Download as pdf or txt
You might also like
- Congenital Muscular Torticollis CMT: By:Dr. Zakir Uk (DPT, MSPT, Kmu) Edited By: Sabar Jamila & Sabar MinaDocument35 pagesCongenital Muscular Torticollis CMT: By:Dr. Zakir Uk (DPT, MSPT, Kmu) Edited By: Sabar Jamila & Sabar Minasyge zwvuNo ratings yet
- Torticollis III BPTDocument31 pagesTorticollis III BPTKASTURI COLLEGENo ratings yet
- Deformities of The SpineDocument112 pagesDeformities of The SpineZunairaNo ratings yet
- CMT MacDocument24 pagesCMT MacChidube UkachukwuNo ratings yet
- Tort Ikol IsDocument8 pagesTort Ikol IsAde CornellisNo ratings yet
- DysrafismDocument44 pagesDysrafismdeealoveadyNo ratings yet
- Congenital Torticollis and Its Physiotherapy Management: Simranjeet KaurDocument8 pagesCongenital Torticollis and Its Physiotherapy Management: Simranjeet KaurEka Wahyu HerdiyantiNo ratings yet
- Tortikolis Muskular Kongenital: Imelda E. Kawatu Engeline AngliadiDocument7 pagesTortikolis Muskular Kongenital: Imelda E. Kawatu Engeline AngliadisayidaffanNo ratings yet
- Congenital Muscular TorticollisDocument29 pagesCongenital Muscular Torticolliskashmala afzal100% (1)
- Help Pedsurgeryafrica38Document6 pagesHelp Pedsurgeryafrica38madalinamihailescuNo ratings yet
- An Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15Document24 pagesAn Osteopathic Approach To Torticollis Plagiocephaly and Otitis Media 2014-15johnNo ratings yet
- Congenital Muscular TorticollisDocument5 pagesCongenital Muscular TorticollisKevin Paul ZuñigaNo ratings yet
- TorticollisDocument86 pagesTorticollisSylvia LoongNo ratings yet
- Pediatric Spine MRI: Occult Spinal DysraphismsDocument5 pagesPediatric Spine MRI: Occult Spinal DysraphismsSilma FarrahaNo ratings yet
- Congenital Muscular TorticolisDocument12 pagesCongenital Muscular TorticolistesfahuntekletilahunNo ratings yet
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Birth InjuriesDocument13 pagesBirth InjuriesLekshmi Manu100% (1)
- Torticolis-Dr P K SahooDocument4 pagesTorticolis-Dr P K SahooRabiaNo ratings yet
- Torticollis ٠٥١٥٢٠Document31 pagesTorticollis ٠٥١٥٢٠nagmxxmNo ratings yet
- Lecture 6 Congenital Bone DisorderDocument100 pagesLecture 6 Congenital Bone DisorderWilson HalimNo ratings yet
- Cervical Myelopathy ColumbiaDocument5 pagesCervical Myelopathy ColumbiarosalinaNo ratings yet
- The Effects of Kinesio Taping Method in Treatment of Congenital Torticollis Case StudiesDocument13 pagesThe Effects of Kinesio Taping Method in Treatment of Congenital Torticollis Case StudiesAna Lu LoboNo ratings yet
- Tort Ikol IsDocument1 pageTort Ikol IsAhmad SabiqNo ratings yet
- Day 14 NCM 109 FE AdolescentDocument57 pagesDay 14 NCM 109 FE AdolescentSheena Patricia ArasulaNo ratings yet
- MyelomeningoceleDocument14 pagesMyelomeningoceleLiliana Bazan CabanillasNo ratings yet
- Overview Congenital Musculoskeletal DisorderDocument84 pagesOverview Congenital Musculoskeletal DisorderRyan Trian100% (3)
- Neural Tube Defects: Dr.M.G.Kartheeka Fellow in Neonatology Cloudnine, OARDocument36 pagesNeural Tube Defects: Dr.M.G.Kartheeka Fellow in Neonatology Cloudnine, OARM G KARTHEEKANo ratings yet
- Imaging in Acute Torticollis NXPowerLiteDocument41 pagesImaging in Acute Torticollis NXPowerLiteOktaviana Sari DewiNo ratings yet
- DR - Tehreem NasirDocument29 pagesDR - Tehreem NasirAhmed SaeedNo ratings yet
- Congenital Muscular TorticollisDocument15 pagesCongenital Muscular TorticollisAhmedAbdelZaherNo ratings yet
- Torticolis 2009Document12 pagesTorticolis 2009fernando gonzalezNo ratings yet
- Scoliosis: Prepared By: Mary Ann AtienzaDocument13 pagesScoliosis: Prepared By: Mary Ann Atienzamhean azneitaNo ratings yet
- Tethered Spinal Cord Syndrome Is A Neurological Disorder Caused by Tissue Attachments That Limit The Movement of The Spinal Cord Within The Spinal ColumnDocument9 pagesTethered Spinal Cord Syndrome Is A Neurological Disorder Caused by Tissue Attachments That Limit The Movement of The Spinal Cord Within The Spinal ColumnSitaNo ratings yet
- Brachial Plexus InjuryDocument20 pagesBrachial Plexus InjurySuci PramadianiNo ratings yet
- Clinical Practice: The Spine From Birth To AdolescenceDocument6 pagesClinical Practice: The Spine From Birth To Adolescencechristian roblesNo ratings yet
- PEDIATRIA RadiologíaDocument17 pagesPEDIATRIA RadiologíaDavid ReyesNo ratings yet
- Congenital TorticollisDocument40 pagesCongenital TorticollisNamakau MuliloNo ratings yet
- Paediatric Guidelines TorticollisDocument4 pagesPaediatric Guidelines TorticollisCatalin ChiriloiNo ratings yet
- Erb'S Palsy: Definition/DescriptionDocument10 pagesErb'S Palsy: Definition/DescriptionGuhan SubramaniamNo ratings yet
- PALSYDocument10 pagesPALSYGuhan SubramaniamNo ratings yet
- Infantile Torticollis: Brief DiscussionDocument36 pagesInfantile Torticollis: Brief DiscussionchinmayghaisasNo ratings yet
- Birth InjuryDocument35 pagesBirth InjurySanjay Kumar SanjuNo ratings yet
- Differential Diagnosis of Shoulder RegionDocument96 pagesDifferential Diagnosis of Shoulder RegionZuhaib AhmedNo ratings yet
- MSKII Case Study PresentationDocument18 pagesMSKII Case Study PresentationMart Joseph SenoNo ratings yet
- CP PresentationDocument35 pagesCP PresentationdrsourabhsinghNo ratings yet
- Pediatric OrthopaedicDocument66 pagesPediatric OrthopaedicDhito RodriguezNo ratings yet
- Birth TraumaDocument18 pagesBirth TraumaJemmy SieNo ratings yet
- Dr. Samir - Paediatric SpineDocument33 pagesDr. Samir - Paediatric SpinelertegimluNo ratings yet
- Cervical SpondylosisDocument10 pagesCervical Spondylosistaufiq duppa duppaaNo ratings yet
- Spina BifidaDocument33 pagesSpina BifidaRegine Prongoso DagumanpanNo ratings yet
- 3 5 4 B TorticollisDocument20 pages3 5 4 B TorticollisPratama IkoNo ratings yet
- Birthinjuries Dr.M.maniDocument65 pagesBirthinjuries Dr.M.manimaniNo ratings yet
- Congenital Muscular Torticollis: DefinitionDocument7 pagesCongenital Muscular Torticollis: DefinitionMona LitaNo ratings yet
- Brachial Plexus Asia inDocument19 pagesBrachial Plexus Asia inFajrin GumilarNo ratings yet
- Brachial Plexus Injury in Neonates: Lourdes Asiain February 2005Document19 pagesBrachial Plexus Injury in Neonates: Lourdes Asiain February 2005i4u88No ratings yet
- Abdul Hakeem Hady.: Done byDocument29 pagesAbdul Hakeem Hady.: Done byعمر احمد شاكرNo ratings yet
- Neural Tube DefectDocument8 pagesNeural Tube DefectReema Akberali nooraniNo ratings yet
- Tortikolis: Tinjauan PustakaDocument9 pagesTortikolis: Tinjauan PustakaMaulidyaNo ratings yet
- Twisted Neck, (Torticollis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTwisted Neck, (Torticollis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A PT With Fever and CoughDocument2 pagesA PT With Fever and CoughCharl UnalNo ratings yet
- A PT With Pleuritic Chest PainDocument2 pagesA PT With Pleuritic Chest PainCharl UnalNo ratings yet
- 5 Drug EruptionsDocument50 pages5 Drug EruptionsCharl UnalNo ratings yet
- A PT With AnemiaDocument2 pagesA PT With AnemiaCharl UnalNo ratings yet
- 4 Perthes Ve SCFEDocument34 pages4 Perthes Ve SCFECharl UnalNo ratings yet
- Sjögren's Syndrome: Berivan Bitik, MDDocument22 pagesSjögren's Syndrome: Berivan Bitik, MDCharl UnalNo ratings yet
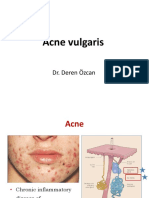
- 8 Acne Vulgaris and RosaceaDocument35 pages8 Acne Vulgaris and RosaceaCharl UnalNo ratings yet
- AFP Brochure08Document4 pagesAFP Brochure08YongoloooNo ratings yet
- Mix Design C 35A - 50%Document1 pageMix Design C 35A - 50%cecbNo ratings yet
- 0802 - MEA, PS, B, C, D, F, G, H, I, J, K, L, M, N, P, Q, R, S, X & MEY - E+H - Final - HSDocument8 pages0802 - MEA, PS, B, C, D, F, G, H, I, J, K, L, M, N, P, Q, R, S, X & MEY - E+H - Final - HSnityasoni121724No ratings yet
- Bed Shukla JiDocument1 pageBed Shukla JiCYBERZONE COMPUTERSNo ratings yet
- Blulock Spec SheetDocument2 pagesBlulock Spec Sheetapi-36492444No ratings yet
- Dim Sum Chicken FeetDocument2 pagesDim Sum Chicken FeetDevon DocenaNo ratings yet
- Orif ReportDocument5 pagesOrif ReportduypalaNo ratings yet
- 2.transmission Line Theory PDFDocument89 pages2.transmission Line Theory PDFSara AhmedNo ratings yet
- Final ReportDocument8 pagesFinal ReportZack GroothouseNo ratings yet
- Bayesian-Statistics Final 20140416 3Document38 pagesBayesian-Statistics Final 20140416 3muralidharanNo ratings yet
- Dr. Reddy's Laboratories: Performance HighlightsDocument10 pagesDr. Reddy's Laboratories: Performance HighlightsAngel BrokingNo ratings yet
- 2024 NM Consultative Meeting For PMNP MPMOsDocument31 pages2024 NM Consultative Meeting For PMNP MPMOssribaccayNo ratings yet
- Macro Curriculum Changes 2023 Part 2Document6 pagesMacro Curriculum Changes 2023 Part 2Al VelNo ratings yet
- Package Dimension (Qcc8C) : WWW - Datasheet.Co - KR WWW - Datasheet.Co - KRDocument3 pagesPackage Dimension (Qcc8C) : WWW - Datasheet.Co - KR WWW - Datasheet.Co - KRindustronicaNo ratings yet
- PDF 1Document36 pagesPDF 1kehidupankucing5No ratings yet
- KatalogDocument3 pagesKatalogJosua Sahat Parulian SinagaNo ratings yet
- Ashik v. Bandula and Others (Noise Pollution Case)Document7 pagesAshik v. Bandula and Others (Noise Pollution Case)Huzaifa SalimNo ratings yet
- Planning Considerations For Ice PlantsDocument5 pagesPlanning Considerations For Ice PlantsribozymesNo ratings yet
- Chapter 4Document8 pagesChapter 4Coursehero Premium0% (1)
- Causes of MeanderingDocument1 pageCauses of MeanderingBalagopal V50% (2)
- Low Cost Mechatronics Prototype Prosthesis For Transfemoral Amputation Controled by Myolectric SignalsDocument6 pagesLow Cost Mechatronics Prototype Prosthesis For Transfemoral Amputation Controled by Myolectric SignalsElizabeth CominaNo ratings yet
- 2.1 Boilers: Classification of BoilerDocument5 pages2.1 Boilers: Classification of BoilerManjunatha EikilaNo ratings yet
- Formulation of An Integrated River Basin Management and Development Master Plan For Marikina River Basin Volume 1: Executive SummaryDocument71 pagesFormulation of An Integrated River Basin Management and Development Master Plan For Marikina River Basin Volume 1: Executive SummaryDexter CaroNo ratings yet
- Stability CosmeticDocument47 pagesStability CosmeticAgustin E SetiowatiNo ratings yet
- Find RoommateDocument2 pagesFind RoommateAyaz QaiserNo ratings yet
- Bata Bata Pano Ka GinawaDocument1 pageBata Bata Pano Ka GinawaVivien BernosNo ratings yet
- May 2014Document48 pagesMay 2014debtwiggNo ratings yet
- Declaration Good Health Form PDFDocument2 pagesDeclaration Good Health Form PDFMurali SiddarthNo ratings yet
- PEHLA 20031beDocument16 pagesPEHLA 20031beLê Tuấn AnhNo ratings yet
- Torque Values RTJ (B16.5)Document3 pagesTorque Values RTJ (B16.5)ariyamanjulaNo ratings yet