Download as docx, pdf, or txt
You might also like
- Marieb 2015 11th 0321919009 SampleDocument31 pagesMarieb 2015 11th 0321919009 SampleJoe Chill100% (1)
- Oxygen Dissociation CurvesDocument11 pagesOxygen Dissociation CurvesSajin Sali75% (4)
- Basics of Neonatal Ventilation 1Document42 pagesBasics of Neonatal Ventilation 1Abid Ali Rizvi100% (1)
- Respiration in Fish N FrogDocument23 pagesRespiration in Fish N FrogHazirah HussinNo ratings yet
- Pulmonary Function TestingDocument35 pagesPulmonary Function TestingMartha ChaseNo ratings yet
- Pulmonary Function TestsDocument65 pagesPulmonary Function TestsPranathi PrasadNo ratings yet
- 5-Pulmonary Function TestsDocument35 pages5-Pulmonary Function TestsDoha JKNo ratings yet
- Introduction To Pulmonary Function TestingDocument58 pagesIntroduction To Pulmonary Function Testingpescao50% (1)
- Respi Update 2019 SpirometryDocument48 pagesRespi Update 2019 SpirometryJashveerBedi100% (1)
- Pulmonary Function TestingDocument53 pagesPulmonary Function TestingAyeNo ratings yet
- Pulmonary Function Tests-Nursing MasenoDocument43 pagesPulmonary Function Tests-Nursing Masenoakoeljames8543No ratings yet
- GOLD Spirometry 2010Document59 pagesGOLD Spirometry 2010Ck Kma100% (1)
- Interpretasi Hasil Faal Paru DR - DanielDocument33 pagesInterpretasi Hasil Faal Paru DR - DanielAyahnya RafliNo ratings yet
- Pulmonary Function TestDocument57 pagesPulmonary Function TestDeepika PatelNo ratings yet
- L 3 SpirmetryDocument24 pagesL 3 SpirmetryXajepoxNo ratings yet
- Pulmonary Function TestsDocument25 pagesPulmonary Function TestsRaviNo ratings yet
- An Approach To Interpreting Spirometry (Finals) PDFDocument25 pagesAn Approach To Interpreting Spirometry (Finals) PDFVanessa CarinoNo ratings yet
- SpirometryDocument47 pagesSpirometrydrmahayousif7451100% (2)
- Pulmonary Function Test, JARA CSUDocument73 pagesPulmonary Function Test, JARA CSUJohn NicoleNo ratings yet
- Spirometry in Primary Care: Global Initiative For Chronic Obstructive Lung Disease (GOLD) 2008Document59 pagesSpirometry in Primary Care: Global Initiative For Chronic Obstructive Lung Disease (GOLD) 2008zulfikar adiNo ratings yet
- Seminar Teste Functionale Studenti-51818Document50 pagesSeminar Teste Functionale Studenti-51818Daniela RobuNo ratings yet
- Pulmonary Function TestingDocument62 pagesPulmonary Function TestingWiz SamNo ratings yet
- Pulmonary Function Testing: Camilla Hollen, MMS, PA-C PA 530Document49 pagesPulmonary Function Testing: Camilla Hollen, MMS, PA-C PA 530KatherynSotoNo ratings yet
- LVRSDocument52 pagesLVRSmahmod omerNo ratings yet
- Pulmonary Function HandoutDocument50 pagesPulmonary Function HandoutAbed SabeNo ratings yet
- LVRSDocument52 pagesLVRSmahmod omerNo ratings yet
- PFT VMDocument71 pagesPFT VMVishnu ManglaNo ratings yet
- Pulmonary Eval Amd LabDocument58 pagesPulmonary Eval Amd LabSara DuranNo ratings yet
- Spirometry: DR Sharan SubramanianDocument38 pagesSpirometry: DR Sharan SubramanianPunit GargNo ratings yet
- Pulmonary Function TestsDocument26 pagesPulmonary Function TestsShodhan PatelNo ratings yet
- Pulmonary Function TestDocument18 pagesPulmonary Function TestelinelisaNo ratings yet
- SpiroDocument31 pagesSpiroMoh Arif KurniawanNo ratings yet
- 02 2018 Biomedical Instrumentation - Measurement of RespirationDocument28 pages02 2018 Biomedical Instrumentation - Measurement of Respirationviki mikiNo ratings yet
- Pulmonary Function Tests - DR MoiseDocument39 pagesPulmonary Function Tests - DR MoisemathemoisemedNo ratings yet
- Spirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Document60 pagesSpirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Alkaustariyah LubisNo ratings yet
- Spirometry Importance Performing and Interpretation Case ReportsDocument149 pagesSpirometry Importance Performing and Interpretation Case ReportsAnonymous eZqDZbObRi100% (1)
- Pulmonary Function Tests: Measuring The Capacity For Life Esmeralda E. Morales, MD September 21, 2004Document54 pagesPulmonary Function Tests: Measuring The Capacity For Life Esmeralda E. Morales, MD September 21, 2004Ronnie JaderNo ratings yet
- Corrected PFT JayatiDocument43 pagesCorrected PFT JayatiKRIPAL BARDHANNo ratings yet
- Interpreting Pulmonary Function TestsDocument10 pagesInterpreting Pulmonary Function TestsSuresh Kumar100% (1)
- Pulmonary Function TestDocument13 pagesPulmonary Function TestsajjadNo ratings yet
- Basics of Ventilatory SupportDocument43 pagesBasics of Ventilatory SupportAdhithya Bhat100% (1)
- Intra-Operative PEEP Vs ZEEPDocument37 pagesIntra-Operative PEEP Vs ZEEPMohamed RifanNo ratings yet
- Pulmonary Function Test (PFT)Document24 pagesPulmonary Function Test (PFT)hm3398No ratings yet
- Lab 6Document22 pagesLab 6202310446No ratings yet
- BOOK Spirometry in PracticeDocument104 pagesBOOK Spirometry in Practicenadeem khan100% (1)
- SpirometryDocument29 pagesSpirometrydrnasir31No ratings yet
- Lung Function Tests: Yazeed Abed El KhaleqDocument35 pagesLung Function Tests: Yazeed Abed El KhaleqYazeedNo ratings yet
- Pulmonary Function TestsDocument24 pagesPulmonary Function TestsSachin KonkaniNo ratings yet
- Pulmonary Function TestsDocument29 pagesPulmonary Function TestsOrion JohnNo ratings yet
- Lung Volumes and CapacitiesDocument15 pagesLung Volumes and CapacitiesEvangelin Melvin100% (1)
- Ratnawati - Spirometry For Diagnosis OLDDocument61 pagesRatnawati - Spirometry For Diagnosis OLDAndry Wahyudi AgusNo ratings yet
- BBB 1 - Pulmonary Function Tests InterpretationDocument14 pagesBBB 1 - Pulmonary Function Tests InterpretationArhanNo ratings yet
- Spirometry For Diagnosis of CopdDocument4 pagesSpirometry For Diagnosis of CopdriasaliNo ratings yet
- Spirometri DR Zuhrial SPPDDocument68 pagesSpirometri DR Zuhrial SPPDx22xNo ratings yet
- Pulmonary Function TestDocument21 pagesPulmonary Function TestAbhi LodhwalNo ratings yet
- Understanding Mechanical Ventilation: Jennifer Zanni, PT, DSCPT Johns Hopkins HospitalDocument52 pagesUnderstanding Mechanical Ventilation: Jennifer Zanni, PT, DSCPT Johns Hopkins HospitalDeepa BhattacharjeeNo ratings yet
- 2 POCUS in Emergency FAST IVC LUNGresidents December 2022Document92 pages2 POCUS in Emergency FAST IVC LUNGresidents December 2022dr mohd abdul basithNo ratings yet
- Prezentare Caz Clinic Ventilatia Mecanica IntraoperatorieDocument55 pagesPrezentare Caz Clinic Ventilatia Mecanica Intraoperatorieralucaioana89No ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Regulation OF Respiration.: DR Arpana HazarikaDocument53 pagesRegulation OF Respiration.: DR Arpana HazarikaDorin PathakNo ratings yet
- Pregnancytests 180321025548Document51 pagesPregnancytests 180321025548Dorin PathakNo ratings yet
- Physiologyofequilibriumbalance 111029153537 Phpapp01Document43 pagesPhysiologyofequilibriumbalance 111029153537 Phpapp01Dorin PathakNo ratings yet
- Reflex DR Arpana HazarikaDocument126 pagesReflex DR Arpana HazarikaDorin Pathak100% (1)
- Anatomy, Physiology of Neuromuscular Junction & Its DisordersDocument26 pagesAnatomy, Physiology of Neuromuscular Junction & Its DisordersDorin PathakNo ratings yet
- Muscle Spindle and Muscle ToneDocument100 pagesMuscle Spindle and Muscle ToneDorin PathakNo ratings yet
- Learning Outcome: Electroencephalogram (EEG)Document29 pagesLearning Outcome: Electroencephalogram (EEG)Dorin PathakNo ratings yet
- Effect of Life Style Changes On Cardiovascular Autonomic FunctionDocument3 pagesEffect of Life Style Changes On Cardiovascular Autonomic FunctionDorin PathakNo ratings yet
- Organization of Nervous System - MBBS NewDocument53 pagesOrganization of Nervous System - MBBS NewDorin PathakNo ratings yet
- Post Covid Symtom ArticleDocument1 pagePost Covid Symtom ArticleDorin PathakNo ratings yet
- Cerebral Cortex 1Document37 pagesCerebral Cortex 1Dorin PathakNo ratings yet
- Cogulation Profile: Bleeding Time, Clotting Time, PT, and PTTDocument49 pagesCogulation Profile: Bleeding Time, Clotting Time, PT, and PTTDorin PathakNo ratings yet
- Hypoxia: Dr. Jyoti Prasad Deori Assistant Professor Dept of PhysiologyDocument35 pagesHypoxia: Dr. Jyoti Prasad Deori Assistant Professor Dept of PhysiologyDorin PathakNo ratings yet
- Speec H: DR Jyoti Prasad DeoriDocument32 pagesSpeec H: DR Jyoti Prasad DeoriDorin PathakNo ratings yet
- Membrane Potential: Dr. Arpana HazarikaDocument22 pagesMembrane Potential: Dr. Arpana HazarikaDorin PathakNo ratings yet
- Anti Haemostatic MechanismDocument29 pagesAnti Haemostatic MechanismDorin PathakNo ratings yet
- Cardiovascular. SocioeconomicDocument4 pagesCardiovascular. SocioeconomicDorin PathakNo ratings yet
- Presented by Cathrine Diana PGI Dept of Oral and Maxillofacial SurgeryDocument78 pagesPresented by Cathrine Diana PGI Dept of Oral and Maxillofacial SurgeryDorin PathakNo ratings yet
- Smooth MuscleDocument33 pagesSmooth MuscleDorin PathakNo ratings yet
- A Descriptive Study To Assess The Knowledge and Practice Regarding Ventilator Associated Pneumonia VAP Critical Care Bundle Among Students of Selected Nursing Colleges of Distt. Mohali, PunjabDocument5 pagesA Descriptive Study To Assess The Knowledge and Practice Regarding Ventilator Associated Pneumonia VAP Critical Care Bundle Among Students of Selected Nursing Colleges of Distt. Mohali, PunjabEditor IJTSRDNo ratings yet
- Department of Education: Republic of The PhilippinesDocument9 pagesDepartment of Education: Republic of The PhilippinesZyryll VegaNo ratings yet
- Act 2 Mechanisms of Gas ExchangeDocument7 pagesAct 2 Mechanisms of Gas ExchangeTyrone Dave BalitaNo ratings yet
- Class 11 - Biology - Respiration in PlantsDocument13 pagesClass 11 - Biology - Respiration in PlantsDivyansheeNo ratings yet
- RespiratorypptDocument69 pagesRespiratorypptMichelle RotairoNo ratings yet
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationDocument75 pagesACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelNo ratings yet
- Neonatal Respiratory Distress - A Practical Approach To Its Diagnosis and Management 2015Document17 pagesNeonatal Respiratory Distress - A Practical Approach To Its Diagnosis and Management 2015Lissey FloresNo ratings yet
- Carescape R860 Spec SheetDocument8 pagesCarescape R860 Spec SheetBaldomero MartínezNo ratings yet
- Lesson 3 ReviewDocument4 pagesLesson 3 ReviewHo Yong WaiNo ratings yet
- Case - Vii: AsthmaDocument18 pagesCase - Vii: AsthmaabubakarNo ratings yet
- Candidate Mcqs Week 12 PhysiologyDocument3 pagesCandidate Mcqs Week 12 PhysiologyAzizNo ratings yet
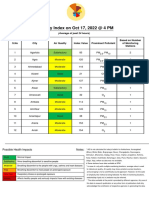
- AQI Bulletin 20221017Document14 pagesAQI Bulletin 20221017Amrish TrivediNo ratings yet
- 2.0 Respiration: 2.1 Respiratory System 2.5 Gaseous Exchange in PlantsDocument1 page2.0 Respiration: 2.1 Respiratory System 2.5 Gaseous Exchange in PlantsaslendabasarNo ratings yet
- Electron Transport and Oxidative Phosphorylation: Paul D. Adams - University of ArkansasDocument43 pagesElectron Transport and Oxidative Phosphorylation: Paul D. Adams - University of ArkansasKrishly Ann Medina SalazarNo ratings yet
- Earth and Life Science SHS 16.3 How Organisms Obtain and Utilize EnergyDocument23 pagesEarth and Life Science SHS 16.3 How Organisms Obtain and Utilize EnergyPamela MalihanNo ratings yet
- Tecline Catalog - EnglishDocument27 pagesTecline Catalog - EnglishMTNo ratings yet
- Meconium Aspiration Syndrome (MAS)Document12 pagesMeconium Aspiration Syndrome (MAS)Angela AmaoNo ratings yet
- Respiratory Physiology PregnancyDocument13 pagesRespiratory Physiology PregnancyAlejandra RequesensNo ratings yet
- Chronic Obstructive Pulmonary Disease Bronchitis Nursing Care PlansDocument10 pagesChronic Obstructive Pulmonary Disease Bronchitis Nursing Care Planscy belNo ratings yet
- Abg CpuDocument49 pagesAbg Cpugwen pencerNo ratings yet
- Respiratory System Anatomy, Assessment & Diagnostic TestsDocument24 pagesRespiratory System Anatomy, Assessment & Diagnostic TestsPrince Rener Velasco PeraNo ratings yet
- Mechanical Ventilation SeminarDocument82 pagesMechanical Ventilation Seminarrajan kumar91% (22)
- Chapter 1: Respiration: ObjectiveDocument3 pagesChapter 1: Respiration: ObjectiveYugenNo ratings yet
- S9 - Q1 - Week 7Document11 pagesS9 - Q1 - Week 7Janice Apole FabioNo ratings yet
- Format Penilaian Bleef TestDocument4 pagesFormat Penilaian Bleef TestNelismi Nelismi100% (4)
- The Respiratory System (Handouts)Document6 pagesThe Respiratory System (Handouts)EdNo ratings yet