Download as docx, pdf, or txt
You might also like
- IIMC Consulting Casebook 2022-23Document147 pagesIIMC Consulting Casebook 2022-23Aarti Kumari100% (2)
- Presentation Fabrication of Storage TankDocument43 pagesPresentation Fabrication of Storage TankAbdul Manaf100% (1)
- Fisheries Post Harvest: 3 Units Instructor: Annie T. OmotoDocument4 pagesFisheries Post Harvest: 3 Units Instructor: Annie T. OmotoChuck SupelanaNo ratings yet
- Science-Related Related Issues and Problems in The CountryDocument3 pagesScience-Related Related Issues and Problems in The CountryRonalyn PaunalNo ratings yet
- Astm A-615Document8 pagesAstm A-615bill_lee_24267% (6)
- AeromodellingDocument15 pagesAeromodellingzain ansariNo ratings yet
- Bolanos Jessica Assign8 BrochureDocument2 pagesBolanos Jessica Assign8 Brochureapi-272728466No ratings yet
- MR and Ms Chmsu GuidelinesDocument2 pagesMR and Ms Chmsu Guidelinessiari ann iliganNo ratings yet
- Criteria For Judging For Production NoDocument6 pagesCriteria For Judging For Production NoReysa m.duatinNo ratings yet
- Activity Report Pulot Kalat-Cdss TudloDocument3 pagesActivity Report Pulot Kalat-Cdss Tudlojestoni langgidoNo ratings yet
- A Narrative Report On StudentDocument13 pagesA Narrative Report On StudentLittleagle100% (2)
- Cacao LeavesDocument3 pagesCacao LeavesMarlyn MabalotNo ratings yet
- Miss Normi 2018: Concept: Philippine FestivalDocument4 pagesMiss Normi 2018: Concept: Philippine FestivalBrian Reyes Gangca100% (1)
- Resolution 2001-006 - Impeachment ProceduresDocument8 pagesResolution 2001-006 - Impeachment ProceduresRohj MarianoNo ratings yet
- 21 Bioprospecting Pros and ConsDocument5 pages21 Bioprospecting Pros and ConsShruti PillaiNo ratings yet
- DELAYED CHROMOS-WPS OfficeDocument31 pagesDELAYED CHROMOS-WPS OfficeMarlon M. AustriaNo ratings yet
- Digital Poster Making ContestDocument1 pageDigital Poster Making ContestJudy Ann FaustinoNo ratings yet
- Judging Sheet For The Spoken Word PoetryDocument1 pageJudging Sheet For The Spoken Word PoetryJohnny C. Abad Jr.No ratings yet
- Capstone Project: Group Name 2 Section Research Title Task DescriptionDocument7 pagesCapstone Project: Group Name 2 Section Research Title Task DescriptionSinead MolinosNo ratings yet
- Cultural Activities: Vocal Solo and Duet Competitions GuidelinesDocument3 pagesCultural Activities: Vocal Solo and Duet Competitions GuidelinesChristine May Sevilleno100% (1)
- NSTP Action PlanDocument2 pagesNSTP Action PlanJee En Bee100% (1)
- Sanitation SOPDocument4 pagesSanitation SOPMICHAEL JIMENONo ratings yet
- Literature ReviewDocument19 pagesLiterature ReviewNasrul Safwan MTNo ratings yet
- CHED Full Blown Proposal RPAG Form TEMPLATE Sep.2021Document14 pagesCHED Full Blown Proposal RPAG Form TEMPLATE Sep.2021Dix TyNo ratings yet
- Cytoskeleton and Cell MotilityDocument47 pagesCytoskeleton and Cell MotilityDyang AprilianiNo ratings yet
- RRL e ColiDocument4 pagesRRL e ColiCristina Pangan100% (1)
- During Fiestas and Festivals in BatangasDocument2 pagesDuring Fiestas and Festivals in BatangasHaroldene BuctolanNo ratings yet
- Chapter-1-3 (Proposal Defense)Document16 pagesChapter-1-3 (Proposal Defense)Jorico Marison EspirituNo ratings yet
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDocument1 pageProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahNo ratings yet
- Room Watcher Personal Data SheetDocument3 pagesRoom Watcher Personal Data SheetGiovanni NaagNo ratings yet
- MR and MS EBN 2023 Criteria For JudgingDocument3 pagesMR and MS EBN 2023 Criteria For JudgingPrincess Mae BalabaNo ratings yet
- Intramurals 2022 Question and Answer (Male Category) : Search For MR & Miss Intramurals PersonalityDocument4 pagesIntramurals 2022 Question and Answer (Male Category) : Search For MR & Miss Intramurals PersonalityShiera Saletrero SimbajonNo ratings yet
- Aquatic Plants: Structure and FunctionsDocument18 pagesAquatic Plants: Structure and FunctionsJai CataluñaNo ratings yet
- Metabolized: Nourishing The Filipino Youth Towards National Well Being" Eco Rampa 2019Document1 pageMetabolized: Nourishing The Filipino Youth Towards National Well Being" Eco Rampa 2019Gladz GladzNo ratings yet
- Chapter 7 - Factors Affects Folk DancingDocument11 pagesChapter 7 - Factors Affects Folk DancingLeonardo IV RamosNo ratings yet
- Module 4 - Rules and Regulations Governing Meat Inspection in The PhilippinesDocument11 pagesModule 4 - Rules and Regulations Governing Meat Inspection in The PhilippinesVincent Felix A. HernandezNo ratings yet
- Tiktok Dance Challenge 1Document1 pageTiktok Dance Challenge 1DAVE ANDREW AMOSCO100% (1)
- Atluna-Midterm Exam Transformative EducationDocument2 pagesAtluna-Midterm Exam Transformative EducationarianNo ratings yet
- Fiesta Sa NayonDocument1 pageFiesta Sa NayonAngel Margaret MayolNo ratings yet
- Degradation of Polyethylene By: Trichoderma HarzianumDocument20 pagesDegradation of Polyethylene By: Trichoderma HarzianumSophia Erika LargoNo ratings yet
- PUP OUS Application For Cross Enrollment 2017Document1 pagePUP OUS Application For Cross Enrollment 2017Aces Salvador SocitoNo ratings yet
- Automatic Waste Segregation and Monitoring SystemDocument7 pagesAutomatic Waste Segregation and Monitoring SystemGopu Mayyala100% (1)
- Bench Cheering MechanicsDocument1 pageBench Cheering MechanicsMaybelle AggabaoNo ratings yet
- MR and Ms-Talent MechanicsDocument5 pagesMR and Ms-Talent MechanicsJoebert DilagNo ratings yet
- Pathogens of Insects and Vertebrate PestsDocument10 pagesPathogens of Insects and Vertebrate PestsRozele RomNo ratings yet
- National Artists of The PhilippinesDocument9 pagesNational Artists of The PhilippinesHazel GumaponNo ratings yet
- Mat CHAPTER II 1 4 STSDocument16 pagesMat CHAPTER II 1 4 STSMarie DetarroNo ratings yet
- Weaving The Threads of Filipino HeritageDocument4 pagesWeaving The Threads of Filipino HeritagesryeyhbsdfvNo ratings yet
- Table Set Up Table Skirting Floral ArrangementDocument1 pageTable Set Up Table Skirting Floral ArrangementEbberussd BansuanNo ratings yet
- Term Paper DC MotorsDocument14 pagesTerm Paper DC MotorsVivekPrakash100% (1)
- Citizen's Charter - VSU Garden Beach ResortDocument3 pagesCitizen's Charter - VSU Garden Beach ResortvisayasstateuNo ratings yet
- Draft PSG For The Bachelor of Science in Civil Engineering BSCE Effective AY 2018 2019Document22 pagesDraft PSG For The Bachelor of Science in Civil Engineering BSCE Effective AY 2018 2019Mico CruzadoNo ratings yet
- 2023 2024 Sci117 Microbiology and Parasitology Course SyllabusDocument15 pages2023 2024 Sci117 Microbiology and Parasitology Course Syllabusmaevycrook09No ratings yet
- Dance Sport Mechanics 2016Document1 pageDance Sport Mechanics 2016XYRA KRISTI TORREVILLASNo ratings yet
- Pe Environmental HazardsDocument33 pagesPe Environmental HazardsMatthew PradoNo ratings yet
- Sepak Takraw GuidelinesDocument3 pagesSepak Takraw GuidelinesJustin Bidz IndiolaNo ratings yet
- Streetdancing ContestDocument3 pagesStreetdancing ContestBonlouie BacalsoNo ratings yet
- Campus Ministry Office GuidelinesDocument6 pagesCampus Ministry Office GuidelinesChristian De Guzman100% (1)
- Criteria For Judging EskuylahanDocument5 pagesCriteria For Judging EskuylahanKRISTINE CHAD NAVALES CANTALEJONo ratings yet
- Entrepreneurship and Business Planning PDFDocument5 pagesEntrepreneurship and Business Planning PDFGracey MorgaNo ratings yet
- PROJECT PROPOSAL HPTA ProjectDocument7 pagesPROJECT PROPOSAL HPTA ProjectSALGIE SERNALNo ratings yet
- Student Council Officers Qualifications and DutiesDocument2 pagesStudent Council Officers Qualifications and DutiesnhfdbhddhsdeyterhguyNo ratings yet
- Subcutaneous Mycoses: Presenter: DR Pranay Reddy Moderator: DR Tonita MNDocument81 pagesSubcutaneous Mycoses: Presenter: DR Pranay Reddy Moderator: DR Tonita MNSandipNo ratings yet
- What Is Subcutaneous MycosesDocument4 pagesWhat Is Subcutaneous MycosesArslan SaeedNo ratings yet
- Movie Time Group 3Document2 pagesMovie Time Group 3Einstein ObladesNo ratings yet
- Paraphilia: and The Sexual SelfDocument20 pagesParaphilia: and The Sexual SelfEinstein ObladesNo ratings yet
- Myco Viro Systemic MycosesDocument6 pagesMyco Viro Systemic MycosesEinstein ObladesNo ratings yet
- Superficial Mycoses 1Document5 pagesSuperficial Mycoses 1Einstein ObladesNo ratings yet
- KW 18KWH Canada Interim Letters - KWUSDocument2 pagesKW 18KWH Canada Interim Letters - KWUSMecano PadNo ratings yet
- Sample Question Paper - 3: Class - XDocument17 pagesSample Question Paper - 3: Class - XRehan AlamNo ratings yet
- Proof of An External WorldDocument3 pagesProof of An External WorldFarri93No ratings yet
- Plural of NounsDocument1 pagePlural of NounsCarmen TeixeiraNo ratings yet
- Oh S Risk RegisterDocument83 pagesOh S Risk RegisterJacob YeboaNo ratings yet
- Modeling of Batch Fermentation Kinetics For Succinic Acid Production by Mannheneimia SucciniciproducensDocument9 pagesModeling of Batch Fermentation Kinetics For Succinic Acid Production by Mannheneimia SucciniciproducensRyuuara Az-ZahraNo ratings yet
- Mens TshirtDocument15 pagesMens TshirtTrung Hieu NguyenNo ratings yet
- Precos Souza CruzDocument12 pagesPrecos Souza CruzPablo ToazzaNo ratings yet
- Cob-Ch11 EvolutionDocument36 pagesCob-Ch11 EvolutiongaryNo ratings yet
- Cost CurvesDocument2 pagesCost CurvesSumit Ray100% (1)
- PPC Researched PointersDocument4 pagesPPC Researched PointershitmonNo ratings yet
- ACT Math Formulas To MemorizeDocument1 pageACT Math Formulas To MemorizeRack OsMaNo ratings yet
- SprinklersDocument2 pagesSprinklersMohamed El MorsyNo ratings yet
- Ar Prda 2018 - FinalDocument37 pagesAr Prda 2018 - FinalucokNo ratings yet
- Liston The Lure of Learning in TeachingDocument28 pagesListon The Lure of Learning in TeachingDaniel NunnehNo ratings yet
- Consumer Electronics Servicing Learning Module 130610203451 Phpapp02Document145 pagesConsumer Electronics Servicing Learning Module 130610203451 Phpapp02Maureen Pusing80% (10)
- 2010 Reclamation Criteria For Wellsites and Associated Facilities For Forested LandsDocument95 pages2010 Reclamation Criteria For Wellsites and Associated Facilities For Forested Landskartikeyab111No ratings yet
- Egg Drop NotesDocument2 pagesEgg Drop Notesapi-365288705No ratings yet
- 978 1 5275 0785 2 SampleDocument30 pages978 1 5275 0785 2 SampleJacob AlonzoNo ratings yet
- Fleming's Left Hand Rule (ForDocument8 pagesFleming's Left Hand Rule (Forb_geyl4286No ratings yet
- 2020 79th PNWIMC Annual Conference AnnouncementDocument2 pages2020 79th PNWIMC Annual Conference AnnouncementnwberryfoundationNo ratings yet
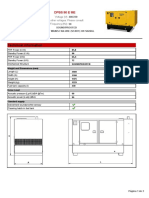
- Technical Information: Dpbs 90 E MeDocument3 pagesTechnical Information: Dpbs 90 E MeЛулу ТраедNo ratings yet
- Materi2012.1pre Print - Part1Document174 pagesMateri2012.1pre Print - Part1Hari TulusNo ratings yet
- Remedies For VenusDocument2 pagesRemedies For VenusAnonymous 4Iu6iiNo ratings yet
- Why Jesus Is Worthy of WorshipDocument7 pagesWhy Jesus Is Worthy of Worshiprukmani27No ratings yet
- Nickel Alloy Inconel 718 Properties and Applications by United Performance MetalsDocument4 pagesNickel Alloy Inconel 718 Properties and Applications by United Performance MetalsShubham SharmaNo ratings yet