
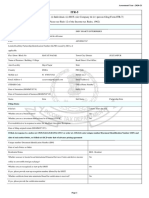
(For All Correspondence) : GSTIN/UIN Number of Client Communciation Address / Address of Regisered
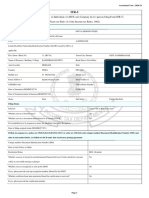
(For All Correspondence) : GSTIN/UIN Number of Client Communciation Address / Address of Regisered
You might also like
- Q3e RW Placement Test A TeacherDocument7 pagesQ3e RW Placement Test A TeacherLevent DemirelNo ratings yet
- Credit Insurance Simplified Questionnaire: Standard Payment Terms With Your Buyers (Measured in Days)Document8 pagesCredit Insurance Simplified Questionnaire: Standard Payment Terms With Your Buyers (Measured in Days)Venu Gopal SistlaNo ratings yet
- Aditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFDocument2 pagesAditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFHoaccounts AuNo ratings yet
- Aditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFDocument2 pagesAditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFHoaccounts AuNo ratings yet
- Annual KYC Updation Form - IndividualDocument2 pagesAnnual KYC Updation Form - IndividualJoy T100% (1)
- FATCA-CRS Declaration & Supplementary KYC Information: Declaration Form For EntitiesDocument6 pagesFATCA-CRS Declaration & Supplementary KYC Information: Declaration Form For Entitiesvikas9saraswatNo ratings yet
- DPR Existing Individual More Than 1 CRDocument57 pagesDPR Existing Individual More Than 1 CRarzNo ratings yet
- Awareness and Preference For Mutual FundsDocument3 pagesAwareness and Preference For Mutual Fundsamitnpatel1No ratings yet
- Doubt Session Ratios 120424Document51 pagesDoubt Session Ratios 120424pre.meh21No ratings yet
- Common Application Form For Etfs PDFDocument2 pagesCommon Application Form For Etfs PDFJami Anil Rasmikha mandanna Anil readsNo ratings yet
- BTC 2021 Form CSDocument40 pagesBTC 2021 Form CSisty5nnt100% (1)
- Banking Account Opening FormDocument12 pagesBanking Account Opening FormCassiane OgliariNo ratings yet
- UFCE FormatDocument2 pagesUFCE Formatytduyyuli yufyufNo ratings yet
- Form PDF 297846460200321Document63 pagesForm PDF 297846460200321anupam soniNo ratings yet
- Form PDF 168391951200919Document62 pagesForm PDF 168391951200919ashokbehera708No ratings yet
- Newsletter April 20 PDFDocument3 pagesNewsletter April 20 PDFSindhu Arauvinth RaajNo ratings yet
- Outlook Publishing (India) Private Limited: Summary of Rated InstrumentsDocument7 pagesOutlook Publishing (India) Private Limited: Summary of Rated InstrumentsKetan BhoiNo ratings yet
- Updated Vendor Selection Form V4Document14 pagesUpdated Vendor Selection Form V4Rommel BatayonNo ratings yet
- Fatca Form (1) (1) 1118-1266-5014-2191-0731-1231Document4 pagesFatca Form (1) (1) 1118-1266-5014-2191-0731-1231Harsh NarwareNo ratings yet
- Finance Derivative MarketDocument13 pagesFinance Derivative MarketTabrej AlamNo ratings yet
- Personal Notes: Business Finance 19-10-2020 Types of Business Categories 1. Sole ProprietorshipDocument18 pagesPersonal Notes: Business Finance 19-10-2020 Types of Business Categories 1. Sole ProprietorshipHijab ZaidiNo ratings yet
- Form PDF 156692990090121Document61 pagesForm PDF 156692990090121Deepika Darkhorse ProfessionalsNo ratings yet
- Us Model Financial Statements For StartupsDocument32 pagesUs Model Financial Statements For StartupsTusharNo ratings yet
- GP0766Document2 pagesGP0766Hans WongNo ratings yet
- 06-Projected Financial StatementsDocument7 pages06-Projected Financial StatementsMaria NisarNo ratings yet
- CH - 2 Accounting For Partnership Firms: Fundamentals: According To Section 4 of The Partnership Act 1932Document12 pagesCH - 2 Accounting For Partnership Firms: Fundamentals: According To Section 4 of The Partnership Act 1932Laksh KhannaNo ratings yet
- Company Tax Return 2020Document12 pagesCompany Tax Return 2020elenaNo ratings yet
- Supplementary KYC Information & FATCA-CRS Declaration - Entities & HUFDocument5 pagesSupplementary KYC Information & FATCA-CRS Declaration - Entities & HUFMohan TilakNo ratings yet
- Financial StatementsDocument8 pagesFinancial Statementsmanthansaini8923No ratings yet
- Divya Designo Tiles 201920 Itr - 1Document64 pagesDivya Designo Tiles 201920 Itr - 1Suman jhaNo ratings yet
- 14 - SS4 App CorpDocument3 pages14 - SS4 App CorprndvdbNo ratings yet
- Published AccountsDocument18 pagesPublished Accountskarangasharon909No ratings yet
- Fatca - NSDL Non Ind. V. 21.3 (PG 1-4)Document4 pagesFatca - NSDL Non Ind. V. 21.3 (PG 1-4)digitaltarun99No ratings yet
- Company Tax Return: 2017 (The Instructions), Available From The ATODocument12 pagesCompany Tax Return: 2017 (The Instructions), Available From The ATOhansolo1974No ratings yet
- Date of Valuation: Revenue Growth Rate For Next Year 4.00% Operating Margin For Next Year 30.00%Document62 pagesDate of Valuation: Revenue Growth Rate For Next Year 4.00% Operating Margin For Next Year 30.00%Pravin AwalkondeNo ratings yet
- Fcffsimpleginzu ITCDocument62 pagesFcffsimpleginzu ITCPravin AwalkondeNo ratings yet
- Study Material CH.-1 Fundamentals of Partnership 2023-24Document28 pagesStudy Material CH.-1 Fundamentals of Partnership 2023-24vsy9926No ratings yet
- Financial Ratios - Non Financial Sector - March2021Document11 pagesFinancial Ratios - Non Financial Sector - March2021karishmapatel93No ratings yet
- Proposal Form Credit Insurance: Your CompanyDocument2 pagesProposal Form Credit Insurance: Your Companyrahul sNo ratings yet
- Chapter 1 RatiosDocument81 pagesChapter 1 Ratiospaola sabbanNo ratings yet
- FFR 2 FormatDocument12 pagesFFR 2 FormatMukeshKataraNo ratings yet
- Advanced Financial Accounting - MB 711 Unit IIDocument59 pagesAdvanced Financial Accounting - MB 711 Unit IIGopi KrisnanNo ratings yet
- RCT Template 2022Document8 pagesRCT Template 2022glenb15cNo ratings yet
- Form PDF 196652130280722Document58 pagesForm PDF 196652130280722CA kundan kumarNo ratings yet
- Application For Employer Identification Number: Third Party DesigneeDocument2 pagesApplication For Employer Identification Number: Third Party DesigneeRemyan RNo ratings yet
- Finman MidsemDocument12 pagesFinman MidsemSHUBHAM NAHATANo ratings yet
- Chapter 6: Appropriation of Profits: Rohit AgarwalDocument4 pagesChapter 6: Appropriation of Profits: Rohit AgarwalbcomNo ratings yet
- Review: Corporate Finance FB5040Document62 pagesReview: Corporate Finance FB5040Koey TseNo ratings yet
- Application For Employer Identification Number: Third Party DesigneeDocument2 pagesApplication For Employer Identification Number: Third Party DesigneeKonstantinos KavafisNo ratings yet
- The Motley Fool's Rule Maker EssentialsDocument4 pagesThe Motley Fool's Rule Maker EssentialsnsadnanNo ratings yet
- CFR Answers Year 2015Document15 pagesCFR Answers Year 2015Ashwini SwamyNo ratings yet
- Itr Ay 2021Document57 pagesItr Ay 2021Suman jhaNo ratings yet
- Predicting and Preventing Corporate FailureDocument24 pagesPredicting and Preventing Corporate FailureleesadzebondeNo ratings yet
- Case Study FaDocument5 pagesCase Study Faabhishek ladhaniNo ratings yet
- Marico Final ProjectDocument49 pagesMarico Final ProjectRAHUL DAMNo ratings yet
- MediLab LLC SS-4Document1 pageMediLab LLC SS-4ashrafashash2010No ratings yet
- Fss 4Document2 pagesFss 4Russell Hartill100% (1)
- Form PDF 344472690310722Document11 pagesForm PDF 344472690310722NandhakumarNo ratings yet
- FATCA Non Individual FormDocument6 pagesFATCA Non Individual FormV RNo ratings yet
- Application For Employer Identification Number: Action Date SignatureDocument2 pagesApplication For Employer Identification Number: Action Date SignatureEl50% (2)
- Resolutions For Approval of Related Party TransactionsDocument3 pagesResolutions For Approval of Related Party TransactionsDinesh GadkariNo ratings yet
- Sample Contract Drafting ChecklistDocument6 pagesSample Contract Drafting ChecklistDinesh GadkariNo ratings yet
- How To Use Manupatra Effectively For Case Research Part 1Document4 pagesHow To Use Manupatra Effectively For Case Research Part 1Dinesh GadkariNo ratings yet
- How To Use Manupatra Effectively For Case Research Part 2Document8 pagesHow To Use Manupatra Effectively For Case Research Part 2Dinesh Gadkari100% (1)
- Loan Checklist - List of Compliances For A Loan TransactionDocument6 pagesLoan Checklist - List of Compliances For A Loan TransactionDinesh GadkariNo ratings yet
- How To Draft A Research Note and Legal OpinionDocument6 pagesHow To Draft A Research Note and Legal OpinionDinesh Gadkari100% (1)
- Corporate Law NotesDocument282 pagesCorporate Law NotesRaghav JainNo ratings yet
- Government of India Act 1919 - The Montague Chelmsford Reforms History IIDocument2 pagesGovernment of India Act 1919 - The Montague Chelmsford Reforms History IIDinesh Gadkari100% (1)
- Kinds of DirectorsDocument14 pagesKinds of DirectorsDinesh GadkariNo ratings yet
- CPJ 1st Sem History NotesDocument179 pagesCPJ 1st Sem History NotesDinesh GadkariNo ratings yet
- Modern Law of Insurance in India - K S N MURTHY and K V S SARMADocument573 pagesModern Law of Insurance in India - K S N MURTHY and K V S SARMADinesh Gadkari50% (2)
- Permenant CommissionDocument24 pagesPermenant CommissionDinesh GadkariNo ratings yet
- ENGIE, Crédit Agricole Assurances and Mirova Win Bid To Acquire 1.7 GW Hydroelectric Portfolio From EDP in PortugalDocument4 pagesENGIE, Crédit Agricole Assurances and Mirova Win Bid To Acquire 1.7 GW Hydroelectric Portfolio From EDP in Portugalvishal.nithamNo ratings yet
- Ms. Pamela Tikku (ICAT)Document30 pagesMs. Pamela Tikku (ICAT)NagaVenkateshGNo ratings yet
- Auxiliary Fire Service Act: Laws of Trinidad and TobagoDocument11 pagesAuxiliary Fire Service Act: Laws of Trinidad and TobagoMarlon FordeNo ratings yet
- HDFC Bank Statement 09-08-2022Document5 pagesHDFC Bank Statement 09-08-2022mahakaal digital point bhopalNo ratings yet
- IEEE Guide For Using IEEE STD 1547™ For Interconnection of Energy Storage Distributed Energy Resources With Electric Power SystemsDocument87 pagesIEEE Guide For Using IEEE STD 1547™ For Interconnection of Energy Storage Distributed Energy Resources With Electric Power Systemsbengisutuna42No ratings yet
- Silicon Carbide: Safety Data SheetDocument6 pagesSilicon Carbide: Safety Data SheetIkaPertiwiNo ratings yet
- Speed FanDocument26 pagesSpeed FanGeorgios PuliarekosNo ratings yet
- Information Technology Grade 7 - 9 Units of Work Draft June 2016Document146 pagesInformation Technology Grade 7 - 9 Units of Work Draft June 2016api-247871582100% (1)
- Muhamma D Asim: ObjectiveDocument2 pagesMuhamma D Asim: ObjectiveMuzaffar HussainNo ratings yet
- Navy Releases Final EIS For Growler Operations at NAS Whidbey IslandDocument2 pagesNavy Releases Final EIS For Growler Operations at NAS Whidbey IslandGrowlerJoeNo ratings yet
- NRLP - C - 129 - Grasshopper - 10 T - ZB - 556Document4 pagesNRLP - C - 129 - Grasshopper - 10 T - ZB - 556MohamedNo ratings yet
- Iaea Safety Guide No. Gs-g-1.4Document50 pagesIaea Safety Guide No. Gs-g-1.4FortunatoNo ratings yet
- Ministry of Energy - Overview T&T Petroleum Post IndependenceDocument11 pagesMinistry of Energy - Overview T&T Petroleum Post Independenceronnysingh1No ratings yet
- Theory of Opportunity CostsDocument35 pagesTheory of Opportunity CostsShagun SoodNo ratings yet
- Chocho Language - WikipediaDocument2 pagesChocho Language - Wikipediajjlajom0% (1)
- Mas QuizzerDocument11 pagesMas QuizzerNica Jane MacapinigNo ratings yet
- Health Safety CompetenceDocument11 pagesHealth Safety CompetenceJenecile ParambitaNo ratings yet
- Vacuum Cleaner Using Iot Base PaperDocument10 pagesVacuum Cleaner Using Iot Base Paper18351ec051No ratings yet
- 1619 Discretionary Bursary Award LetterDocument3 pages1619 Discretionary Bursary Award LetterMaria Guerrero troncosoNo ratings yet
- Fires & Fire Extinguishers: Name: - Class: - DateDocument12 pagesFires & Fire Extinguishers: Name: - Class: - DateArcherNo ratings yet
- Sept8 CabDocument4 pagesSept8 Cabaviral.mathurNo ratings yet
- Siemens Power Engineering Guide 7E 54Document1 pageSiemens Power Engineering Guide 7E 54mydearteacherNo ratings yet
- 6300.50 Intercambiadores RaypakDocument8 pages6300.50 Intercambiadores RaypakHector FajardoNo ratings yet
- 1 s2.0 S2590198222000197 MainDocument8 pages1 s2.0 S2590198222000197 MaindashakrezubNo ratings yet
- Important Monthly Current Affairs Capsule - February 2021: TelegramDocument142 pagesImportant Monthly Current Affairs Capsule - February 2021: TelegramDigvijaya SrivastavaNo ratings yet
- Calculation of Loads: 1. Self Weight of BoxDocument6 pagesCalculation of Loads: 1. Self Weight of BoxAshwani BindalNo ratings yet
- Director of Lands Vs CADocument11 pagesDirector of Lands Vs CAJoanna GaringNo ratings yet
- Review For The Fundamentals of Engineering ExamDocument20 pagesReview For The Fundamentals of Engineering Exammrspeakish100% (1)
- Work Book Day 1 (Continued !!)Document7 pagesWork Book Day 1 (Continued !!)Mithun VasanthaKumarNo ratings yet


































































































Download as pdf or txt
You might also like
- Q3e RW Placement Test A TeacherDocument7 pagesQ3e RW Placement Test A TeacherLevent DemirelNo ratings yet
- Credit Insurance Simplified Questionnaire: Standard Payment Terms With Your Buyers (Measured in Days)Document8 pagesCredit Insurance Simplified Questionnaire: Standard Payment Terms With Your Buyers (Measured in Days)Venu Gopal SistlaNo ratings yet
- Aditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFDocument2 pagesAditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFHoaccounts AuNo ratings yet
- Aditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFDocument2 pagesAditya Birla - FATCA and CRS - UBO - NON INDIVIDUALS PDFHoaccounts AuNo ratings yet
- Annual KYC Updation Form - IndividualDocument2 pagesAnnual KYC Updation Form - IndividualJoy T100% (1)
- FATCA-CRS Declaration & Supplementary KYC Information: Declaration Form For EntitiesDocument6 pagesFATCA-CRS Declaration & Supplementary KYC Information: Declaration Form For Entitiesvikas9saraswatNo ratings yet
- DPR Existing Individual More Than 1 CRDocument57 pagesDPR Existing Individual More Than 1 CRarzNo ratings yet
- Awareness and Preference For Mutual FundsDocument3 pagesAwareness and Preference For Mutual Fundsamitnpatel1No ratings yet
- Doubt Session Ratios 120424Document51 pagesDoubt Session Ratios 120424pre.meh21No ratings yet
- Common Application Form For Etfs PDFDocument2 pagesCommon Application Form For Etfs PDFJami Anil Rasmikha mandanna Anil readsNo ratings yet
- BTC 2021 Form CSDocument40 pagesBTC 2021 Form CSisty5nnt100% (1)
- Banking Account Opening FormDocument12 pagesBanking Account Opening FormCassiane OgliariNo ratings yet
- UFCE FormatDocument2 pagesUFCE Formatytduyyuli yufyufNo ratings yet
- Form PDF 297846460200321Document63 pagesForm PDF 297846460200321anupam soniNo ratings yet
- Form PDF 168391951200919Document62 pagesForm PDF 168391951200919ashokbehera708No ratings yet
- Newsletter April 20 PDFDocument3 pagesNewsletter April 20 PDFSindhu Arauvinth RaajNo ratings yet
- Outlook Publishing (India) Private Limited: Summary of Rated InstrumentsDocument7 pagesOutlook Publishing (India) Private Limited: Summary of Rated InstrumentsKetan BhoiNo ratings yet
- Updated Vendor Selection Form V4Document14 pagesUpdated Vendor Selection Form V4Rommel BatayonNo ratings yet
- Fatca Form (1) (1) 1118-1266-5014-2191-0731-1231Document4 pagesFatca Form (1) (1) 1118-1266-5014-2191-0731-1231Harsh NarwareNo ratings yet
- Finance Derivative MarketDocument13 pagesFinance Derivative MarketTabrej AlamNo ratings yet
- Personal Notes: Business Finance 19-10-2020 Types of Business Categories 1. Sole ProprietorshipDocument18 pagesPersonal Notes: Business Finance 19-10-2020 Types of Business Categories 1. Sole ProprietorshipHijab ZaidiNo ratings yet
- Form PDF 156692990090121Document61 pagesForm PDF 156692990090121Deepika Darkhorse ProfessionalsNo ratings yet
- Us Model Financial Statements For StartupsDocument32 pagesUs Model Financial Statements For StartupsTusharNo ratings yet
- GP0766Document2 pagesGP0766Hans WongNo ratings yet
- 06-Projected Financial StatementsDocument7 pages06-Projected Financial StatementsMaria NisarNo ratings yet
- CH - 2 Accounting For Partnership Firms: Fundamentals: According To Section 4 of The Partnership Act 1932Document12 pagesCH - 2 Accounting For Partnership Firms: Fundamentals: According To Section 4 of The Partnership Act 1932Laksh KhannaNo ratings yet
- Company Tax Return 2020Document12 pagesCompany Tax Return 2020elenaNo ratings yet
- Supplementary KYC Information & FATCA-CRS Declaration - Entities & HUFDocument5 pagesSupplementary KYC Information & FATCA-CRS Declaration - Entities & HUFMohan TilakNo ratings yet
- Financial StatementsDocument8 pagesFinancial Statementsmanthansaini8923No ratings yet
- Divya Designo Tiles 201920 Itr - 1Document64 pagesDivya Designo Tiles 201920 Itr - 1Suman jhaNo ratings yet
- 14 - SS4 App CorpDocument3 pages14 - SS4 App CorprndvdbNo ratings yet
- Published AccountsDocument18 pagesPublished Accountskarangasharon909No ratings yet
- Fatca - NSDL Non Ind. V. 21.3 (PG 1-4)Document4 pagesFatca - NSDL Non Ind. V. 21.3 (PG 1-4)digitaltarun99No ratings yet
- Company Tax Return: 2017 (The Instructions), Available From The ATODocument12 pagesCompany Tax Return: 2017 (The Instructions), Available From The ATOhansolo1974No ratings yet
- Date of Valuation: Revenue Growth Rate For Next Year 4.00% Operating Margin For Next Year 30.00%Document62 pagesDate of Valuation: Revenue Growth Rate For Next Year 4.00% Operating Margin For Next Year 30.00%Pravin AwalkondeNo ratings yet
- Fcffsimpleginzu ITCDocument62 pagesFcffsimpleginzu ITCPravin AwalkondeNo ratings yet
- Study Material CH.-1 Fundamentals of Partnership 2023-24Document28 pagesStudy Material CH.-1 Fundamentals of Partnership 2023-24vsy9926No ratings yet
- Financial Ratios - Non Financial Sector - March2021Document11 pagesFinancial Ratios - Non Financial Sector - March2021karishmapatel93No ratings yet
- Proposal Form Credit Insurance: Your CompanyDocument2 pagesProposal Form Credit Insurance: Your Companyrahul sNo ratings yet
- Chapter 1 RatiosDocument81 pagesChapter 1 Ratiospaola sabbanNo ratings yet
- FFR 2 FormatDocument12 pagesFFR 2 FormatMukeshKataraNo ratings yet
- Advanced Financial Accounting - MB 711 Unit IIDocument59 pagesAdvanced Financial Accounting - MB 711 Unit IIGopi KrisnanNo ratings yet
- RCT Template 2022Document8 pagesRCT Template 2022glenb15cNo ratings yet
- Form PDF 196652130280722Document58 pagesForm PDF 196652130280722CA kundan kumarNo ratings yet
- Application For Employer Identification Number: Third Party DesigneeDocument2 pagesApplication For Employer Identification Number: Third Party DesigneeRemyan RNo ratings yet
- Finman MidsemDocument12 pagesFinman MidsemSHUBHAM NAHATANo ratings yet
- Chapter 6: Appropriation of Profits: Rohit AgarwalDocument4 pagesChapter 6: Appropriation of Profits: Rohit AgarwalbcomNo ratings yet
- Review: Corporate Finance FB5040Document62 pagesReview: Corporate Finance FB5040Koey TseNo ratings yet
- Application For Employer Identification Number: Third Party DesigneeDocument2 pagesApplication For Employer Identification Number: Third Party DesigneeKonstantinos KavafisNo ratings yet
- The Motley Fool's Rule Maker EssentialsDocument4 pagesThe Motley Fool's Rule Maker EssentialsnsadnanNo ratings yet
- CFR Answers Year 2015Document15 pagesCFR Answers Year 2015Ashwini SwamyNo ratings yet
- Itr Ay 2021Document57 pagesItr Ay 2021Suman jhaNo ratings yet
- Predicting and Preventing Corporate FailureDocument24 pagesPredicting and Preventing Corporate FailureleesadzebondeNo ratings yet
- Case Study FaDocument5 pagesCase Study Faabhishek ladhaniNo ratings yet
- Marico Final ProjectDocument49 pagesMarico Final ProjectRAHUL DAMNo ratings yet
- MediLab LLC SS-4Document1 pageMediLab LLC SS-4ashrafashash2010No ratings yet
- Fss 4Document2 pagesFss 4Russell Hartill100% (1)
- Form PDF 344472690310722Document11 pagesForm PDF 344472690310722NandhakumarNo ratings yet
- FATCA Non Individual FormDocument6 pagesFATCA Non Individual FormV RNo ratings yet
- Application For Employer Identification Number: Action Date SignatureDocument2 pagesApplication For Employer Identification Number: Action Date SignatureEl50% (2)
- Resolutions For Approval of Related Party TransactionsDocument3 pagesResolutions For Approval of Related Party TransactionsDinesh GadkariNo ratings yet
- Sample Contract Drafting ChecklistDocument6 pagesSample Contract Drafting ChecklistDinesh GadkariNo ratings yet
- How To Use Manupatra Effectively For Case Research Part 1Document4 pagesHow To Use Manupatra Effectively For Case Research Part 1Dinesh GadkariNo ratings yet
- How To Use Manupatra Effectively For Case Research Part 2Document8 pagesHow To Use Manupatra Effectively For Case Research Part 2Dinesh Gadkari100% (1)
- Loan Checklist - List of Compliances For A Loan TransactionDocument6 pagesLoan Checklist - List of Compliances For A Loan TransactionDinesh GadkariNo ratings yet
- How To Draft A Research Note and Legal OpinionDocument6 pagesHow To Draft A Research Note and Legal OpinionDinesh Gadkari100% (1)
- Corporate Law NotesDocument282 pagesCorporate Law NotesRaghav JainNo ratings yet
- Government of India Act 1919 - The Montague Chelmsford Reforms History IIDocument2 pagesGovernment of India Act 1919 - The Montague Chelmsford Reforms History IIDinesh Gadkari100% (1)
- Kinds of DirectorsDocument14 pagesKinds of DirectorsDinesh GadkariNo ratings yet
- CPJ 1st Sem History NotesDocument179 pagesCPJ 1st Sem History NotesDinesh GadkariNo ratings yet
- Modern Law of Insurance in India - K S N MURTHY and K V S SARMADocument573 pagesModern Law of Insurance in India - K S N MURTHY and K V S SARMADinesh Gadkari50% (2)
- Permenant CommissionDocument24 pagesPermenant CommissionDinesh GadkariNo ratings yet
- ENGIE, Crédit Agricole Assurances and Mirova Win Bid To Acquire 1.7 GW Hydroelectric Portfolio From EDP in PortugalDocument4 pagesENGIE, Crédit Agricole Assurances and Mirova Win Bid To Acquire 1.7 GW Hydroelectric Portfolio From EDP in Portugalvishal.nithamNo ratings yet
- Ms. Pamela Tikku (ICAT)Document30 pagesMs. Pamela Tikku (ICAT)NagaVenkateshGNo ratings yet
- Auxiliary Fire Service Act: Laws of Trinidad and TobagoDocument11 pagesAuxiliary Fire Service Act: Laws of Trinidad and TobagoMarlon FordeNo ratings yet
- HDFC Bank Statement 09-08-2022Document5 pagesHDFC Bank Statement 09-08-2022mahakaal digital point bhopalNo ratings yet
- IEEE Guide For Using IEEE STD 1547™ For Interconnection of Energy Storage Distributed Energy Resources With Electric Power SystemsDocument87 pagesIEEE Guide For Using IEEE STD 1547™ For Interconnection of Energy Storage Distributed Energy Resources With Electric Power Systemsbengisutuna42No ratings yet
- Silicon Carbide: Safety Data SheetDocument6 pagesSilicon Carbide: Safety Data SheetIkaPertiwiNo ratings yet
- Speed FanDocument26 pagesSpeed FanGeorgios PuliarekosNo ratings yet
- Information Technology Grade 7 - 9 Units of Work Draft June 2016Document146 pagesInformation Technology Grade 7 - 9 Units of Work Draft June 2016api-247871582100% (1)
- Muhamma D Asim: ObjectiveDocument2 pagesMuhamma D Asim: ObjectiveMuzaffar HussainNo ratings yet
- Navy Releases Final EIS For Growler Operations at NAS Whidbey IslandDocument2 pagesNavy Releases Final EIS For Growler Operations at NAS Whidbey IslandGrowlerJoeNo ratings yet
- NRLP - C - 129 - Grasshopper - 10 T - ZB - 556Document4 pagesNRLP - C - 129 - Grasshopper - 10 T - ZB - 556MohamedNo ratings yet
- Iaea Safety Guide No. Gs-g-1.4Document50 pagesIaea Safety Guide No. Gs-g-1.4FortunatoNo ratings yet
- Ministry of Energy - Overview T&T Petroleum Post IndependenceDocument11 pagesMinistry of Energy - Overview T&T Petroleum Post Independenceronnysingh1No ratings yet
- Theory of Opportunity CostsDocument35 pagesTheory of Opportunity CostsShagun SoodNo ratings yet
- Chocho Language - WikipediaDocument2 pagesChocho Language - Wikipediajjlajom0% (1)
- Mas QuizzerDocument11 pagesMas QuizzerNica Jane MacapinigNo ratings yet
- Health Safety CompetenceDocument11 pagesHealth Safety CompetenceJenecile ParambitaNo ratings yet
- Vacuum Cleaner Using Iot Base PaperDocument10 pagesVacuum Cleaner Using Iot Base Paper18351ec051No ratings yet
- 1619 Discretionary Bursary Award LetterDocument3 pages1619 Discretionary Bursary Award LetterMaria Guerrero troncosoNo ratings yet
- Fires & Fire Extinguishers: Name: - Class: - DateDocument12 pagesFires & Fire Extinguishers: Name: - Class: - DateArcherNo ratings yet
- Sept8 CabDocument4 pagesSept8 Cabaviral.mathurNo ratings yet
- Siemens Power Engineering Guide 7E 54Document1 pageSiemens Power Engineering Guide 7E 54mydearteacherNo ratings yet
- 6300.50 Intercambiadores RaypakDocument8 pages6300.50 Intercambiadores RaypakHector FajardoNo ratings yet
- 1 s2.0 S2590198222000197 MainDocument8 pages1 s2.0 S2590198222000197 MaindashakrezubNo ratings yet
- Important Monthly Current Affairs Capsule - February 2021: TelegramDocument142 pagesImportant Monthly Current Affairs Capsule - February 2021: TelegramDigvijaya SrivastavaNo ratings yet
- Calculation of Loads: 1. Self Weight of BoxDocument6 pagesCalculation of Loads: 1. Self Weight of BoxAshwani BindalNo ratings yet
- Director of Lands Vs CADocument11 pagesDirector of Lands Vs CAJoanna GaringNo ratings yet
- Review For The Fundamentals of Engineering ExamDocument20 pagesReview For The Fundamentals of Engineering Exammrspeakish100% (1)
- Work Book Day 1 (Continued !!)Document7 pagesWork Book Day 1 (Continued !!)Mithun VasanthaKumarNo ratings yet