia 3 BSN - ADocument2 pagesIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- Issaiah Nicolle L. Cecilia 3 BSN - A: Peaks in 30 To 60 Minutes Peaks in 5 To 6 HoursDocument2 pagesIssaiah Nicolle L. Cecilia 3 BSN - A: Peaks in 30 To 60 Minutes Peaks in 5 To 6 HoursIssaiah Nicolle CeciliaNo ratings yet
- Operational FrameworkDocument2 pagesOperational FrameworkIssaiah Nicolle CeciliaNo ratings yet
- Warm Water Compress As An Alternative For Decreasing The Degree of Superficial Phlebitis in Children During HospitalizationDocument8 pagesWarm Water Compress As An Alternative For Decreasing The Degree of Superficial Phlebitis in Children During HospitalizationYogi SastrawanNo ratings yet
- DOCUMENTATION: Written, Legal Record Of: Problems and Contributes inDocument11 pagesDOCUMENTATION: Written, Legal Record Of: Problems and Contributes inChristine Ann GotanNo ratings yet
- Evaluación de Las Prácticas Seguras de Inyección en Los Establecimientos de Salud de OmánDocument9 pagesEvaluación de Las Prácticas Seguras de Inyección en Los Establecimientos de Salud de OmánGeraldine Arana LandaetaNo ratings yet
- DylojectDocument4 pagesDylojectranachamanNo ratings yet
- Amphotericin B: Component Mg/liter Mol. Wt. Mol. (MM)Document7 pagesAmphotericin B: Component Mg/liter Mol. Wt. Mol. (MM)Echa Alifyanty SyarifNo ratings yet
- French PADocument5 pagesFrench PADaniel PeprahNo ratings yet
- Fluids in Surgery 1 1Document43 pagesFluids in Surgery 1 1محمد عماد عليNo ratings yet
- 3Document232 pages3Dipeshwari ThakreNo ratings yet
- Centrel Venous CatheterizationDocument77 pagesCentrel Venous CatheterizationAli100% (1)
- BD Alaris Plus Transfer Tool DFU BDDF00494 enDocument18 pagesBD Alaris Plus Transfer Tool DFU BDDF00494 enWaleed Ah-DhaifiNo ratings yet
- Acoustic Lens Improves Superficial In-Plane Ultrasound-Guided ProceduresDocument6 pagesAcoustic Lens Improves Superficial In-Plane Ultrasound-Guided ProceduresHarm ScholtenNo ratings yet
- Jeremy Diehl ResumeDocument2 pagesJeremy Diehl Resumeapi-437018433No ratings yet
- Heart Transplant Surgery - Docx 2Document6 pagesHeart Transplant Surgery - Docx 2oguzguneri2010No ratings yet
- ALCON CatalogDocument56 pagesALCON CatalogpabloNo ratings yet
- Fundamentals of NursingDocument13 pagesFundamentals of NursingGiselle Chloe Baluya icoNo ratings yet
- Insert INFUSAN D5 + NSDocument2 pagesInsert INFUSAN D5 + NSNurul HusnaNo ratings yet
- Extravasation GuidanceDocument24 pagesExtravasation Guidancechercal100% (1)
- Handouts For Drug CalculationDocument19 pagesHandouts For Drug CalculationEmeroot RootNo ratings yet
- Phlebotomy in A NutshellDocument131 pagesPhlebotomy in A Nutshellgreen_archerNo ratings yet
- Hypovolemic Shock TEXTDocument5 pagesHypovolemic Shock TEXTrhen1991No ratings yet
- Endocrine EmergencyDocument24 pagesEndocrine EmergencymalarmathiNo ratings yet
- NLE Compilation 1 Q PDFDocument67 pagesNLE Compilation 1 Q PDFKc Orense100% (3)
- Calcium AcetateDocument3 pagesCalcium AcetateKIM NAMJOON'S PEACHES & CREAM100% (1)
- LucidaDocument9 pagesLucidaErwin SutejoNo ratings yet
- WEEK 1 HTN Crisis QDocument5 pagesWEEK 1 HTN Crisis QBanana QNo ratings yet
- Soumya S Nair Biodata 4-07Document24 pagesSoumya S Nair Biodata 4-07ElizabethNo ratings yet
- Revision For PONDocument4 pagesRevision For PONSandra YeboaaNo ratings yet
- Resume Canada - NurseDocument2 pagesResume Canada - NurseDiana KalengaNo ratings yet