Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Gem Elixiers and Vibrational Healing Vol I & II 1985 - GurudasDocument422 pagesGem Elixiers and Vibrational Healing Vol I & II 1985 - GurudasTe voy a contarNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Review Notes in Pharmacology - NCLEXDocument1 pageReview Notes in Pharmacology - NCLEXLalaine April E. Ortiola79% (29)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Online High School OM013: Honors Precalculus With TrigonometryDocument2 pagesOnline High School OM013: Honors Precalculus With TrigonometryJin SiclonNo ratings yet
- Qa Practice Reflection Worksheet Sem2Document1 pageQa Practice Reflection Worksheet Sem2api-315256143No ratings yet
- JSA - Repair-Coating and Finition WorkDocument3 pagesJSA - Repair-Coating and Finition WorkAMIN100% (1)
- Xecutive Ummary: Work Sharing During The Great RecessionDocument4 pagesXecutive Ummary: Work Sharing During The Great RecessionJin SiclonNo ratings yet
- Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and NutritionDocument116 pagesEssential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and NutritionJin SiclonNo ratings yet
- Informal Employment in Namibia 2008Document68 pagesInformal Employment in Namibia 2008Jin SiclonNo ratings yet
- Tendencias Mundiales Empleo - 2013 - OIT (Inglés)Document172 pagesTendencias Mundiales Empleo - 2013 - OIT (Inglés)David Velázquez SeiferheldNo ratings yet
- Social Protection Floor For A Fair and Inclusive GlobalizationDocument150 pagesSocial Protection Floor For A Fair and Inclusive GlobalizationSalam Salam Solidarity (fauzi ibrahim)No ratings yet
- 2012 06 Statistical Update v2Document28 pages2012 06 Statistical Update v2Jin SiclonNo ratings yet
- Decent Work Indicators - Concepts and DefinitionsDocument170 pagesDecent Work Indicators - Concepts and DefinitionsJin SiclonNo ratings yet
- Decent Work Indicators in Africa - A First Assessment Based On National SourcesDocument160 pagesDecent Work Indicators in Africa - A First Assessment Based On National SourcesJin SiclonNo ratings yet
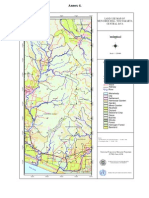
- Annex 4.: Land Use Map of Menoreh Hill-Yogyakarta Central JavaDocument1 pageAnnex 4.: Land Use Map of Menoreh Hill-Yogyakarta Central JavaJin SiclonNo ratings yet
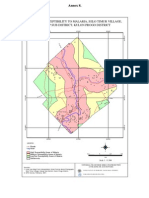
- Maps of Susceptibility To Malaria, Selo Timur Village, Kokap Sub District, Kulon Progo DistrictDocument1 pageMaps of Susceptibility To Malaria, Selo Timur Village, Kokap Sub District, Kulon Progo DistrictJin SiclonNo ratings yet
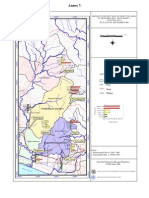
- Annex 7Document1 pageAnnex 7Jin SiclonNo ratings yet
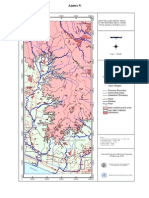
- Annex 9.: Most Malaria Prone Areas in The Menoreh Hills ( 200M) - Yogyakarta Central JavaDocument1 pageAnnex 9.: Most Malaria Prone Areas in The Menoreh Hills ( 200M) - Yogyakarta Central JavaJin SiclonNo ratings yet
- Annex 6.: Beyond The Study Area River Road Railway Case Village NgemplakDocument1 pageAnnex 6.: Beyond The Study Area River Road Railway Case Village NgemplakJin SiclonNo ratings yet
- Annex 5Document1 pageAnnex 5Jin SiclonNo ratings yet
- Product OsDocument29 pagesProduct OsCristian LaraNo ratings yet
- Basic Science Techniques in Clinical Practice (PDFDrive)Document162 pagesBasic Science Techniques in Clinical Practice (PDFDrive)Isah MohammedNo ratings yet
- MOHAMMED Health Passport 05-11-2022 1.1Document1 pageMOHAMMED Health Passport 05-11-2022 1.1EXPERTISE STORENo ratings yet
- 10 Herbs For Cleansing Ur KidneysDocument8 pages10 Herbs For Cleansing Ur KidneysHussainz AliNo ratings yet
- Akshata Sawant Final Article 1Document16 pagesAkshata Sawant Final Article 1SonuNo ratings yet
- Fukuoka Kinen HospitalDocument23 pagesFukuoka Kinen HospitaldihcsarNo ratings yet
- American College Sports Medicine Strength Training and Responses in BeginnersDocument9 pagesAmerican College Sports Medicine Strength Training and Responses in BeginnersMohd Syafiq HasriNo ratings yet
- UGT1A1 Allele Definition TableDocument7 pagesUGT1A1 Allele Definition TableElizaDiasNo ratings yet
- IMEC Series IntroductionDocument49 pagesIMEC Series IntroductionNicolas NeffaNo ratings yet
- Stock 6 Juni 2023Document42 pagesStock 6 Juni 2023Faishal Adi CandraNo ratings yet
- The Most Effective Natural Cures On Earth - Johnny BowdenDocument257 pagesThe Most Effective Natural Cures On Earth - Johnny BowdenLewis John33% (3)
- MSH Ehandbook CompleteDocument446 pagesMSH Ehandbook CompleteNaweed Miakhel100% (1)
- Managing Medicine SelectionDocument25 pagesManaging Medicine SelectionShoaib BiradarNo ratings yet
- Evolution in Health and Disease 2nd Stearns Koella PDFDocument1 pageEvolution in Health and Disease 2nd Stearns Koella PDFJenniferNo ratings yet
- Ethics in Pediatric Patient CareDocument12 pagesEthics in Pediatric Patient CareTiwi QiraNo ratings yet
- SR Phonares II Tooth Mould ChartDocument8 pagesSR Phonares II Tooth Mould ChartSomnath SenguptaNo ratings yet
- Relevance and Treatment of Coccidiosis in Domestic Pigeons (Columba Livia Forma Domestica) With Particular Emphasis On ToltrazurilDocument6 pagesRelevance and Treatment of Coccidiosis in Domestic Pigeons (Columba Livia Forma Domestica) With Particular Emphasis On ToltrazurilAnonymous tBJwSUSjNo ratings yet
- How To Study Quickly and Effectively - 1. IntroductionDocument3 pagesHow To Study Quickly and Effectively - 1. IntroductionfuzzychanNo ratings yet
- TestyDocument21 pagesTestyNa ClNo ratings yet
- Giving Back To Gondwana Concert ProgramDocument24 pagesGiving Back To Gondwana Concert ProgramanguswoodsNo ratings yet
- BP605TPDocument1 pageBP605TPsd1596823No ratings yet
- VenoferinfDocument10 pagesVenoferinfzerin_atinNo ratings yet
- Power Point Environmental CleaningDocument60 pagesPower Point Environmental CleaningPrapitta AnindyaNo ratings yet
- Dexmedetomidine Expanding Role in AnesthesiaDocument9 pagesDexmedetomidine Expanding Role in AnesthesiaUnggul Yudha100% (1)
- Jurnal IlmiahDocument8 pagesJurnal IlmiahDeni Ratna Juwita IINo ratings yet
- Analgesics: AnticonvulsantsDocument8 pagesAnalgesics: AnticonvulsantsGina Giammalvo100% (1)