Download as docx, pdf, or txt
You might also like
- Labor Pain NCPDocument4 pagesLabor Pain NCPBea Dela Cena60% (5)
- Nursing Care Plan-AscitesDocument10 pagesNursing Care Plan-AscitesKayki Louise75% (4)
- Nurse'S Notes Name: - Cleopatra Andude - Age/Sex/CS: - 36/F/M - Ward/Room: - Obward-123 - ATTENDING PHYSICIAN - Dr. Danilo DizonDocument3 pagesNurse'S Notes Name: - Cleopatra Andude - Age/Sex/CS: - 36/F/M - Ward/Room: - Obward-123 - ATTENDING PHYSICIAN - Dr. Danilo DizonRenea Joy ArruejoNo ratings yet
- Orif Post Op NCPDocument1 pageOrif Post Op NCPKristine Young100% (1)
- Orif Post NCPDocument1 pageOrif Post NCPKristine Young100% (2)
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationRenea Joy ArruejoNo ratings yet
- Manguiat, Ncma 111 RomeoDocument4 pagesManguiat, Ncma 111 RomeoCiara ManguiatNo ratings yet
- NCP PostpartumDocument6 pagesNCP PostpartumLovely Anne ArqueroNo ratings yet
- NCP, DrugstudyDocument5 pagesNCP, DrugstudySheena LacasteNo ratings yet
- Assessment Nursing Diagnosis Analysis Planning Implementation Rationale EvaluationDocument1 pageAssessment Nursing Diagnosis Analysis Planning Implementation Rationale EvaluationAnne Beatriz SantiagoNo ratings yet
- NCP orDocument2 pagesNCP orAngel Caldeo BolidoNo ratings yet
- Nursing Care Plan For CellulitisDocument6 pagesNursing Care Plan For CellulitisChander Kanta100% (3)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument9 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationLillabinNo ratings yet
- Nursing Care Plan For CellulitisDocument6 pagesNursing Care Plan For CellulitisJenefer PanchoNo ratings yet
- "I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by TheDocument2 pages"I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by Theunnamed person100% (1)
- Nursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationSheril Sularte CasanesNo ratings yet
- Nursing Care Plan For Ischemic Stroke ProblemDocument2 pagesNursing Care Plan For Ischemic Stroke ProblemA HNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Desired Outcomes Subjective: "Napakasakit NG Mga Kasukasuhan Ko" As Verbalized by The PatientDocument5 pagesAssessment Diagnosis Planning Implementation Rationale Desired Outcomes Subjective: "Napakasakit NG Mga Kasukasuhan Ko" As Verbalized by The PatientAngelou Mortos100% (1)
- Nursing Care PlanDocument5 pagesNursing Care PlankingpinNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- NCP FamedDocument1 pageNCP FamedAbegail MierNo ratings yet
- Silliman University Dumaguete City: SY 2019-2020 College of NursingDocument3 pagesSilliman University Dumaguete City: SY 2019-2020 College of NursingRiza Angela BarazanNo ratings yet
- NCP DengueDocument3 pagesNCP DengueNecy Tessa C. AcostaNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation IndependentDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation IndependentYongNo ratings yet
- NCPDocument3 pagesNCPKrishcel Canlapan InsoNo ratings yet
- 2 NCPSDocument7 pages2 NCPSJamila Galindo TomasNo ratings yet
- Nursing Care Plan Cesarian DeliveryDocument2 pagesNursing Care Plan Cesarian Deliveryderic97% (39)
- Nursing Care Plan: University of San Jose-RecoletosDocument2 pagesNursing Care Plan: University of San Jose-RecoletosIvan A. EleginoNo ratings yet
- NCP Case AnalysisDocument3 pagesNCP Case AnalysisKyle DapulagNo ratings yet
- LCCSDocument2 pagesLCCSmaria_magno_6No ratings yet
- Nursing Care Plan ON The Effects of ChemotherapyDocument4 pagesNursing Care Plan ON The Effects of ChemotherapyCecil CacayNo ratings yet
- Nursing Care Plan ON The Effects of ChemotherapyDocument4 pagesNursing Care Plan ON The Effects of ChemotherapyCecil CacayNo ratings yet
- Nursing Care Plan ON The Effects of ChemotherapyDocument4 pagesNursing Care Plan ON The Effects of ChemotherapyCecil CacayNo ratings yet
- Nursing Care Plan ON The Effects of ChemotherapyDocument4 pagesNursing Care Plan ON The Effects of ChemotherapyCecil CacayNo ratings yet
- Nursing Care Plan ON The Effects of ChemotherapyDocument4 pagesNursing Care Plan ON The Effects of ChemotherapyCecil CacayNo ratings yet
- Pre-Operative (Incision & Drainage of Abscess)Document6 pagesPre-Operative (Incision & Drainage of Abscess)Eunice MañalacNo ratings yet
- Nursing ManagementDocument3 pagesNursing Managementjames quintoNo ratings yet
- NCP CSDocument4 pagesNCP CSJM UncianoNo ratings yet
- St. Paul University PhilippinesDocument3 pagesSt. Paul University PhilippinesMia Grace GarciaNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationAriaNo ratings yet
- Impaired Physical MobilityDocument2 pagesImpaired Physical MobilityNicole Genevie MallariNo ratings yet
- Cues Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Planning Intervention Rationale EvaluationBiancaGabatinoAbarcaNo ratings yet
- After Pain Related To Body Response To Infective Agent, Properties of InfectionDocument4 pagesAfter Pain Related To Body Response To Infective Agent, Properties of InfectionimnotmecoNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanIrish Paping TucyapaoNo ratings yet
- Observed Guarding Behavior in BedDocument3 pagesObserved Guarding Behavior in BedRose Alvarez ArajaNo ratings yet
- NCPDocument6 pagesNCPIrene Grace BalcuevaNo ratings yet
- NCP and PatophyDocument2 pagesNCP and PatophyRhea Anne NuñezNo ratings yet
- S: "Masakit Ang Ulo at Tiyan Niya" As Verbalized byDocument2 pagesS: "Masakit Ang Ulo at Tiyan Niya" As Verbalized bydenise-iceNo ratings yet
- Nursing Care PlansDocument4 pagesNursing Care Plansapi-19762967No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlankimtalaNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Independent: Short Term Goal OutcomeDocument9 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Independent: Short Term Goal OutcomeCindy MariscotesNo ratings yet
- NCP Skin IntegrityDocument3 pagesNCP Skin IntegrityAlfie Ayro50% (2)
- NCP For Surgical CasesDocument10 pagesNCP For Surgical Caseslouie roderosNo ratings yet
- ASSESSMENTDocument1 pageASSESSMENTBryant Riego IIINo ratings yet
- NCP During LaborDocument6 pagesNCP During LaborJamielyn BassigNo ratings yet
- Care PlansDocument7 pagesCare PlansFirenze Fil100% (6)
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- Medical Integration Model as it Pertains to Musculoskeletal ConditionsFrom EverandMedical Integration Model as it Pertains to Musculoskeletal ConditionsNo ratings yet
- Respiratory Failure: Presenter: Rafin, Marinel F. Ramos Marvin ODocument28 pagesRespiratory Failure: Presenter: Rafin, Marinel F. Ramos Marvin ORenea Joy ArruejoNo ratings yet
- Nurse'S Notes: Date-Shift Focus Data - Action - ResponseDocument5 pagesNurse'S Notes: Date-Shift Focus Data - Action - ResponseRenea Joy ArruejoNo ratings yet
- Covid 19 - PathophysiologyDocument3 pagesCovid 19 - PathophysiologyRenea Joy ArruejoNo ratings yet
- Doctor's Order Phase 2Document5 pagesDoctor's Order Phase 2Renea Joy ArruejoNo ratings yet
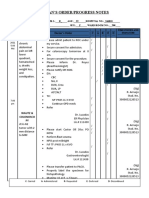
- Date Progress Notes Doctor's Order C AR E DDocument4 pagesDate Progress Notes Doctor's Order C AR E DRenea Joy ArruejoNo ratings yet
- WWW - Unp.edu - PH CP# 09177148749, 09175785986: University of Northern PhilippinesDocument1 pageWWW - Unp.edu - PH CP# 09177148749, 09175785986: University of Northern PhilippinesRenea Joy ArruejoNo ratings yet
- Thematic (Polgov) : The Importance of The Covid-19 VaccineDocument2 pagesThematic (Polgov) : The Importance of The Covid-19 VaccineRenea Joy ArruejoNo ratings yet
- Ostomy Care: Learning Manual DescriptionDocument12 pagesOstomy Care: Learning Manual DescriptionRenea Joy ArruejoNo ratings yet
- Module 2 Leadership MGTDocument14 pagesModule 2 Leadership MGTRenea Joy ArruejoNo ratings yet
- Module 1 - IS-PEFRDocument7 pagesModule 1 - IS-PEFRRenea Joy ArruejoNo ratings yet
- ET Intubation and SuctioningDocument15 pagesET Intubation and SuctioningRenea Joy ArruejoNo ratings yet
- Tracheostomy Care: Module DescriptionDocument9 pagesTracheostomy Care: Module DescriptionRenea Joy ArruejoNo ratings yet
- IV TXDocument9 pagesIV TXRenea Joy ArruejoNo ratings yet
- University of Northern Philippines: Northside Doctors Hospital (Ward3)Document3 pagesUniversity of Northern Philippines: Northside Doctors Hospital (Ward3)Renea Joy ArruejoNo ratings yet
- O2 TherapyDocument23 pagesO2 TherapyRenea Joy ArruejoNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanRenea Joy ArruejoNo ratings yet
- Hypertension & CardiomyopathyDocument18 pagesHypertension & CardiomyopathyRenea Joy ArruejoNo ratings yet
- Severe Acute Respiratory Syndrome Coronavirus 2 (Sars Cov 2Document16 pagesSevere Acute Respiratory Syndrome Coronavirus 2 (Sars Cov 2Renea Joy ArruejoNo ratings yet
- Pathophysiology of COVID-19.: Anant Parasher Postgrad Med J 2021 97:312-320Document1 pagePathophysiology of COVID-19.: Anant Parasher Postgrad Med J 2021 97:312-320Renea Joy ArruejoNo ratings yet
- Kardex: Time Started Time DUEDocument2 pagesKardex: Time Started Time DUERenea Joy ArruejoNo ratings yet
- Doctor'S Order Sheet: Time Posted AND SignatureDocument3 pagesDoctor'S Order Sheet: Time Posted AND SignatureRenea Joy ArruejoNo ratings yet
- Therapeutic Sheet: Name: C.A Age/Sex/CS:36/M Ward/Room:123 Date and Time GivenDocument3 pagesTherapeutic Sheet: Name: C.A Age/Sex/CS:36/M Ward/Room:123 Date and Time GivenRenea Joy ArruejoNo ratings yet
- Renea Joy Arruejo - Lecture ActivityDocument2 pagesRenea Joy Arruejo - Lecture ActivityRenea Joy ArruejoNo ratings yet
- Unp-Cn Do Not Reproduce: University of Northern PhilippinesDocument5 pagesUnp-Cn Do Not Reproduce: University of Northern PhilippinesRenea Joy ArruejoNo ratings yet
- Vital Signs Sheet: Date Time BP PR Temp RR O2 SAT Intake Output RemarksDocument5 pagesVital Signs Sheet: Date Time BP PR Temp RR O2 SAT Intake Output RemarksRenea Joy ArruejoNo ratings yet
- Patient's Chart - Parenteral SheetDocument3 pagesPatient's Chart - Parenteral SheetRenea Joy ArruejoNo ratings yet
- Unp-Cn Do Not Reproduce: Module DescriptionDocument5 pagesUnp-Cn Do Not Reproduce: Module DescriptionRenea Joy ArruejoNo ratings yet
- Inverted Nipple PaperDocument7 pagesInverted Nipple PaperFarisah Dewi Batari EmsilNo ratings yet
- kh7 CVPDocument50 pageskh7 CVPأبوأحمد الحكيمNo ratings yet
- AmraDocument6 pagesAmraShantu ShirurmathNo ratings yet
- Rom, Eprom, & Eeprom Technology: Figure 9-1. Read Only Memory SchematicDocument14 pagesRom, Eprom, & Eeprom Technology: Figure 9-1. Read Only Memory SchematicVu LeNo ratings yet
- ARC VisionDocument2 pagesARC VisionmelvincabeNo ratings yet
- Infectious Mononucleosis in Adults and Adolescents - UpToDateDocument26 pagesInfectious Mononucleosis in Adults and Adolescents - UpToDateEduardo Romero StéfaniNo ratings yet
- Chem 27.1 Experiment 5 Oxidation Reduction Titration IodimetryDocument3 pagesChem 27.1 Experiment 5 Oxidation Reduction Titration IodimetryNathaniel John JumalonNo ratings yet
- TPC-1071H - 1271H - 1571H - 1771H - User Manual - Ed3Document88 pagesTPC-1071H - 1271H - 1571H - 1771H - User Manual - Ed3DeniMestiWidiantoNo ratings yet
- Rodan and Fields Product GuideDocument17 pagesRodan and Fields Product GuideSusy MariaNo ratings yet
- Creativity and InnovationDocument25 pagesCreativity and InnovationHarshaNo ratings yet
- Final Exam Bee4113 Sem 1 201011Document8 pagesFinal Exam Bee4113 Sem 1 201011Kung ChinHan100% (1)
- Mobile SPM & DF 2020.ppt (Compatibility Mode)Document18 pagesMobile SPM & DF 2020.ppt (Compatibility Mode)Sambo BenerNo ratings yet
- MEO Class 1 ProjectDocument2 pagesMEO Class 1 ProjectAshish Ranjan0% (1)
- Endocrine System (Zoology)Document3 pagesEndocrine System (Zoology)Cheska de GuzmanNo ratings yet
- Tábua de Maré - Dezembro 2023Document1 pageTábua de Maré - Dezembro 2023gustavo alvesNo ratings yet
- 16 RMM Spring Edition 2020 Solutions CompressedDocument83 pages16 RMM Spring Edition 2020 Solutions CompressedKhokon GayenNo ratings yet
- Future - Brochure (ENG) 2022Document28 pagesFuture - Brochure (ENG) 2022Peso RcsoNo ratings yet
- S475Document33 pagesS475Barjam KafexhiuNo ratings yet
- Problems of Iron and Steel Industry in India:: Swot Analysis StrengthDocument4 pagesProblems of Iron and Steel Industry in India:: Swot Analysis StrengthAnonymous hmd3jXd4No ratings yet
- Net Paper With Solution June 2017 Chemical SciencesDocument40 pagesNet Paper With Solution June 2017 Chemical SciencesDeeksha KumariNo ratings yet
- Instruction Manual Pygmy Current Meter Model Oss-Pc1: Hyquest Solutions Pty LTDDocument17 pagesInstruction Manual Pygmy Current Meter Model Oss-Pc1: Hyquest Solutions Pty LTDTomás Londoño GarcíaNo ratings yet
- A 6 DoF Maneuvering Model For The Rapid Estimation of Hydrod - 2020 - Ocean EngiDocument22 pagesA 6 DoF Maneuvering Model For The Rapid Estimation of Hydrod - 2020 - Ocean EngijavierzmorNo ratings yet
- Bomba Neumatica Wilden T4Document27 pagesBomba Neumatica Wilden T4Jhon Edison Mazo JaramilloNo ratings yet
- Delegate List - 10th IMRC With Contact Details - Removed (1) - RemovedDocument234 pagesDelegate List - 10th IMRC With Contact Details - Removed (1) - RemovedSharon SusmithaNo ratings yet
- How To Clean and JerkDocument3 pagesHow To Clean and JerkTim Donahey100% (4)
- 06/30/11 - Moneysaver - Lewis-Clark EditionDocument24 pages06/30/11 - Moneysaver - Lewis-Clark EditionDavid ArndtNo ratings yet
- Definition and Longvowelsand Short VowelsDocument8 pagesDefinition and Longvowelsand Short Vowelslinh nguyenNo ratings yet
- Osha UthmDocument19 pagesOsha UthmWan Muhammad Faiz Bin Mohd RoslanNo ratings yet
- Serpent of Isis Game WalkthroughDocument82 pagesSerpent of Isis Game WalkthroughGyörgyi FrajkovskýNo ratings yet
- Thesis CoutureDocument6 pagesThesis Couturemariapolitepalmdale100% (2)