
Advanced Vulvar Paget's Disease Insight Into A Rare Presentation
Advanced Vulvar Paget's Disease Insight Into A Rare Presentation
You might also like
- Adhd Diva - 5Document20 pagesAdhd Diva - 5quaz488% (17)
- Drugs Acting On Lower RespiratoryDocument45 pagesDrugs Acting On Lower RespiratoryHannah Lorraine Gamayon100% (1)
- Common Drugs Used in The EmergencyDocument5 pagesCommon Drugs Used in The Emergencyhatem alsrour88% (25)
- 5) 308 NM Excimer Laser A Hopeful and Optional Therapy For Pityriasis VersicolorDocument6 pages5) 308 NM Excimer Laser A Hopeful and Optional Therapy For Pityriasis VersicolorFathia KhattabNo ratings yet
- Clinical Treatment of Vulvar Paget's Disease: A CaseDocument3 pagesClinical Treatment of Vulvar Paget's Disease: A CaseDeliaNo ratings yet
- 1 s2.0 S2214442022002121 MainDocument3 pages1 s2.0 S2214442022002121 MainGregory AssonitisNo ratings yet
- Hemdan 2014Document6 pagesHemdan 2014DavorIvanićNo ratings yet
- Balanoposthitis With Epithelial Dysplasia Treated by Photodynamic TherapyDocument3 pagesBalanoposthitis With Epithelial Dysplasia Treated by Photodynamic TherapyTeja Laksana NukanaNo ratings yet
- Clin Cas 1Document5 pagesClin Cas 1Dragos Viorel ScripcariuNo ratings yet
- QUAD. 0 7 21 RegimenDocument6 pagesQUAD. 0 7 21 RegimenEskadmas BelayNo ratings yet
- Double Rarities, Double Challenges: Extra-Mammary Paget's Disease and Anal AdenocarcinomaDocument4 pagesDouble Rarities, Double Challenges: Extra-Mammary Paget's Disease and Anal AdenocarcinomaLaura PredescuNo ratings yet
- Jco 38 1763Document12 pagesJco 38 1763solifugae123No ratings yet
- 1 s2.0 S1028455922002935 MainDocument4 pages1 s2.0 S1028455922002935 Mainmodacasper056No ratings yet
- VitiligoDocument3 pagesVitiligoAulia Chandra DwiNo ratings yet
- Gynecology and Minimally Invasive Therapy: Case ReportDocument5 pagesGynecology and Minimally Invasive Therapy: Case ReportMetharisaNo ratings yet
- 4451 FullDocument4 pages4451 FullSukhvinder Singh RanaNo ratings yet
- Josephson 2007Document15 pagesJosephson 2007nimaelhajjiNo ratings yet
- Medicine 1Document2 pagesMedicine 1ÇağlaNo ratings yet
- Randomized Controlled Trial of Live LactobacillusDocument6 pagesRandomized Controlled Trial of Live LactobacilluscarolineNo ratings yet
- Achy 2017 01 005Document8 pagesAchy 2017 01 005Head RadiotherapyNo ratings yet
- Recurrent Ta Low-Grade Non-Muscle-Invasive Bladder Cancer: What Are The Options?Document7 pagesRecurrent Ta Low-Grade Non-Muscle-Invasive Bladder Cancer: What Are The Options?Dr. Alexandre SatoNo ratings yet
- Concurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaDocument5 pagesConcurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaIjsrnet EditorialNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyTit fuckerNo ratings yet
- Harrington 2015Document16 pagesHarrington 2015Geoffroy De VilmarestNo ratings yet
- Radio - Oncology 2008Document95 pagesRadio - Oncology 2008api-3856051100% (2)
- Palliation of Dysphagia in Locally Advanced Carcinoma Esophagus - Exploration of Two Different Radiotherapy SchedulesDocument3 pagesPalliation of Dysphagia in Locally Advanced Carcinoma Esophagus - Exploration of Two Different Radiotherapy SchedulesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 10 1016@j Jfma 2018 01 015Document10 pages10 1016@j Jfma 2018 01 015darpa22No ratings yet
- Case Report A Rare Case of Metastatic Primary Peritoneal Ependymoma: A Case Report and Literature ReviewDocument8 pagesCase Report A Rare Case of Metastatic Primary Peritoneal Ependymoma: A Case Report and Literature Reviewnurul auliaNo ratings yet
- Ijcmr 2030 v1Document3 pagesIjcmr 2030 v1SathyaNo ratings yet
- Nejmoa 2032125Document13 pagesNejmoa 2032125CARLOS DURANNo ratings yet
- NPCDocument8 pagesNPCArsy Mira PertiwiNo ratings yet
- Garcia Del Muro2008Document6 pagesGarcia Del Muro2008Bruno AlanNo ratings yet
- SouthAsianJCancer6115-2517942 065939Document5 pagesSouthAsianJCancer6115-2517942 065939Gibi SupitNo ratings yet
- Rectal CancerDocument4 pagesRectal CancerAlice AugustinNo ratings yet
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDocument6 pagesLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraNo ratings yet
- 559 FullDocument5 pages559 FullSukhvinder Singh RanaNo ratings yet
- Mucinous Neoplasm of Appendix TreatmentDocument3 pagesMucinous Neoplasm of Appendix TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Phase II INTERACT-ION Study: Ezabenlimab (BI 754091) and MDCF (Docetaxel, Cisplatin, and 5-Fluorouracil) Followed by Chemoradiotherapy in Patients With Stage III Squamous Cell Anal CarcinomaDocument11 pagesPhase II INTERACT-ION Study: Ezabenlimab (BI 754091) and MDCF (Docetaxel, Cisplatin, and 5-Fluorouracil) Followed by Chemoradiotherapy in Patients With Stage III Squamous Cell Anal CarcinomaStefano KimNo ratings yet
- Cisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412Document6 pagesCisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412ZuriNo ratings yet
- Pathologic Response When Increased by Longer Interva - 2016 - International JouDocument10 pagesPathologic Response When Increased by Longer Interva - 2016 - International Jouwilliam tandeasNo ratings yet
- PALLIATIVE RadiationDocument13 pagesPALLIATIVE RadiationFeras OskanNo ratings yet
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 pagesPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007No ratings yet
- Gynecologic Oncology Reports: Sarah Z. Hazell, Rebecca L. Stone, Je Ffrey Y. Lin, Akila N. ViswanathanDocument4 pagesGynecologic Oncology Reports: Sarah Z. Hazell, Rebecca L. Stone, Je Ffrey Y. Lin, Akila N. ViswanathanWassCANNo ratings yet
- The Evolving Role of Hypofractionated Radiotherapy in Older Adults With Gastrointestinal CancersDocument9 pagesThe Evolving Role of Hypofractionated Radiotherapy in Older Adults With Gastrointestinal CancersRaul Matute MartinNo ratings yet
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaNo ratings yet
- Khosrowmomtaz 1998Document8 pagesKhosrowmomtaz 1998Mariana JuravleNo ratings yet
- Early Versus Late Surgery For Ileo-Caecal Crohn's Disease: Alimentary Pharmacology & TherapeuticsDocument10 pagesEarly Versus Late Surgery For Ileo-Caecal Crohn's Disease: Alimentary Pharmacology & TherapeuticsBernadett FarkasNo ratings yet
- Cancer of The EsophagusDocument6 pagesCancer of The EsophagusDileep SrinivasanNo ratings yet
- Gastrointestinal 132Document8 pagesGastrointestinal 132Minerva Medical Treatment Pvt LtdNo ratings yet
- 1627-Article Text-2378-1-10-20220708Document3 pages1627-Article Text-2378-1-10-20220708gfr9px8db6No ratings yet
- Narrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaDocument6 pagesNarrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaJavier Perez ManriquezNo ratings yet
- Journal of Gastroenterology and Hepatology (2013)Document1 pageJournal of Gastroenterology and Hepatology (2013)Norberto MolloNo ratings yet
- MP CorticoadrenalesDocument13 pagesMP CorticoadrenalesJuan Torres MeleroNo ratings yet
- Glandula SalivarDocument8 pagesGlandula SalivarporsanimedNo ratings yet
- Adjuvant RadiotherapyDocument7 pagesAdjuvant Radiotherapyciko momonNo ratings yet
- Outpatient Rituximab, Ifosfamide, Etoposide (R-IE) in Patients Older Than 60 Years With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Who Are Not Candidates For Stem Cell TransplantationDocument8 pagesOutpatient Rituximab, Ifosfamide, Etoposide (R-IE) in Patients Older Than 60 Years With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Who Are Not Candidates For Stem Cell TransplantationAudrey DSNo ratings yet
- Gastric RTDocument10 pagesGastric RTLjupka Banar PoposkaNo ratings yet
- MedulloblastomaDocument3 pagesMedulloblastomaMohammadAwitNo ratings yet
- JFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisDocument2 pagesJFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisBilalNo ratings yet
- JR Kemo TitaDocument21 pagesJR Kemo TitaTitaPuspitasariNo ratings yet
- Diificult AirwayDocument13 pagesDiificult AirwayBhi-An BatobalonosNo ratings yet
- A Retrospective Analysis On Treatment and Survival Outcome of Locally Advanced Cervical CancerDocument11 pagesA Retrospective Analysis On Treatment and Survival Outcome of Locally Advanced Cervical CancerdlledlycnNo ratings yet
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- Effectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceDocument10 pagesEffectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of the Quality of Community Satisfaction in Public Services in Tanjungpinang Class I State Detention HouseDocument13 pagesAnalysis of the Quality of Community Satisfaction in Public Services in Tanjungpinang Class I State Detention HouseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of the Effectiveness of Based Public Services Information and Communication Technology (ICT)Document10 pagesAnalysis of the Effectiveness of Based Public Services Information and Communication Technology (ICT)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Effects of Nanoplastics on Human Health: A Comprehensive StudyDocument7 pagesEffects of Nanoplastics on Human Health: A Comprehensive StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Anti-Diabetic Semaglutide: A GLP-1 RA PeptideDocument11 pagesOral Anti-Diabetic Semaglutide: A GLP-1 RA PeptideInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Zilebesiran: The First siRNA Drug Therapy for HypertensionDocument5 pagesZilebesiran: The First siRNA Drug Therapy for HypertensionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Analysis of Various Formwork SystemsDocument6 pagesDesign and Analysis of Various Formwork SystemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyDocument8 pagesNurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Association Between Gender and Depression Among College StudentsDocument4 pagesAssociation Between Gender and Depression Among College StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Salivary Diagnostics in Oral and Systemic Diseases - A ReviewDocument5 pagesSalivary Diagnostics in Oral and Systemic Diseases - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityDocument9 pagesShift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Environmental Sanitation – A Therapy for Healthy Living for Sustainable Development. A Case Study of Argungu Township Kebbi State, North Western NigeriaDocument15 pagesEnvironmental Sanitation – A Therapy for Healthy Living for Sustainable Development. A Case Study of Argungu Township Kebbi State, North Western NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Reintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveDocument1 pageReintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyDocument6 pagesMSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyDocument6 pagesEvaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesDocument5 pagesBiometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Appraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateDocument12 pagesAppraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateDocument6 pagesOccupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateInternational Journal of Innovative Science and Research Technology100% (1)
- Prevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyDocument4 pagesPrevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AI Robots in Various SectorDocument3 pagesAI Robots in Various SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)Document7 pagesAn Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Dynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnDocument3 pagesDynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dr. Joseph Stan DDS - Cosmetic Dentist & Dental Implant Specialist in Beverly Hills & Los Angeles, CADocument8 pagesDr. Joseph Stan DDS - Cosmetic Dentist & Dental Implant Specialist in Beverly Hills & Los Angeles, CAjosephstanddsNo ratings yet
- Managing OtitisDocument9 pagesManaging OtitisdanielguerinNo ratings yet
- Neonatal EmergenciesDocument21 pagesNeonatal EmergenciesRNo ratings yet
- Effect of Preterm Infant Massage by The Mother On The Mood of Mothers Having Preterm InfantsDocument10 pagesEffect of Preterm Infant Massage by The Mother On The Mood of Mothers Having Preterm InfantsopanocayNo ratings yet
- COVID-19 Vaccine Developers Oxford-AstraZeneca Linked To British Eugenics MovementDocument18 pagesCOVID-19 Vaccine Developers Oxford-AstraZeneca Linked To British Eugenics MovementOwen KingNo ratings yet
- Epidemiology of Parkinson'S Disease: SciencedirectDocument13 pagesEpidemiology of Parkinson'S Disease: SciencedirectAleja ToPaNo ratings yet
- Sickle Cell Anemia Control Program: (A Major Tribal Health Program of Gujarat)Document29 pagesSickle Cell Anemia Control Program: (A Major Tribal Health Program of Gujarat)Sutapa PawarNo ratings yet
- PI Ferinject PDFDocument2 pagesPI Ferinject PDFMostofa RubalNo ratings yet
- Subjective and Objective DataDocument9 pagesSubjective and Objective DatagraceNo ratings yet
- Quinn TJ, Langhorne P, Stott DJ (2011) - Barthel Index For Stroke Trials: Development, Properties, and Application. Stroke. 42: 1146-1151Document2 pagesQuinn TJ, Langhorne P, Stott DJ (2011) - Barthel Index For Stroke Trials: Development, Properties, and Application. Stroke. 42: 1146-1151Sausan Hana MaharaniNo ratings yet
- Clinical Guideline: Aminoglycoside: Recommendations For Use, Dosing and Monitoring Clinical GuidelineDocument16 pagesClinical Guideline: Aminoglycoside: Recommendations For Use, Dosing and Monitoring Clinical GuidelineVita LesielaNo ratings yet
- PerrobinDocument6 pagesPerrobinVicente RivanoNo ratings yet
- Bricks Intensive Reading - L2 - Word List BDocument16 pagesBricks Intensive Reading - L2 - Word List BNathaniel McleodNo ratings yet
- Gardasil VAERS Adverse ReactionsDocument1,824 pagesGardasil VAERS Adverse Reactionsmcdonald.rr100% (2)
- Nursingstaff: Annotated BibliographyDocument5 pagesNursingstaff: Annotated BibliographyAnnette BainesNo ratings yet
- Clinical Neurology and NeurosurgeryDocument8 pagesClinical Neurology and NeurosurgeryMasithaNo ratings yet
- Clinical Case Book MeDioStar 2018-11Document48 pagesClinical Case Book MeDioStar 2018-11medspa49No ratings yet
- Challenges and Opportunities of Clinical Pharmacy Services in Ethiopia: A Qualitative Study From Healthcare Practitioners' PerspectiveDocument7 pagesChallenges and Opportunities of Clinical Pharmacy Services in Ethiopia: A Qualitative Study From Healthcare Practitioners' Perspectivebekalu dessieNo ratings yet
- Allergic Rhinitis: Dr. Fauziah Henny, SP - THT-KLDocument14 pagesAllergic Rhinitis: Dr. Fauziah Henny, SP - THT-KLIsra AbdiNo ratings yet
- Project Proposal For PIMA Hospital Mansehra Prof Iqbal KhanDocument14 pagesProject Proposal For PIMA Hospital Mansehra Prof Iqbal KhanMuhmmad TahaNo ratings yet
- Liability and Consent FormDocument2 pagesLiability and Consent Formapi-19917129No ratings yet
- Essential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 3 PDFDocument1 pageEssential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 3 PDFMariam QaisNo ratings yet
- Bioanalysis NotesDocument7 pagesBioanalysis NoteskeerthiNo ratings yet
- 9007 - 9008 - Convercation For Cheking Vital Nurse (Diarrhea) - 3A S.TR KeperawatanDocument4 pages9007 - 9008 - Convercation For Cheking Vital Nurse (Diarrhea) - 3A S.TR Keperawatandiahpurnama dewiNo ratings yet
- Emergency and Disaster Nursing NewDocument42 pagesEmergency and Disaster Nursing Newlalufebrian hendika25No ratings yet
- NSSK Training Aug, 16Document3 pagesNSSK Training Aug, 16Chhote yadavNo ratings yet
- Preventing Hospital Infections Real World Problems Realistic Solutions 2Nd Edition Jennifer Meddings Download PDF ChapterDocument52 pagesPreventing Hospital Infections Real World Problems Realistic Solutions 2Nd Edition Jennifer Meddings Download PDF Chaptermary.schoonmaker770100% (11)






















































































































Download as pdf or txt
Volume 6, Issue 8, August – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Advanced Vulvar Paget’s Disease:
Insight into a Rare Presentation
Tarangini Yadav1, Diptajit Paul2, Vivek Kaushal3
1.
Junior Resident
2.
Senior Resident
3.
Senior Professor and Head of Department
Department of Radiation Oncology, Pt. B. D. Sharma PGIMS, Rohtak
Corresponding author: Diptajit Paul, Senior Resident, Department of Radiation Oncology, Pt. B. D. Sharma PGIMS, Rohtak,
Haryana, India
Abstract:- Extra-mammary Paget’s disease, a rare II.CASE SUMMARY
neoplasm, have variable rates of invasion. Vulva is the
most common extra mammary site, others being A 71-year-old woman presented with an ulcerated
perineal, perianal and scrotal region in a few cases. lesion in vulva for 1-year duration, which was insidious in
Presence of Paget’s cells in tissue biopsy confirms the onset, rapidly growing in size, painless but accompanied by
diagnosis, whereas invasion beyond basement to pruritus. The pruritus was severe in intensity, off and on
surrounding structure is associated with malignant type, lasted locally in vulva for last 8-years, partially
nature of disease. It commonly occurs in relieved by topical ointment appo8lication. She had no
postmenopausal, elderly females. This case reports told associated history of fever, weight loss, anorexia, headache,
off a 71-year-old woman presented with an ulcerated chest or abdominal discomfort. She was non-smoker, non-
lesion in vulva for 1-year duration which came out as alcoholic and not having any chronic illness. Patient had no
invasive vulvar Paget’s disease. Wide local excision history of abnormal uterine bleeding and had attained
followed by post-operative whole pelvic irradiation was menopause 20-years ago, menstrual cycles were uneventful.
given for radical cure. Unfortunately, patient had local She had 2 children, delivered vaginally at government
reoccurrence within 1-year and was given metronomic hospital. General physical and systemic examination was
chemotherapy with oral cyclophosphamide and normal. Local examination revealed a 4.0 × 3.0 cm
capecitabine primarily. As disease was progressive in ulcerated, bright red, eczematous lesion in vulva and labia
this regimen, she was shifted to metronomic majora, more prominent on left side.
chemotherapy with oral methotrexate and celecoxib.
Patient had got symptomatic relief with current regimen The patient’s routine blood tests including complete
and is continuing the regimen for last 3-years. This case hemogram and blood biochemistry profile, ultrasound of
report showed the high chance of reoccurrence in vulvar abdomen-pelvis region and chest radiograph were within
Paget’s disease and partial response to oral methotrexate normal limits. Patient underwent wide local excision of
in such condition. More case reports and case series are labial lesion with vulvar reconstruction. Histopathology of
needed for driving the definite conclusions on treatment surgical specimen revealed Paget’s cell in the lesion &
protocol and role of oral metronomic chemotherapy for surrounding epithelium and strong cytokeratin 7 (CK 7)
invasive vulvar Paget’s disease. positivity in tumor cell was noted by immunohistochemistry
(IHC) staining. The histopathology and IHC appearance
Keywords:- Vulvar Paget’s Disease; Wide Local Excision, confirmed it as a case of vulvar Paget’s disease with
Whole Pelvic Irradiation, Metronomic Chemotherapy. invasion into surrounding tissue.
I.INTRODUCTION To prevent local recurrence, patient was given post-
operative whole pelvic irradiation in dose of 54 gray (Gy) in
Most common site of extra-mammary Paget’s disease 30 fractions over 6 weeks. After that, she was on regular
is vulvar region. It is a tenacious condition with higher follow-up and remained asymptomatic for 14-months.
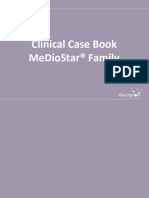
prevalence of relapse and currently requires multi-modality Subsequently, the patient presented with red velvety
management. Here, we present a case of recurrent, invasive ulcerated lesion with areas of necrosis in vulva and labia
valvar Paget’s disease in an old lady treated by majora more on left side having a size of 4.0 × 6.5 cm
multidisciplinary approach of surgery, radiation and implying disease recurrence (Figure 1).
chemotherapy.
IJISRT21AUG556 www.ijisrt.com 1310
Volume 6, Issue 8, August – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Radiation therapy (RT) is an option as definitive
treatment for patients not eligible for surgery (medically
unfit) or not willing for surgery. It can also be given in post-
operative settings to prevent local recurrence and as second
line treatment in patients having recurrence after surgery.
Recommended dose range of radiation therapy is 55 Gy to
65 Gy by conventional fractionation for invasive vulvar
Paget’s disease. [9] Long-term follow-up in post
radiotherapy patients showed less recurrence rates. [4]
A few numbers of chemotherapy related studies have
been conducted till date, which limit the value of its
significance. This includes clinical trials with FECOM (5-
Figure 1: Ulcerated, bright red, eczematous lesion in vulva fluorouracil, epirubicin, carboplatin, vincristine, and
and labia majora. mitomycin-C) regimen; FEC100 (fluorouracil, epirubicin,
and cyclophosphamide) regimen followed by docetaxel;
She was given oral metronomic chemotherapy with cyclophosphamide and capecitabine; methotrexate and
tablet cyclophosphamide (50 mg daily) and tablet celecoxib with variable outcome. [10-13] Regimen
capecitabine (500 mg twice daily) for 3-years. Despite consisting of trastuzumab along with paclitaxel was also
having this treatment, the disease was still progressing and explored in a case report having lymph node metastatic Her-
patient was given therapeutic trials of metronomic 2-neu positive vulvar Paget disease, which showed partial
chemotherapy with oral methotrexate tablet (25 mg once response in terms of lymph node regression. [14]
weekly) and capsule celecoxib (20 mg twice daily). Patient
had got symptomatic relief with current regimen and is In our case, patient was given post-operative adjuvant
continuing the regimen for last 3-years. radiation therapy to prevent local recurrence within 1-month
of surgical intervention. Later on, patient had reoccurrence
after 14 months and then modality of treatment was changed
III.DISCUSSION
to novel oral metronomic chemotherapy that is
cyclophosphamide & capecitabine. 3-years later another
Extra-mammary Paget’s disease is an infrequent novel regimen was explored in view of disease progression,
disorder with 6.5% frequentness and variable rates of which consisted of oral methotrexate. The patient has stable
invasion. [1] Vulva is the most frequent extra-mammary disease and is being on monthly follow up since last 3-years.
site, others being perineal, perianal and scrotal region in a
few cases. It is often difficult to diagnose and is frequently IV.CONCLUSION
present for many years before treatment begins. [2] It
commonly occurs in females having old age after
Invasive Paget’s disease of vulva is an infrequent
menopause. [3] Once diagnosed, it is being classified by
entity having aggressive clinical behavior. Majority of the
Wilkinson and Brown system of classification into primary
cases do not resolve completely and have off and on
(cutaneous origin) and secondary (non-cutaneous origin). [4]
recurrence pattern. Radical curative intent is the initial
The survival is not so poor with an 5-year overall survival is
approach, but often palliation of symptoms becomes the
around 70%, however disease remain off and on in most of
goal of treatment. In our case, surgery followed by adjuvant
the surviving females. [5] The invasiveness contributed in
radiotherapy was employed first for radical cure and
12% of diagnosed cases and have high relapse rate i.e. 12 to
61% with an average of 2 recurrences per patient. [6] In metronomic chemotherapy was given while there was
general, dermal invasion being key factor predicting recurrence. However, the treatment yielded partial response
and good subjective symptomatic relief. More case reports
recurrence, whereas role of pathologic features, R0
are needed for driving the definite conclusions on treatment
resectability, tumor cell aneuploidy, hormone receptor
protocol and role of oral metronomic chemotherapy for
positivity, and cytogenetic abnormality in local recurrence is
invasive vulvar Paget’s disease.
under research. [7]
REFERENCES
The initial treatment of choice for lesion confined to
vulva is surgical intervention which mainly consist of wide
[1]. McDaniel B, Brown F, Crane JS. Extramammary
local excision (WLE) with local (inguino-femoral) lymph
Paget Disease. In: StatPearls. StatPearls Publishing,
node dissection in majority of cases. The main challenge is
Treasure Island (FL); 2020. PMID: 29630276.
of obtaining clear R0 surgical margin. In majority of cases,
[2]. Bouceiro-Mendes R, Mendonça-Sanches M, Soares-
patients have post-operative local complications which are
infection, hematomas and wound breakdown (incidence de-Almeida L, Correia-Fonseca I. A case of chronic
and relapsing Paget disease of the vulva. Revista
rates: 9–45%). [4] The post-surgery recurrence rates are also
Brasileira de Ginecologia e Obstetrícia. 2019 Jul
high (about 58%) with significant morbidity and these are
22;41:412-6.
similar to patient who didn’t underwent surgery. [8].
[3]. Fanning J, Lambert HC, Hale TM, Morris PC,
Therefore, there is need for alternative treatment approach.
Schuerch C. Paget's disease of the vulva: prevalence of
IJISRT21AUG556 www.ijisrt.com 1311
Volume 6, Issue 8, August – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
associated vulvar adenocarcinoma, invasive Paget's
disease, and recurrence after surgical excision. Am J
Obstet Gynecol. 1999 Jan;180(1 Pt 1):24-7.
[4]. van der Linden M, Meeuwis KA, Bulten J, Bosse T,
van Poelgeest MI, de Hullu JA. Paget disease of the
vulva. Crit Rev Oncol Hematol. 2016 May;101:60-74.
[5]. Borghi C, Bogani G, Ditto A, Martinelli F, Signorelli
M, Chiappa V et al. Invasive Paget disease of the
vulva. Int J Gynecol Cancer. 2018 Jan;28(1):176-82.
[6]. Nitecki R, Davis M, Watkins JC, Wu YE, Vitonis AF,
Muto MG et al. Extramammary Paget disease of the
vulva: a case series examining treatment, recurrence,
and malignant transformation. Int J Gynecol Cancer.
2018 Mar 1;28(3).
[7]. Shaco-Levy R, Bean SM, Vollmer RT, Papalas JA,
Bentley RC, Selim MA et al. Paget disease of the
vulva: a histologic study of 56 cases correlating
pathologic features and disease course. Int J of
Gynecol Pathol. 2010 Jan 1;29(1):69-78.
[8]. Onaiwu CO, Salcedo MP, Pessini SA, Munsell MF,
Euscher EE, Reed KE et al. Paget's disease of the
vulva: A review of 89 cases. Gynecol Oncol Rep. 2017
Feb 1;19:46-9.
[9]. Son SH, Lee JS, Kim YS, Ryu MR, Chung SM,
Namkoong SE et al. The role of radiation therapy for
the extramammary paget's disease of the vulva;
experience of 3 cases. Cancer Res Treat. 2005
Dec;37(6):365-9.
[10]. Oashi K, Tsutsumida A, Namikawa K, Tanaka R,
Omata W, Yamamoto Y et al. Combination
chemotherapy for metastatic extramammary Paget
disease. Br J Dermatol. 2014 Jun;170(6):1354-7.
[11]. Tauveron V, Body G, Machet L, Lenain H, Ouldamer
L, Lorette G. Prolonged remission of Paget disease of
the vulva after chemotherapy for breast carcinoma. Br
J Dermatol. 2014;170(5):1199-200.
[12]. Downey L, Livingston R, Stopeck A. Diagnosing and
treating breast cancer in elderly women: a call for
improved understanding. J Am Geriatr Soc. 2007
Oct;55(10):1636-44.
[13]. Lebas E, Chapelier C, Quatresooz P, Seidel L, Nikkels
AF. Exploratory assessment of oxygen flow–assisted
cutaneous administration of methotrexate for
superficial basal cell carcinoma, mycosis fungoides,
and extramammary Paget disease. J Invest Dermatol.
2020 Mar 1;140(3):583-92.
[14]. Hanawa F, Inozume T, Harada K, Kawamura T,
Shibagaki N, Shimada S. A case of metastatic
extramammary Paget’s disease responding to
trastuzumab plus paclitaxel combination therapy. Case
Rep Dermatol. 2011;3(3):223-7.
IJISRT21AUG556 www.ijisrt.com 1312
You might also like
- Adhd Diva - 5Document20 pagesAdhd Diva - 5quaz488% (17)
- Drugs Acting On Lower RespiratoryDocument45 pagesDrugs Acting On Lower RespiratoryHannah Lorraine Gamayon100% (1)
- Common Drugs Used in The EmergencyDocument5 pagesCommon Drugs Used in The Emergencyhatem alsrour88% (25)
- 5) 308 NM Excimer Laser A Hopeful and Optional Therapy For Pityriasis VersicolorDocument6 pages5) 308 NM Excimer Laser A Hopeful and Optional Therapy For Pityriasis VersicolorFathia KhattabNo ratings yet
- Clinical Treatment of Vulvar Paget's Disease: A CaseDocument3 pagesClinical Treatment of Vulvar Paget's Disease: A CaseDeliaNo ratings yet
- 1 s2.0 S2214442022002121 MainDocument3 pages1 s2.0 S2214442022002121 MainGregory AssonitisNo ratings yet
- Hemdan 2014Document6 pagesHemdan 2014DavorIvanićNo ratings yet
- Balanoposthitis With Epithelial Dysplasia Treated by Photodynamic TherapyDocument3 pagesBalanoposthitis With Epithelial Dysplasia Treated by Photodynamic TherapyTeja Laksana NukanaNo ratings yet
- Clin Cas 1Document5 pagesClin Cas 1Dragos Viorel ScripcariuNo ratings yet
- QUAD. 0 7 21 RegimenDocument6 pagesQUAD. 0 7 21 RegimenEskadmas BelayNo ratings yet
- Double Rarities, Double Challenges: Extra-Mammary Paget's Disease and Anal AdenocarcinomaDocument4 pagesDouble Rarities, Double Challenges: Extra-Mammary Paget's Disease and Anal AdenocarcinomaLaura PredescuNo ratings yet
- Jco 38 1763Document12 pagesJco 38 1763solifugae123No ratings yet
- 1 s2.0 S1028455922002935 MainDocument4 pages1 s2.0 S1028455922002935 Mainmodacasper056No ratings yet
- VitiligoDocument3 pagesVitiligoAulia Chandra DwiNo ratings yet
- Gynecology and Minimally Invasive Therapy: Case ReportDocument5 pagesGynecology and Minimally Invasive Therapy: Case ReportMetharisaNo ratings yet
- 4451 FullDocument4 pages4451 FullSukhvinder Singh RanaNo ratings yet
- Josephson 2007Document15 pagesJosephson 2007nimaelhajjiNo ratings yet
- Medicine 1Document2 pagesMedicine 1ÇağlaNo ratings yet
- Randomized Controlled Trial of Live LactobacillusDocument6 pagesRandomized Controlled Trial of Live LactobacilluscarolineNo ratings yet
- Achy 2017 01 005Document8 pagesAchy 2017 01 005Head RadiotherapyNo ratings yet
- Recurrent Ta Low-Grade Non-Muscle-Invasive Bladder Cancer: What Are The Options?Document7 pagesRecurrent Ta Low-Grade Non-Muscle-Invasive Bladder Cancer: What Are The Options?Dr. Alexandre SatoNo ratings yet
- Concurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaDocument5 pagesConcurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaIjsrnet EditorialNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyTit fuckerNo ratings yet
- Harrington 2015Document16 pagesHarrington 2015Geoffroy De VilmarestNo ratings yet
- Radio - Oncology 2008Document95 pagesRadio - Oncology 2008api-3856051100% (2)
- Palliation of Dysphagia in Locally Advanced Carcinoma Esophagus - Exploration of Two Different Radiotherapy SchedulesDocument3 pagesPalliation of Dysphagia in Locally Advanced Carcinoma Esophagus - Exploration of Two Different Radiotherapy SchedulesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 10 1016@j Jfma 2018 01 015Document10 pages10 1016@j Jfma 2018 01 015darpa22No ratings yet
- Case Report A Rare Case of Metastatic Primary Peritoneal Ependymoma: A Case Report and Literature ReviewDocument8 pagesCase Report A Rare Case of Metastatic Primary Peritoneal Ependymoma: A Case Report and Literature Reviewnurul auliaNo ratings yet
- Ijcmr 2030 v1Document3 pagesIjcmr 2030 v1SathyaNo ratings yet
- Nejmoa 2032125Document13 pagesNejmoa 2032125CARLOS DURANNo ratings yet
- NPCDocument8 pagesNPCArsy Mira PertiwiNo ratings yet
- Garcia Del Muro2008Document6 pagesGarcia Del Muro2008Bruno AlanNo ratings yet
- SouthAsianJCancer6115-2517942 065939Document5 pagesSouthAsianJCancer6115-2517942 065939Gibi SupitNo ratings yet
- Rectal CancerDocument4 pagesRectal CancerAlice AugustinNo ratings yet
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDocument6 pagesLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraNo ratings yet
- 559 FullDocument5 pages559 FullSukhvinder Singh RanaNo ratings yet
- Mucinous Neoplasm of Appendix TreatmentDocument3 pagesMucinous Neoplasm of Appendix TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Phase II INTERACT-ION Study: Ezabenlimab (BI 754091) and MDCF (Docetaxel, Cisplatin, and 5-Fluorouracil) Followed by Chemoradiotherapy in Patients With Stage III Squamous Cell Anal CarcinomaDocument11 pagesPhase II INTERACT-ION Study: Ezabenlimab (BI 754091) and MDCF (Docetaxel, Cisplatin, and 5-Fluorouracil) Followed by Chemoradiotherapy in Patients With Stage III Squamous Cell Anal CarcinomaStefano KimNo ratings yet
- Cisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412Document6 pagesCisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412ZuriNo ratings yet
- Pathologic Response When Increased by Longer Interva - 2016 - International JouDocument10 pagesPathologic Response When Increased by Longer Interva - 2016 - International Jouwilliam tandeasNo ratings yet
- PALLIATIVE RadiationDocument13 pagesPALLIATIVE RadiationFeras OskanNo ratings yet
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 pagesPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007No ratings yet
- Gynecologic Oncology Reports: Sarah Z. Hazell, Rebecca L. Stone, Je Ffrey Y. Lin, Akila N. ViswanathanDocument4 pagesGynecologic Oncology Reports: Sarah Z. Hazell, Rebecca L. Stone, Je Ffrey Y. Lin, Akila N. ViswanathanWassCANNo ratings yet
- The Evolving Role of Hypofractionated Radiotherapy in Older Adults With Gastrointestinal CancersDocument9 pagesThe Evolving Role of Hypofractionated Radiotherapy in Older Adults With Gastrointestinal CancersRaul Matute MartinNo ratings yet
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaNo ratings yet
- Khosrowmomtaz 1998Document8 pagesKhosrowmomtaz 1998Mariana JuravleNo ratings yet
- Early Versus Late Surgery For Ileo-Caecal Crohn's Disease: Alimentary Pharmacology & TherapeuticsDocument10 pagesEarly Versus Late Surgery For Ileo-Caecal Crohn's Disease: Alimentary Pharmacology & TherapeuticsBernadett FarkasNo ratings yet
- Cancer of The EsophagusDocument6 pagesCancer of The EsophagusDileep SrinivasanNo ratings yet
- Gastrointestinal 132Document8 pagesGastrointestinal 132Minerva Medical Treatment Pvt LtdNo ratings yet
- 1627-Article Text-2378-1-10-20220708Document3 pages1627-Article Text-2378-1-10-20220708gfr9px8db6No ratings yet
- Narrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaDocument6 pagesNarrowband Ultraviolet-B Phototherapy in Pityriasis Lichenoides ChronicaJavier Perez ManriquezNo ratings yet
- Journal of Gastroenterology and Hepatology (2013)Document1 pageJournal of Gastroenterology and Hepatology (2013)Norberto MolloNo ratings yet
- MP CorticoadrenalesDocument13 pagesMP CorticoadrenalesJuan Torres MeleroNo ratings yet
- Glandula SalivarDocument8 pagesGlandula SalivarporsanimedNo ratings yet
- Adjuvant RadiotherapyDocument7 pagesAdjuvant Radiotherapyciko momonNo ratings yet
- Outpatient Rituximab, Ifosfamide, Etoposide (R-IE) in Patients Older Than 60 Years With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Who Are Not Candidates For Stem Cell TransplantationDocument8 pagesOutpatient Rituximab, Ifosfamide, Etoposide (R-IE) in Patients Older Than 60 Years With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Who Are Not Candidates For Stem Cell TransplantationAudrey DSNo ratings yet
- Gastric RTDocument10 pagesGastric RTLjupka Banar PoposkaNo ratings yet
- MedulloblastomaDocument3 pagesMedulloblastomaMohammadAwitNo ratings yet
- JFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisDocument2 pagesJFP - 1986 09 - v23 - I3 - A Case of Chronic AppendicitisBilalNo ratings yet
- JR Kemo TitaDocument21 pagesJR Kemo TitaTitaPuspitasariNo ratings yet
- Diificult AirwayDocument13 pagesDiificult AirwayBhi-An BatobalonosNo ratings yet
- A Retrospective Analysis On Treatment and Survival Outcome of Locally Advanced Cervical CancerDocument11 pagesA Retrospective Analysis On Treatment and Survival Outcome of Locally Advanced Cervical CancerdlledlycnNo ratings yet
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- Effectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceDocument10 pagesEffectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of the Quality of Community Satisfaction in Public Services in Tanjungpinang Class I State Detention HouseDocument13 pagesAnalysis of the Quality of Community Satisfaction in Public Services in Tanjungpinang Class I State Detention HouseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of the Effectiveness of Based Public Services Information and Communication Technology (ICT)Document10 pagesAnalysis of the Effectiveness of Based Public Services Information and Communication Technology (ICT)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Effects of Nanoplastics on Human Health: A Comprehensive StudyDocument7 pagesEffects of Nanoplastics on Human Health: A Comprehensive StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Anti-Diabetic Semaglutide: A GLP-1 RA PeptideDocument11 pagesOral Anti-Diabetic Semaglutide: A GLP-1 RA PeptideInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Zilebesiran: The First siRNA Drug Therapy for HypertensionDocument5 pagesZilebesiran: The First siRNA Drug Therapy for HypertensionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Analysis of Various Formwork SystemsDocument6 pagesDesign and Analysis of Various Formwork SystemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyDocument8 pagesNurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Association Between Gender and Depression Among College StudentsDocument4 pagesAssociation Between Gender and Depression Among College StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Salivary Diagnostics in Oral and Systemic Diseases - A ReviewDocument5 pagesSalivary Diagnostics in Oral and Systemic Diseases - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityDocument9 pagesShift from Traditional to Modern Building Concepts and Designs in Ringim Town: A Comparative Study of Aesthetics, Values, Functions and DurabilityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Environmental Sanitation – A Therapy for Healthy Living for Sustainable Development. A Case Study of Argungu Township Kebbi State, North Western NigeriaDocument15 pagesEnvironmental Sanitation – A Therapy for Healthy Living for Sustainable Development. A Case Study of Argungu Township Kebbi State, North Western NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Reintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveDocument1 pageReintegration of Dairy in Daily American Diets: A Biochemical and Nutritional PerspectiveInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- MSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyDocument6 pagesMSMEs and Rural Prosperity: A Study of their Influence in Indonesian Agriculture and Rural EconomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyDocument6 pagesEvaluation of Lateral and Vertical Gingival Displacement Produced by Three Different Gingival Retraction Systems using Impression Scanning: An in-Vivo Original StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesDocument5 pagesBiometric Security Systems Enhanced by AI: Exploring Concerns with AI Advancements in Facial Recognition and Other Biometric Systems have Security Implications and VulnerabilitiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Appraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateDocument12 pagesAppraisal of Nursing Care Received and it’s Satisfaction: A Case Study of Admitted Patients in Afe Babalola Multisystem Hospital, Ado Ekiti, Ekiti StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateDocument6 pagesOccupational Injuries among Health Care Workers in Selected Hospitals in Ogbomosho, Oyo StateInternational Journal of Innovative Science and Research Technology100% (1)
- Prevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyDocument4 pagesPrevalence of Microorganisms in UTI and Antibiotic Sensitivity Pattern among Gram Negative Isolates: A Cohort StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AI Robots in Various SectorDocument3 pagesAI Robots in Various SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)Document7 pagesAn Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Dynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnDocument3 pagesDynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dr. Joseph Stan DDS - Cosmetic Dentist & Dental Implant Specialist in Beverly Hills & Los Angeles, CADocument8 pagesDr. Joseph Stan DDS - Cosmetic Dentist & Dental Implant Specialist in Beverly Hills & Los Angeles, CAjosephstanddsNo ratings yet
- Managing OtitisDocument9 pagesManaging OtitisdanielguerinNo ratings yet
- Neonatal EmergenciesDocument21 pagesNeonatal EmergenciesRNo ratings yet
- Effect of Preterm Infant Massage by The Mother On The Mood of Mothers Having Preterm InfantsDocument10 pagesEffect of Preterm Infant Massage by The Mother On The Mood of Mothers Having Preterm InfantsopanocayNo ratings yet
- COVID-19 Vaccine Developers Oxford-AstraZeneca Linked To British Eugenics MovementDocument18 pagesCOVID-19 Vaccine Developers Oxford-AstraZeneca Linked To British Eugenics MovementOwen KingNo ratings yet
- Epidemiology of Parkinson'S Disease: SciencedirectDocument13 pagesEpidemiology of Parkinson'S Disease: SciencedirectAleja ToPaNo ratings yet
- Sickle Cell Anemia Control Program: (A Major Tribal Health Program of Gujarat)Document29 pagesSickle Cell Anemia Control Program: (A Major Tribal Health Program of Gujarat)Sutapa PawarNo ratings yet
- PI Ferinject PDFDocument2 pagesPI Ferinject PDFMostofa RubalNo ratings yet
- Subjective and Objective DataDocument9 pagesSubjective and Objective DatagraceNo ratings yet
- Quinn TJ, Langhorne P, Stott DJ (2011) - Barthel Index For Stroke Trials: Development, Properties, and Application. Stroke. 42: 1146-1151Document2 pagesQuinn TJ, Langhorne P, Stott DJ (2011) - Barthel Index For Stroke Trials: Development, Properties, and Application. Stroke. 42: 1146-1151Sausan Hana MaharaniNo ratings yet
- Clinical Guideline: Aminoglycoside: Recommendations For Use, Dosing and Monitoring Clinical GuidelineDocument16 pagesClinical Guideline: Aminoglycoside: Recommendations For Use, Dosing and Monitoring Clinical GuidelineVita LesielaNo ratings yet
- PerrobinDocument6 pagesPerrobinVicente RivanoNo ratings yet
- Bricks Intensive Reading - L2 - Word List BDocument16 pagesBricks Intensive Reading - L2 - Word List BNathaniel McleodNo ratings yet
- Gardasil VAERS Adverse ReactionsDocument1,824 pagesGardasil VAERS Adverse Reactionsmcdonald.rr100% (2)
- Nursingstaff: Annotated BibliographyDocument5 pagesNursingstaff: Annotated BibliographyAnnette BainesNo ratings yet
- Clinical Neurology and NeurosurgeryDocument8 pagesClinical Neurology and NeurosurgeryMasithaNo ratings yet
- Clinical Case Book MeDioStar 2018-11Document48 pagesClinical Case Book MeDioStar 2018-11medspa49No ratings yet
- Challenges and Opportunities of Clinical Pharmacy Services in Ethiopia: A Qualitative Study From Healthcare Practitioners' PerspectiveDocument7 pagesChallenges and Opportunities of Clinical Pharmacy Services in Ethiopia: A Qualitative Study From Healthcare Practitioners' Perspectivebekalu dessieNo ratings yet
- Allergic Rhinitis: Dr. Fauziah Henny, SP - THT-KLDocument14 pagesAllergic Rhinitis: Dr. Fauziah Henny, SP - THT-KLIsra AbdiNo ratings yet
- Project Proposal For PIMA Hospital Mansehra Prof Iqbal KhanDocument14 pagesProject Proposal For PIMA Hospital Mansehra Prof Iqbal KhanMuhmmad TahaNo ratings yet
- Liability and Consent FormDocument2 pagesLiability and Consent Formapi-19917129No ratings yet
- Essential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 3 PDFDocument1 pageEssential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 3 PDFMariam QaisNo ratings yet
- Bioanalysis NotesDocument7 pagesBioanalysis NoteskeerthiNo ratings yet
- 9007 - 9008 - Convercation For Cheking Vital Nurse (Diarrhea) - 3A S.TR KeperawatanDocument4 pages9007 - 9008 - Convercation For Cheking Vital Nurse (Diarrhea) - 3A S.TR Keperawatandiahpurnama dewiNo ratings yet
- Emergency and Disaster Nursing NewDocument42 pagesEmergency and Disaster Nursing Newlalufebrian hendika25No ratings yet
- NSSK Training Aug, 16Document3 pagesNSSK Training Aug, 16Chhote yadavNo ratings yet
- Preventing Hospital Infections Real World Problems Realistic Solutions 2Nd Edition Jennifer Meddings Download PDF ChapterDocument52 pagesPreventing Hospital Infections Real World Problems Realistic Solutions 2Nd Edition Jennifer Meddings Download PDF Chaptermary.schoonmaker770100% (11)