Download as docx, pdf, or txt
You might also like
- Pharmaceutical Jurisprudence ManualDocument12 pagesPharmaceutical Jurisprudence ManualSlark SlarkNo ratings yet
- Introduction To PharmacotherapeuticsDocument14 pagesIntroduction To Pharmacotherapeuticskyra alondayNo ratings yet
- Preclinical Research PDFDocument4 pagesPreclinical Research PDFEleyra Llanos Parra100% (1)
- Chapter 3. One-Compartment Open Model Intravenous Bolus AdministrationDocument23 pagesChapter 3. One-Compartment Open Model Intravenous Bolus AdministrationbencleeseNo ratings yet
- QSAR and Drug Design: New Developments and ApplicationsFrom EverandQSAR and Drug Design: New Developments and ApplicationsRating: 5 out of 5 stars5/5 (1)
- Pharmacists Role Clinical Pharmacokinetic MonitoringDocument2 pagesPharmacists Role Clinical Pharmacokinetic MonitoringauliaNo ratings yet
- Biopharmaceutics and PharmacokineticDocument4 pagesBiopharmaceutics and PharmacokineticRiyaz AliNo ratings yet
- Mathematical Fundamental in PharmacokineticDocument21 pagesMathematical Fundamental in PharmacokineticErna PratiwiNo ratings yet
- Introduction To BiopharmaceuticsDocument27 pagesIntroduction To BiopharmaceuticsAmina Akther Mim 1821179649No ratings yet
- Biopharmaceutics: GSDMSFI - BS Pharmacy 3Document11 pagesBiopharmaceutics: GSDMSFI - BS Pharmacy 3Majeddah Aliudin TalambunganNo ratings yet
- Jurnal TSF 1 - Pharmacopoeial Standards and Specifications For PDFDocument12 pagesJurnal TSF 1 - Pharmacopoeial Standards and Specifications For PDFAngelia Nuuril FahmiNo ratings yet
- Autonomic Nervous SystemDocument36 pagesAutonomic Nervous SystemGrace NdutaNo ratings yet
- Amity Institute of Pharmacy-NddsDocument5 pagesAmity Institute of Pharmacy-NddsTanujaNo ratings yet
- BioequivalenceDocument30 pagesBioequivalenceTejas PatelNo ratings yet
- Clinical PharmacyDocument15 pagesClinical PharmacyKate EvangelistaNo ratings yet
- BiopharmaceuticsDocument13 pagesBiopharmaceuticsAngeli Marie PadillaNo ratings yet
- Practice Question Paper BPPKDocument1 pagePractice Question Paper BPPKAyush SrinivasanNo ratings yet
- Practical Lab ManualDocument15 pagesPractical Lab ManualMahesh Chougule50% (2)
- BPharma-6Sem-DrRishiPaliwal-Biopharmaceutics & PharmacokineticsDocument23 pagesBPharma-6Sem-DrRishiPaliwal-Biopharmaceutics & Pharmacokineticsירדן לויןNo ratings yet
- Drug EliminationDocument10 pagesDrug EliminationFabulously ShooktNo ratings yet
- BASIC PHARMACOKINETICS - CHAPTER 13: Non-Linear KineticsDocument22 pagesBASIC PHARMACOKINETICS - CHAPTER 13: Non-Linear KineticsDrHeba100% (7)
- Semisolid Dosage Forms Manufacturing Tools, Critical Process Parameters, Strategies, Optimization and Recent AdvancesDocument11 pagesSemisolid Dosage Forms Manufacturing Tools, Critical Process Parameters, Strategies, Optimization and Recent AdvancesNantiSartikaNo ratings yet
- Paracetamol Tablets by Direct CompresisonDocument3 pagesParacetamol Tablets by Direct CompresisonShivraj JadhavNo ratings yet
- Forensic Pharmacy and Forensic PharmacistDocument17 pagesForensic Pharmacy and Forensic PharmacistHajra Mehar100% (1)
- GRDDSDocument31 pagesGRDDSMuhammad Azam TahirNo ratings yet
- Pharmacy PracticeDocument17 pagesPharmacy PracticeP D SpencerNo ratings yet
- Therapeutic Drug MonitoringDocument14 pagesTherapeutic Drug MonitoringChristian DavidNo ratings yet
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Community PharmacyDocument8 pagesCommunity PharmacyAmit KumarNo ratings yet
- CPR SummaryDocument2 pagesCPR SummaryaqsamerajNo ratings yet
- Dissolution Profile ComparisonDocument17 pagesDissolution Profile Comparisondipti_srivNo ratings yet
- Statement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistDocument5 pagesStatement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistAprilia R. Permatasari0% (1)
- 905 Uniformity of Dosage UnitsDocument10 pages905 Uniformity of Dosage UnitsIcee SinlapasertNo ratings yet
- BASIC PHARMACOKINETICS - CHAPTER 1: IntroductionDocument34 pagesBASIC PHARMACOKINETICS - CHAPTER 1: IntroductionDrHeba100% (2)
- Clinical Pharmacy Introduction and ScopeDocument22 pagesClinical Pharmacy Introduction and ScopeSufyan MirzaNo ratings yet
- Ward RoundDocument2 pagesWard RoundAnonymous whcvnPBeQNo ratings yet
- Excretion of Drugs: Dr. G.SAILAJA, M.Pharm - PH.D., Assoc. Professor, Dept. of PharmaceuticsDocument43 pagesExcretion of Drugs: Dr. G.SAILAJA, M.Pharm - PH.D., Assoc. Professor, Dept. of PharmaceuticsSailaja Reddy GunnamNo ratings yet
- Altered Pharmacokinetics in Liver DiseasesDocument30 pagesAltered Pharmacokinetics in Liver DiseasesNailaAns100% (1)
- Clinical Pharmacy PHR 405: Chapter 1: General ConsiderationsDocument24 pagesClinical Pharmacy PHR 405: Chapter 1: General ConsiderationsSamiul Alam Rajib100% (1)
- Pharmacology: Pharmacokinetic & Dose: Ana Khusnul Faizah Farmasi FK Uht 2018Document27 pagesPharmacology: Pharmacokinetic & Dose: Ana Khusnul Faizah Farmasi FK Uht 2018Aulia rahmawatiNo ratings yet
- Assignment I SolubilityDocument24 pagesAssignment I Solubilityabthapa100% (1)
- Bio PharmaceuticsDocument48 pagesBio PharmaceuticsRajan Kashyap100% (2)
- Principles of PharmacoeconomicsDocument12 pagesPrinciples of PharmacoeconomicsNida Ali100% (1)
- Pharmaceutical Care in Multiple EnvironmentsDocument7 pagesPharmaceutical Care in Multiple EnvironmentsMansoor KhanNo ratings yet
- Controlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesDocument17 pagesControlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesintanNo ratings yet
- Introduction To PharmacotherapeuticsDocument49 pagesIntroduction To PharmacotherapeuticsChandraprakash JadhavNo ratings yet
- AP ECET Pharmacy Stream Syllabus and Exam PatternDocument15 pagesAP ECET Pharmacy Stream Syllabus and Exam PatternpavaniNo ratings yet
- Pharmaceutics Chapter 7 Novel Drug Delivery System NotesDocument10 pagesPharmaceutics Chapter 7 Novel Drug Delivery System NotesBhuvnesh ChandraNo ratings yet
- Worker's Care Monitored Receives Instructions.: PH-PHR 212 Dispensing 1 - LECDocument7 pagesWorker's Care Monitored Receives Instructions.: PH-PHR 212 Dispensing 1 - LECSeania BuenaventuraNo ratings yet
- 2013 Introduction of Clinical PharmacyDocument18 pages2013 Introduction of Clinical Pharmacyyudi100% (1)
- Bioavailability and BioequivalenceDocument56 pagesBioavailability and Bioequivalenceنور الهدى100% (1)
- Slide 9 Patient Counseling and Other Special Considerations in CounselingDocument22 pagesSlide 9 Patient Counseling and Other Special Considerations in CounselingJean GanubNo ratings yet
- Pharmaco KineticsDocument38 pagesPharmaco KineticsAnonymous 3xcMImL4No ratings yet
- Solid Dosage FormsDocument4 pagesSolid Dosage Formscofodike1No ratings yet
- Sandra Bai CVDocument3 pagesSandra Bai CVSandra BaiNo ratings yet
- BP 181212054815Document74 pagesBP 181212054815Ahmad AinurofiqNo ratings yet
- Hepatic ClearanceDocument14 pagesHepatic ClearanceMohamed MarzoukNo ratings yet
- Pharmaceutical CareDocument27 pagesPharmaceutical Caremai elewaNo ratings yet
- Pharmacokinetic ParametersDocument29 pagesPharmacokinetic Parametersfaisalnadeem100% (1)
- Public Communication: Click To Edit Master Title StyleDocument9 pagesPublic Communication: Click To Edit Master Title Styleheyyo ggNo ratings yet
- Lipids Reviewer MidtermDocument14 pagesLipids Reviewer Midtermheyyo ggNo ratings yet
- Or Al Interpretation: Applying Verbal and Non Verbal SymbolsDocument8 pagesOr Al Interpretation: Applying Verbal and Non Verbal Symbolsheyyo ggNo ratings yet
- What Are The Evaluation of Drugs? 11.3. Microscopical EvaluationDocument3 pagesWhat Are The Evaluation of Drugs? 11.3. Microscopical Evaluationheyyo ggNo ratings yet
- Exercise No. 3 Hospital FormularyDocument5 pagesExercise No. 3 Hospital Formularyheyyo ggNo ratings yet
- Gestures and Body MovementsDocument17 pagesGestures and Body Movementsheyyo ggNo ratings yet
- Troglitazone: Prepared By: Ariza, Zareen Angela V. Mejia, Vica Mae B. Solis, Allyssa Moira BDocument12 pagesTroglitazone: Prepared By: Ariza, Zareen Angela V. Mejia, Vica Mae B. Solis, Allyssa Moira Bheyyo ggNo ratings yet
- Hospi Lab ExpDocument6 pagesHospi Lab Expheyyo ggNo ratings yet
- CLINICAL TRIALS DDD Mid StartDocument7 pagesCLINICAL TRIALS DDD Mid Startheyyo ggNo ratings yet
- CADDDocument5 pagesCADDheyyo ggNo ratings yet
- TRANSFER OF TECHNOLOGY ManuDocument4 pagesTRANSFER OF TECHNOLOGY Manuheyyo ggNo ratings yet
- Interpretation: Red Blood Cell Count Is Lower Than NormalDocument3 pagesInterpretation: Red Blood Cell Count Is Lower Than Normalheyyo ggNo ratings yet
- ROFECOXIBDocument10 pagesROFECOXIBheyyo ggNo ratings yet
- Exercise No 2Document12 pagesExercise No 2heyyo ggNo ratings yet
- Clinical Trial PhasesDocument11 pagesClinical Trial Phasesheyyo ggNo ratings yet
- PHARMACOVIGILANCEDocument29 pagesPHARMACOVIGILANCEheyyo ggNo ratings yet
- Introduction To Pharmaceutical Dosage Forms, Drug Delivery Systems, and Medical DevicesDocument3 pagesIntroduction To Pharmaceutical Dosage Forms, Drug Delivery Systems, and Medical Devicesheyyo ggNo ratings yet
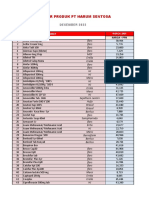
- Daftar Produk PT Harum Sentosa: NO Nama ObatDocument10 pagesDaftar Produk PT Harum Sentosa: NO Nama ObatLutfia LatifahNo ratings yet
- Sr. No: CategoryDocument42 pagesSr. No: CategoryMonti SainiNo ratings yet
- August 2022Document11 pagesAugust 2022mercene medicalNo ratings yet
- Corticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Document26 pagesCorticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Ghadi ElbarghathiNo ratings yet
- Dpo S. Jefri NewDocument4 pagesDpo S. Jefri Newseptian gunturNo ratings yet
- Benzodiazepine Drug BankDocument5 pagesBenzodiazepine Drug BankAbhishek MishraNo ratings yet
- Pharmacodynamics and Pharmacokinetics of The.29Document4 pagesPharmacodynamics and Pharmacokinetics of The.29Ama KireidesuNo ratings yet
- Holze 2023Document10 pagesHolze 2023Ramiro Manzano NúñezNo ratings yet
- OBAT INJEKSI AmyDocument4 pagesOBAT INJEKSI AmyKlinik MMCNo ratings yet
- Stock 15 April 2024Document6 pagesStock 15 April 2024Liana AnggraeniNo ratings yet
- LevetiracetamDocument4 pagesLevetiracetamGwyn RosalesNo ratings yet
- STOK8Document35 pagesSTOK8Adinda Nur AtifahNo ratings yet
- UntitledDocument244 pagesUntitledFARMACIA MASNo ratings yet
- CARVEDILOL Nursing ImplicationsDocument2 pagesCARVEDILOL Nursing Implicationsshiraz.aNo ratings yet
- FUNDA LEC Finals - Medication AdministrationDocument14 pagesFUNDA LEC Finals - Medication AdministrationNel joy PaurilloNo ratings yet
- Raws Price ListDocument2 pagesRaws Price ListVinicius100% (1)
- Bioavailability Protocol and Methods of AssessmentDocument20 pagesBioavailability Protocol and Methods of AssessmentKeerti RashmikaNo ratings yet
- Data Master OkDocument128 pagesData Master OkGudang farmasi Rs TandunNo ratings yet
- Form Obat Berdasarkan GolonganDocument39 pagesForm Obat Berdasarkan GolonganLulu AzizahNo ratings yet
- Lexicomp® Drug Interactions - UpToDateDocument2 pagesLexicomp® Drug Interactions - UpToDateDiana PhamNo ratings yet
- Angeles y Demonios (Benni Hinn)Document147 pagesAngeles y Demonios (Benni Hinn)Jonatan CabreraNo ratings yet
- Drug Study Valproate SodiumDocument4 pagesDrug Study Valproate SodiumLouie Danielle SegarraNo ratings yet
- Roedor Rodent - AnalgesiaDocument9 pagesRoedor Rodent - AnalgesiaMalu Verruck TortolaNo ratings yet
- Obat PsikiatriDocument1 pageObat Psikiatriice rumkoremNo ratings yet
- Table 25-4Document1 pageTable 25-4Dragutin PetrićNo ratings yet
- Daftar Nama Obat Yang Mengandung PrekursorDocument4 pagesDaftar Nama Obat Yang Mengandung PrekursorRadika Afiko PradestiNo ratings yet
- Parenteral Drugs: Compatibilit Y: Yosefa Asteria, S.Farm.,Apt Rs Suaka Insan BanjarmasinDocument42 pagesParenteral Drugs: Compatibilit Y: Yosefa Asteria, S.Farm.,Apt Rs Suaka Insan Banjarmasinfarida nur ainiNo ratings yet
- Queenie Rose Domingo - Drug Study (Silver Sulfadiazine)Document1 pageQueenie Rose Domingo - Drug Study (Silver Sulfadiazine)Sheryl Ann Barit PedinesNo ratings yet
- Stock 29.04.23Document5 pagesStock 29.04.23Kasi HumasNo ratings yet
- Antihipertenziva Alfa 2 MimeticiDocument10 pagesAntihipertenziva Alfa 2 MimeticiaksymarNo ratings yet