Download as pdf or txt
You might also like
- Mastering Your Fears and Phobias - Workbook, Second Edition (Treatments That Work) (PDFDrive)Document199 pagesMastering Your Fears and Phobias - Workbook, Second Edition (Treatments That Work) (PDFDrive)Tiffany Lawrence100% (2)
- Dentalphobia PDFDocument3 pagesDentalphobia PDFAnonymous 9KcGpv100% (1)
- HealingToothDecay PDFDocument6 pagesHealingToothDecay PDFBj Long100% (1)
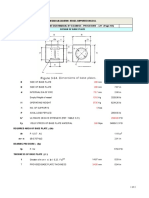
- Leg Support Calculation PDFDocument2 pagesLeg Support Calculation PDFSanjay MoreNo ratings yet
- Chapter 6 Work, Energy and PowerDocument12 pagesChapter 6 Work, Energy and PowerZhu Jiankun100% (1)
- Yamaha CLP 170 Service ManualDocument122 pagesYamaha CLP 170 Service ManualicaroheartNo ratings yet
- An Overview of Dental Anxiety and The Non-Pharmacological Management of Dental AnxietyDocument4 pagesAn Overview of Dental Anxiety and The Non-Pharmacological Management of Dental AnxietyMishellKarelisMorochoSegarraNo ratings yet
- Dental Fear and Anxiety: Information For Dental PractitionersDocument4 pagesDental Fear and Anxiety: Information For Dental PractitionersDinaNo ratings yet
- Argument SynthesisDocument7 pagesArgument Synthesisapi-309603847No ratings yet
- LD ModDocument62 pagesLD ModGayathri MenonNo ratings yet
- Dental FearsDocument10 pagesDental Fearshantimurova.nNo ratings yet
- Armfield Et Al-2013-Australian Dental JournalDocument18 pagesArmfield Et Al-2013-Australian Dental JournalAbhishek Isaac MathewNo ratings yet
- PhobiaDocument3 pagesPhobiaMana MegamNo ratings yet
- Pamphlet - 2Document1 pagePamphlet - 2Van AnhNo ratings yet
- Appu Kutt AnDocument16 pagesAppu Kutt AnAmalia ArumsariNo ratings yet
- Seligman 2017Document16 pagesSeligman 2017Sung Soon ChangNo ratings yet
- HipnozaDocument4 pagesHipnozaCetina AdelinNo ratings yet
- Dental FearDocument8 pagesDental FearShrishtiChokhaniNo ratings yet
- Evaluating Factors Associated With Fear And.7Document6 pagesEvaluating Factors Associated With Fear And.7Yusmiranda 06No ratings yet
- Appukuttan2016 PDFDocument16 pagesAppukuttan2016 PDFOscar Andres De LeonNo ratings yet
- Ansiedad Dental 2020Document11 pagesAnsiedad Dental 2020Francisca Abarca CifuentesNo ratings yet
- Dental PhobiaDocument9 pagesDental PhobiaMiztaloges86No ratings yet
- What Are You Afraid ofDocument3 pagesWhat Are You Afraid ofmohaddisaNo ratings yet
- 1.behavioral ManagementDocument20 pages1.behavioral Managementrudaf hanifNo ratings yet
- Psychology of PhobiasDocument13 pagesPsychology of PhobiasMalakNo ratings yet
- Englishpro 1Document10 pagesEnglishpro 1Santosh NiwaneNo ratings yet
- A Fear of PainDocument2 pagesA Fear of PainBabac Compass PashazadehNo ratings yet
- PsicologiaDocument24 pagesPsicologiaPablo UlisesNo ratings yet
- Dental Anxiety PDFDocument12 pagesDental Anxiety PDFKhalydia NafishaNo ratings yet
- Dental Anxiety - FullDocument14 pagesDental Anxiety - FullTJPRC PublicationsNo ratings yet
- Anxiety DisordersDocument16 pagesAnxiety Disordersapi-252217375No ratings yet
- 2019 Vanhee - Stimuli Involved in Dental Anxiety What Are Patients Afraid of A DescriptiveDocument10 pages2019 Vanhee - Stimuli Involved in Dental Anxiety What Are Patients Afraid of A Descriptivefabian.balazs.93No ratings yet
- Case Example: Obsessive-Compulsive DisorderDocument2 pagesCase Example: Obsessive-Compulsive DisorderLester MoeNo ratings yet
- Dental Fear/Anxiety: Managing Anxious or Fearful PatientsDocument3 pagesDental Fear/Anxiety: Managing Anxious or Fearful PatientsSung Soon ChangNo ratings yet
- I at Ro SedationDocument2 pagesI at Ro SedationAnchi JenNo ratings yet
- PharmaDocument1 pagePharmaAtinyaseelNo ratings yet
- Tapping for Dental Fear and Anxiety: Simple Steps to Clear the Fear and Love Your Dentist AgainFrom EverandTapping for Dental Fear and Anxiety: Simple Steps to Clear the Fear and Love Your Dentist AgainNo ratings yet
- 301 Notes For Unit-4Document7 pages301 Notes For Unit-4kulkarni.himani19940809No ratings yet
- Management of Dental Anxiety in Patients With Hearing ImpairmentDocument3 pagesManagement of Dental Anxiety in Patients With Hearing Impairmentveaceslav drobotNo ratings yet
- Anxiety and Dental ManagementDocument5 pagesAnxiety and Dental ManagementD DongNo ratings yet
- Does Your Child Have An Ear InfectionDocument1 pageDoes Your Child Have An Ear InfectionachmadtabaNo ratings yet
- (Download PDF) Sedation E Book A Guide To Patient Management 5Th Edition PDF Full Chapter PDFDocument38 pages(Download PDF) Sedation E Book A Guide To Patient Management 5Th Edition PDF Full Chapter PDFsmokieancica100% (8)
- Anxiety Disorder by SlidesgoDocument25 pagesAnxiety Disorder by SlidesgoTammar Haithem MustafaNo ratings yet
- American Journal of Clinical HypnosisDocument8 pagesAmerican Journal of Clinical Hypnosisbrice lemaireNo ratings yet
- Dental Fear in Patients Pursuing Orthodontic Treatment: Original ArticleDocument6 pagesDental Fear in Patients Pursuing Orthodontic Treatment: Original Articlemudassir rehmanNo ratings yet
- Question 1-What Is Phobia?: Day 7 Assignment Give Brief Answers of Below Given QuestionsDocument3 pagesQuestion 1-What Is Phobia?: Day 7 Assignment Give Brief Answers of Below Given QuestionsashwinNo ratings yet
- Delirium: A Guide For Patients, Family Members, and CaregiversDocument2 pagesDelirium: A Guide For Patients, Family Members, and Caregiversramzan aliNo ratings yet
- Aminabadi 2017Document25 pagesAminabadi 2017fghdhmdkhNo ratings yet
- Dental Fear/anxiety Among Children and Adolescents. A Systematic ReviewDocument10 pagesDental Fear/anxiety Among Children and Adolescents. A Systematic ReviewfghdhmdkhNo ratings yet
- Research Paper PhobiasDocument4 pagesResearch Paper Phobiasglavagwhf100% (1)
- Management of Fear & Anxiety - A Review 2013Document19 pagesManagement of Fear & Anxiety - A Review 2013AnimeAngelNo ratings yet
- Anxiety, Stress, & Coping: An International JournalDocument15 pagesAnxiety, Stress, & Coping: An International JournalSung Soon ChangNo ratings yet
- Dental Fear, Anxiety and Phobia (Final1)Document55 pagesDental Fear, Anxiety and Phobia (Final1)Aj VishwadheebNo ratings yet
- Dent Update 2015 42 373-382Document7 pagesDent Update 2015 42 373-382danissaNo ratings yet
- Pediatric Bruxism: From Etiology To Treatment: A ReviewDocument4 pagesPediatric Bruxism: From Etiology To Treatment: A ReviewApurava SinghNo ratings yet
- Panic Disorder PhobiasDocument9 pagesPanic Disorder Phobiasapi-3797941No ratings yet
- Treatment Options For The Specific Phobias: IjbcpDocument6 pagesTreatment Options For The Specific Phobias: IjbcpMarius MoroianuNo ratings yet
- How To End Phobias Anxiety and Panic 3rd EdDocument41 pagesHow To End Phobias Anxiety and Panic 3rd EdHung TranNo ratings yet
- Internacional Dentistry 2009Document8 pagesInternacional Dentistry 2009Sung Soon ChangNo ratings yet
- Conquering Dental Fear: Strategies for Overcoming Anxiety at the Dentist: All About DentistryFrom EverandConquering Dental Fear: Strategies for Overcoming Anxiety at the Dentist: All About DentistryNo ratings yet
- Anxiety Disorder by SlidesgoDocument55 pagesAnxiety Disorder by SlidesgoIra GustinaNo ratings yet
- Anxiety Disorder by SlidesgoDocument55 pagesAnxiety Disorder by SlidesgoTuesi Fredella AvissaNo ratings yet
- Form 67 Delivery Unloading and Loading of Materials and PlantDocument6 pagesForm 67 Delivery Unloading and Loading of Materials and PlantMohamed MedhioubNo ratings yet
- En Mongolia 06Document39 pagesEn Mongolia 06Sandeep DasNo ratings yet
- Water Stability - What Does It Mean and How Do You Measure It ?Document9 pagesWater Stability - What Does It Mean and How Do You Measure It ?Richard EscueNo ratings yet
- Macro Chapter 7Document12 pagesMacro Chapter 7Mary Jane PelaezNo ratings yet
- Ikimono Gakari - HOT MILKDocument3 pagesIkimono Gakari - HOT MILKapi-3799292100% (1)
- CR Unit 1 &11 (Part A &B)Document12 pagesCR Unit 1 &11 (Part A &B)durai muruganNo ratings yet
- Textbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFDocument39 pagesTextbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFjanet.galloway812100% (8)
- 12 2f17 Vegetarian Argumentative EssayDocument7 pages12 2f17 Vegetarian Argumentative Essayapi-413258549No ratings yet
- Tutorial-2 - Heterocycles Nomenclature-Part-IIDocument18 pagesTutorial-2 - Heterocycles Nomenclature-Part-IIamirNo ratings yet
- Is-Cal01 Design Carbon Accounting On Site Rev.02Document6 pagesIs-Cal01 Design Carbon Accounting On Site Rev.02shoba9945No ratings yet
- Background of Philippine Art and Literature in Romantic RealismDocument2 pagesBackground of Philippine Art and Literature in Romantic RealismRaldz CoyocaNo ratings yet
- Premium HC: 120 Halfcell Monocrystalline High Performance Solar ModuleDocument2 pagesPremium HC: 120 Halfcell Monocrystalline High Performance Solar ModuleMujahed Al-HamatiNo ratings yet
- Low Noise Amplifier Basics: by V. M. García-ChocanoDocument4 pagesLow Noise Amplifier Basics: by V. M. García-ChocanoPranjal Jalan100% (1)
- Combustion Engineering, Heat Transfer, Refrigeration Engineering, & Air ConditioningDocument17 pagesCombustion Engineering, Heat Transfer, Refrigeration Engineering, & Air ConditioningNicole Mae AllosadaNo ratings yet
- Autonomous University of Baja California: Faculty of Engineering Aerospace EngineeringDocument18 pagesAutonomous University of Baja California: Faculty of Engineering Aerospace EngineeringOscar Oreste Salvador CarlosNo ratings yet
- Free Download All Aeronautical Engg Books: AERO 3-1 BOOKSDocument11 pagesFree Download All Aeronautical Engg Books: AERO 3-1 BOOKSMacen SnoodleNo ratings yet
- 10 Science TP 11 1Document5 pages10 Science TP 11 1Ananaya BansalNo ratings yet
- KONAN Emmanuel Sales Technical Engineer 16 Juin 23Document1 pageKONAN Emmanuel Sales Technical Engineer 16 Juin 23EMMANUEL KONANNo ratings yet
- Quatre Agro Enterprise Private LimitedDocument25 pagesQuatre Agro Enterprise Private Limitedp23pallavNo ratings yet
- Regulator InfoDocument6 pagesRegulator InfoAguilar AlexNo ratings yet
- AbseilingDocument12 pagesAbseilingMurah Rezeki Cikgu WafiNo ratings yet
- Tax System SriLankaDocument44 pagesTax System SriLankamandarak7146No ratings yet
- English Final Test Grade XiiDocument9 pagesEnglish Final Test Grade XiiLiza RahmawatiNo ratings yet
- ISA - Study Guide Table of ContentsDocument3 pagesISA - Study Guide Table of Contentsasdf123asdfasdfNo ratings yet
- Straumann Product Catalogue 2018 2019Document260 pagesStraumann Product Catalogue 2018 2019kllasikalleNo ratings yet
- ASTM GradesDocument4 pagesASTM GradesSaurabh MundheNo ratings yet
- Electronics Cooling: Mechanical Power Engineering DeptDocument22 pagesElectronics Cooling: Mechanical Power Engineering DeptneilNo ratings yet