Download as pdf or txt
You might also like
- Anatomy and Physiology: Prelim Laboratory Quiz 1Document35 pagesAnatomy and Physiology: Prelim Laboratory Quiz 1Aubrey Rosales100% (1)
- Journal 4Document5 pagesJournal 4dr. Nadia Salsabila100% (1)
- Manual Cavitadora Kim 8 EnglishDocument7 pagesManual Cavitadora Kim 8 EnglishEngelbert GuzmánNo ratings yet
- AP Biology Name - Chapter 6 Guided Reading AssignmentDocument6 pagesAP Biology Name - Chapter 6 Guided Reading AssignmentRobert Ladaga33% (3)
- Chest Part 3Document48 pagesChest Part 3rakshit09100% (1)
- Left Superior Intercostal VeinDocument3 pagesLeft Superior Intercostal VeinwurifreshNo ratings yet
- 05 Cardiac PDFDocument16 pages05 Cardiac PDFANAS ALINo ratings yet
- Congential Left Subclavian Steal Syndrome With Right Sided Aortic ArchDocument6 pagesCongential Left Subclavian Steal Syndrome With Right Sided Aortic ArchInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Aortic Tears1Document6 pagesAortic Tears1Syifa NurainiNo ratings yet
- Fundamentals of Diagnostic Radiology Cardiac MassesDocument2 pagesFundamentals of Diagnostic Radiology Cardiac MassesIkea BalhonNo ratings yet
- Cardiac ImagingDocument32 pagesCardiac ImagingRafid DragneelNo ratings yet
- Section XI - Cardiac Radiology: A. Sinus VenosusDocument8 pagesSection XI - Cardiac Radiology: A. Sinus VenosustoichongwNo ratings yet
- RadiographyDocument5 pagesRadiographyImha MikanersandsmashblastNo ratings yet
- Chest Anatomy. Chest AnatomyDocument70 pagesChest Anatomy. Chest AnatomydrelvNo ratings yet
- Radiology - Part 3 Post TestDocument24 pagesRadiology - Part 3 Post Testschating2No ratings yet
- Cardiac Radiology.Document13 pagesCardiac Radiology.Haluk AlibazogluNo ratings yet
- OMJ Anomalous Systemic Artery To A Normal Lung - A Rare Cause of Hemoptysis in AdultsDocument4 pagesOMJ Anomalous Systemic Artery To A Normal Lung - A Rare Cause of Hemoptysis in AdultsradiologirsckNo ratings yet
- 1 s2.0 S1878540920301705 MainDocument4 pages1 s2.0 S1878540920301705 MainBhagya Narayan PanditNo ratings yet
- Central Venous Access Line Subclavian Femoral IJ Jugular VeinDocument24 pagesCentral Venous Access Line Subclavian Femoral IJ Jugular VeinОлександр РабошукNo ratings yet
- Heart FailureDocument8 pagesHeart FailureAnonymous 71ChQ5pzNo ratings yet
- 42020E58E9FE69687The20Jugular20Venous20Pressure20and20Pulse20Contour20 20Clinical20Methods20 20NCBI20BookshelfDocument6 pages42020E58E9FE69687The20Jugular20Venous20Pressure20and20Pulse20Contour20 20Clinical20Methods20 20NCBI20BookshelfMayda MendozaNo ratings yet
- Heart Size MediastinalDocument11 pagesHeart Size MediastinalSherry FeliciaNo ratings yet
- Journal Reading - CT of Thoracic Lymph Nodes. Part I Anatomy and DrainageDocument45 pagesJournal Reading - CT of Thoracic Lymph Nodes. Part I Anatomy and DrainageVincentius Henry SundahNo ratings yet
- Radiological Signs of Lobar Collapse. Chest Radiographic Findings and CT ImagesDocument38 pagesRadiological Signs of Lobar Collapse. Chest Radiographic Findings and CT ImagesMuhammad ReyhanNo ratings yet
- CharlaDocument4 pagesCharlaCarlos Nicolas GordilloNo ratings yet
- Pi Is 0003497516313285Document3 pagesPi Is 0003497516313285Gordana PuzovicNo ratings yet
- Left Ventricular Diverticulum in Association With Bicuspid Aortic Valve and Pseudocoarctation: Hitherto Unreported AssociationDocument3 pagesLeft Ventricular Diverticulum in Association With Bicuspid Aortic Valve and Pseudocoarctation: Hitherto Unreported AssociationIsabella María GantivarNo ratings yet
- Thoracic Spine SurgeryDocument6 pagesThoracic Spine SurgeryAna GabrielaNo ratings yet
- 04-CVS - Nader 6 2019+++++++Document14 pages04-CVS - Nader 6 2019+++++++Refan NajiNo ratings yet
- Kardio Kel.2Document84 pagesKardio Kel.2Senja FajarNo ratings yet
- Arun Case CircDocument3 pagesArun Case CircDavin TakaryantoNo ratings yet
- Cardiac Anatomy Using CTDocument39 pagesCardiac Anatomy Using CTDyah KumalasariNo ratings yet
- Georgia TrumpDocument1 pageGeorgia Trumpjulia abanavasNo ratings yet
- Semester Paper (Sem 2 Jsmu, Aug, 2013) : Cont / /2012/05/diaphragm - PNGDocument3 pagesSemester Paper (Sem 2 Jsmu, Aug, 2013) : Cont / /2012/05/diaphragm - PNGJawad SamejoNo ratings yet
- Figure 308E-1: Normal Chest Radiograph-Review of Anatomy. 1. Trachea. 2Document35 pagesFigure 308E-1: Normal Chest Radiograph-Review of Anatomy. 1. Trachea. 2Pridina SyadirahNo ratings yet
- 09 IrDocument17 pages09 IrANAS ALINo ratings yet
- 2019 Pitfalls in Cardiac CTDocument8 pages2019 Pitfalls in Cardiac CTsabaxlentNo ratings yet
- Evaluation of Major Aortopulmonary Collateral Arteries (Mapcas) Using Three-Dimensional CT Angiography: Two Case ReportsDocument4 pagesEvaluation of Major Aortopulmonary Collateral Arteries (Mapcas) Using Three-Dimensional CT Angiography: Two Case ReportsninataniaaaNo ratings yet
- Hallazgos Radiológicos en La Disección Arterial Carotidea Espontanea. Papel Del Radiólogo en Esta EntidadDocument31 pagesHallazgos Radiológicos en La Disección Arterial Carotidea Espontanea. Papel Del Radiólogo en Esta EntidadDiana Adixa GarciaNo ratings yet
- Pathologic Cardiac Configuraion AjayDocument11 pagesPathologic Cardiac Configuraion AjayAJAY LALNo ratings yet
- 1 s2.0 S2468644123001299 MainDocument6 pages1 s2.0 S2468644123001299 MainRonald QuezadaNo ratings yet
- 4 Surgical Anatomy of The HeartDocument79 pages4 Surgical Anatomy of The HeartKacper DaraszkiewiczNo ratings yet
- Out 25Document5 pagesOut 25Noven MezaNo ratings yet
- Insuffisance Mitrale Apport deDocument2 pagesInsuffisance Mitrale Apport deBrahim PharmNo ratings yet
- 1rabio (Oo'.: Proceedings MedicineDocument12 pages1rabio (Oo'.: Proceedings MedicineMadhumala KumariNo ratings yet
- Sistemul CardiovascularDocument73 pagesSistemul CardiovascularAnda NicoletaNo ratings yet
- Chapter 2 - Surgical Anatomy of The HeartDocument36 pagesChapter 2 - Surgical Anatomy of The HeartbunzaiNo ratings yet
- 03-Chest - Nader 2 6 2019++++++++Document33 pages03-Chest - Nader 2 6 2019++++++++Refan NajiNo ratings yet
- Investigations - CXR: PA Film, Adequate Inspiration and Penetration FindingsDocument4 pagesInvestigations - CXR: PA Film, Adequate Inspiration and Penetration Findingshammer07No ratings yet
- HeartDocument37 pagesHeartpm7197362No ratings yet
- The Radiology Assistant - Basic InterpretationDocument67 pagesThe Radiology Assistant - Basic InterpretationMaria LimaNo ratings yet
- The Clinical Anatomy of Pericardiocentesis: Natomy of Ommon RoceduresDocument2 pagesThe Clinical Anatomy of Pericardiocentesis: Natomy of Ommon RoceduresAlfi NafiilaNo ratings yet
- Anatomi CardiovaskulerDocument76 pagesAnatomi CardiovaskulerPUTRINo ratings yet
- LinesDocument46 pagesLinesHarris ShaikhNo ratings yet
- Chest X Ray - BasicsDocument4 pagesChest X Ray - BasicsEd ChangNo ratings yet
- How To Read A Goofy Chest X Ray MbbsDocument70 pagesHow To Read A Goofy Chest X Ray MbbsrutendonormamapurisaNo ratings yet
- Radiology - All in OnDocument37 pagesRadiology - All in OnTop MusicNo ratings yet
- Biatrial Enlargement: An Unusual Cause of Massive CardiomegalyDocument2 pagesBiatrial Enlargement: An Unusual Cause of Massive CardiomegalynadiaNo ratings yet
- Anatomy & PhysiologyDocument38 pagesAnatomy & PhysiologyParsa EbrahimpourNo ratings yet
- Chest X-Ray InterpretationDocument67 pagesChest X-Ray Interpretationabhirajkale95% (20)
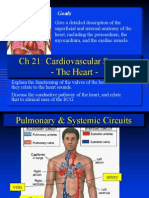
- CH 21: Cardiovascular System - The Heart - : GoalsDocument21 pagesCH 21: Cardiovascular System - The Heart - : GoalsgopscharanNo ratings yet
- Geometric Changes Allow Normal Ejection Fraction Despite Depressed Myocardial Shortening in Hypertensive Left Ventricular HypertrophyDocument8 pagesGeometric Changes Allow Normal Ejection Fraction Despite Depressed Myocardial Shortening in Hypertensive Left Ventricular Hypertrophymoh300No ratings yet
- The Cardiovascular System: The Heart: AnatomyDocument76 pagesThe Cardiovascular System: The Heart: AnatomyadnanNo ratings yet
- Surgical Critical Care and Emergency Surgery: Clinical Questions and AnswersFrom EverandSurgical Critical Care and Emergency Surgery: Clinical Questions and AnswersForrest "Dell" MooreNo ratings yet
- Del 2Document6 pagesDel 2Ed SllenNo ratings yet
- Del 3Document6 pagesDel 3Ed SllenNo ratings yet
- Xray PicDocument5 pagesXray PicEd SllenNo ratings yet
- Figure # 6. The Red Arrows Point To Typical Air Bronchograms in A Patient With A Segmental Pneumonia. Note There Is NoDocument4 pagesFigure # 6. The Red Arrows Point To Typical Air Bronchograms in A Patient With A Segmental Pneumonia. Note There Is NoEd SllenNo ratings yet
- Hand Hygiene Research PaperDocument3 pagesHand Hygiene Research PaperEd SllenNo ratings yet
- Blood Transfusion Protocols in NeonatesDocument12 pagesBlood Transfusion Protocols in NeonatesSupriya M A SuppiNo ratings yet
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoNo ratings yet
- 18 Digestion To Egestion-3Document43 pages18 Digestion To Egestion-3Princess NtleleNo ratings yet
- Anatomy of The Human Heart.Document22 pagesAnatomy of The Human Heart.Shimmering MoonNo ratings yet
- Reproductive System Quiz: Student Academic Learning ServicesDocument3 pagesReproductive System Quiz: Student Academic Learning ServicesMark Vincent SahagunNo ratings yet
- Cancer Book by DR - RamakrishnanDocument1 pageCancer Book by DR - RamakrishnanDr.Rajesh BartheNo ratings yet
- LyseDocument1 pageLyseHussein MohamedNo ratings yet
- Kami Export - CirculatorySystem12052022Document1 pageKami Export - CirculatorySystem12052022Nyla ScottNo ratings yet
- Hhis Lab PrelimDocument14 pagesHhis Lab PrelimMONICA VILLANUEVANo ratings yet
- Estágios Do Desenvolvimento Do EmbriãoDocument3 pagesEstágios Do Desenvolvimento Do EmbriãoDr SilvaNo ratings yet
- Cutaneous Wound HealingDocument78 pagesCutaneous Wound HealingClaudio Luis VenturiniNo ratings yet
- Pathological Anatomy CollegeDocument193 pagesPathological Anatomy CollegeHarsh NimavatNo ratings yet
- DNB ObstetricsDocument241 pagesDNB ObstetricsDilushini CalderaNo ratings yet
- Nayli Bio SBP 2019 EseiDocument5 pagesNayli Bio SBP 2019 EseiEqis AlfiesyaNo ratings yet
- Segmented Worms - Earthworm Anatomy: NameDocument5 pagesSegmented Worms - Earthworm Anatomy: NamePhantom AugustNo ratings yet
- Ex Cert IonDocument11 pagesEx Cert IonVicky BhardwajNo ratings yet
- Soft Tissue SarcomasDocument8 pagesSoft Tissue SarcomasHerman PurnomoNo ratings yet
- Suturing and Closure: March 2020Document26 pagesSuturing and Closure: March 2020yui cherryNo ratings yet
- Exocrine Glands Are Those Which Release Their Cellular Secretions Through A Duct Which EmptiesDocument2 pagesExocrine Glands Are Those Which Release Their Cellular Secretions Through A Duct Which EmptiesEllee HadesNo ratings yet
- Tumor Pada Ginjal: Dr.H.Delyuzar, M.Ked (Pa), Sppa (K)Document134 pagesTumor Pada Ginjal: Dr.H.Delyuzar, M.Ked (Pa), Sppa (K)Dony DamaraNo ratings yet
- Plant Body Chap5Document71 pagesPlant Body Chap5bry uyNo ratings yet
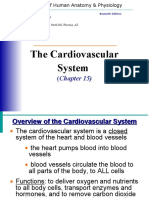
- The Cardiovascular System: (Chapter 15)Document59 pagesThe Cardiovascular System: (Chapter 15)Hasanuddin NuruNo ratings yet
- Why Is It Necessary For The Trachea To Have Rings of Cartilage in Its WallsDocument3 pagesWhy Is It Necessary For The Trachea To Have Rings of Cartilage in Its Wallsapi-265276766No ratings yet
- Review - Spinal Cord Injury - 2Document1 pageReview - Spinal Cord Injury - 2Sarah MendozaNo ratings yet
- Human Embryonic DevelopmentDocument8 pagesHuman Embryonic DevelopmentGargi BhattacharyaNo ratings yet
- Neuromuscular System: Questions 261-266Document24 pagesNeuromuscular System: Questions 261-266Bach XuanNo ratings yet